
Abstract
Abstract
Background:
Single-incision laparoscopic cholecystectomy (SILC) is theoretically supposed to be associated with better cosmetic results and less surgical-site pain than multi-incision laparoscopic cholesystectomy (MILC). So far, several relevant randomized controlled trials (RCTs) have been reported, but the results are conflicting.
Materials and Methods:
Meta-analysis was conducted with all the qualified RCTs comparing SILC with MILC. The databases include PubMed, EmBase, and the Cochrane Library, and the censor data were collected up to November 2011. The analyzed outcome variables included postoperative pain score, analgesia requirements, morbidity, conversion rate, operative time, postoperative hospital stay, and postoperative cosmetic score. Analyses were based on the intention-to-treat principle, if possible. All the calculations and statistical tests were performed using ReviewerManager version 5.1.2 software.
Results:
Nine trials with a total of 755 patients (SILC in 400 patients, MILC in 355 patients) were identified and analyzed. SILC resulted in significantly longer operative time (P=.005) and higher postoperative cosmetic score on Day 30 after operation (P<.00001). There was no statistically significant difference between the groups in terms of postoperative pain score, analgesia requirements, morbidity, conversion rate, and postoperative hospital stay.
Conclusions:
Based on the current meta-analysis, SILC appears to be as safe and effective as MILC to remove the gallbladder and results in a longer operative time and higher cosmetic satisfaction on Day 30 after surgery.
Introduction
Materials and Methods
Inclusion and exclusion criteria
This meta-analysis included only RCTs that aimed to compare SILC with MILC. SILC could be performed by laparoscopic instruments and endoscopic ones, 13 which is also called laparoendoscopic single-site surgery or single-incision endoscopic surgery. Our meta-analysis included trials performing SILC with laparoscopic instruments and ones addressing the surgical technique with endoscopic instruments. All studies that were included needed to report at least one of the following outcome measures: postoperative pain score, analgesia requirements, morbidity, conversion rate, operative time, postoperative hospital stay, and cosmetic score. Reviews, case reports, retrospective analyses, and quasirandomized trials were excluded. For duplicate publications, the smaller dataset was excluded.
Search strategy
We conducted a comprehensive search to identify all published relevant RCTs by searching the following electronic databases—PubMed, EmBase, and the Cochrane Library—up to November 2011. The search strategy used for this review was a combination of MeSH and text words related to LC and single incision. To identify RCTs, we combined the search words with the search filters, such as “randomized controlled trials” or “controlled clinical trials,” as recommended by the Cochrane Handbook for Systematic Reviews of Interventions 14 and the limitation function in the PubMed database. For example, the search strategy for PubMed used the strings (single-port OR single-trocar OR single-incision OR 1-port OR 1-trocar OR 1-incision OR single port OR single trocar OR single incision OR 1 port OR 1 trocar OR 1 incision OR one-port OR one-trocar OR one-incision OR one port OR one trocar OR one incision) AND “cholecystectomy, laparoscopic” (MeSH Terms), limited to RCT. Furthermore, reference lists of all retrieved articles were manually searched for additional studies.
Types of outcome measures analyzed
The seven outcome variables analyzed included (1) postoperative pain score; (2) analgesia requirements; (3) morbidity; (4) conversion rate; (5) operative time; (6) postoperative hospital stay; and (7) postoperative cosmetic score.
Data extraction and assessment of risk of bias
Data were extracted from each study by three independent reviewers (J.-H.L., M.-L.L., and J.-S.M.). The reviewers also evaluated the risk of bias using the Cochrane Handbook for Systematic Reviews of Interventions. 15 The assessment is based on sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. Agreement was achieved through discussion when necessary.
Statistical analysis
Statistical analysis was performed using ReviewerManager (version 5.1.2, 2011; The Nordic Cochrane Centre, Cochrane Collaboration; www.cochrane-handbook.org). The statistical method was referred to the Cochrane Handbook for Systematic Reviews of Interventions. 16 Heterogeneity was checked using a chi-squared test, and P<.01 was considered significant. If there was no statistically significant heterogeneity, a fixed-effect model was used. If the results of trials had heterogeneity, a random-effects model was applied for meta-analysis. Data from different trials reporting the same or similar outcomes were combined. The result was expressed with odds ratio (OR) for binary variables and with mean difference (MD) or standard MD (SMD) for continuous variables. P<.05 was considered statistically significant, and the 95% confidence interval (CI) is presented for each effect measure. According to Cochrane Handbook for Systematic Reviews of Interventions 16 the standard deviation can be calculated on the assumptions that both groups have the same variance, and this may not be true. Therefore, a sensitivity analysis was performed by excluding the trials in which the standard deviation was not available for continuous outcomes. All analyses were based on the intention-to-treat principle, if possible. An available case analysis was also performed for sensitivity analysis. Publication bias exploration using a funnel plot and Egger's regression method 17 was performed, when at least 10 trials were included in this study.
Results
Description of the included trials
From the 241 records received from the electronic database, nine trials10–13,18–22 were included in the meta-analysis after checking for eligibility. No records were identified through other sources. The other articles were excluded mainly because of irrelevant topics. Figure 1 shows the flowchart for selection of articles according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 23 In total, 755 patients were randomized to either SILC (n=400 patients) or MILC (n=355). There were no statistically significant differences in the demographic characteristics, including age, gender, body mass index (BMI), and preoperative diagnosis, except for one trial 19 with a significant difference in age between two groups and another trials 10 with a significant difference in BMI. The basic data, including sample size, age, intervention, available outcomes, and supportive technique for gallbladder retraction, are presented in Table 1.
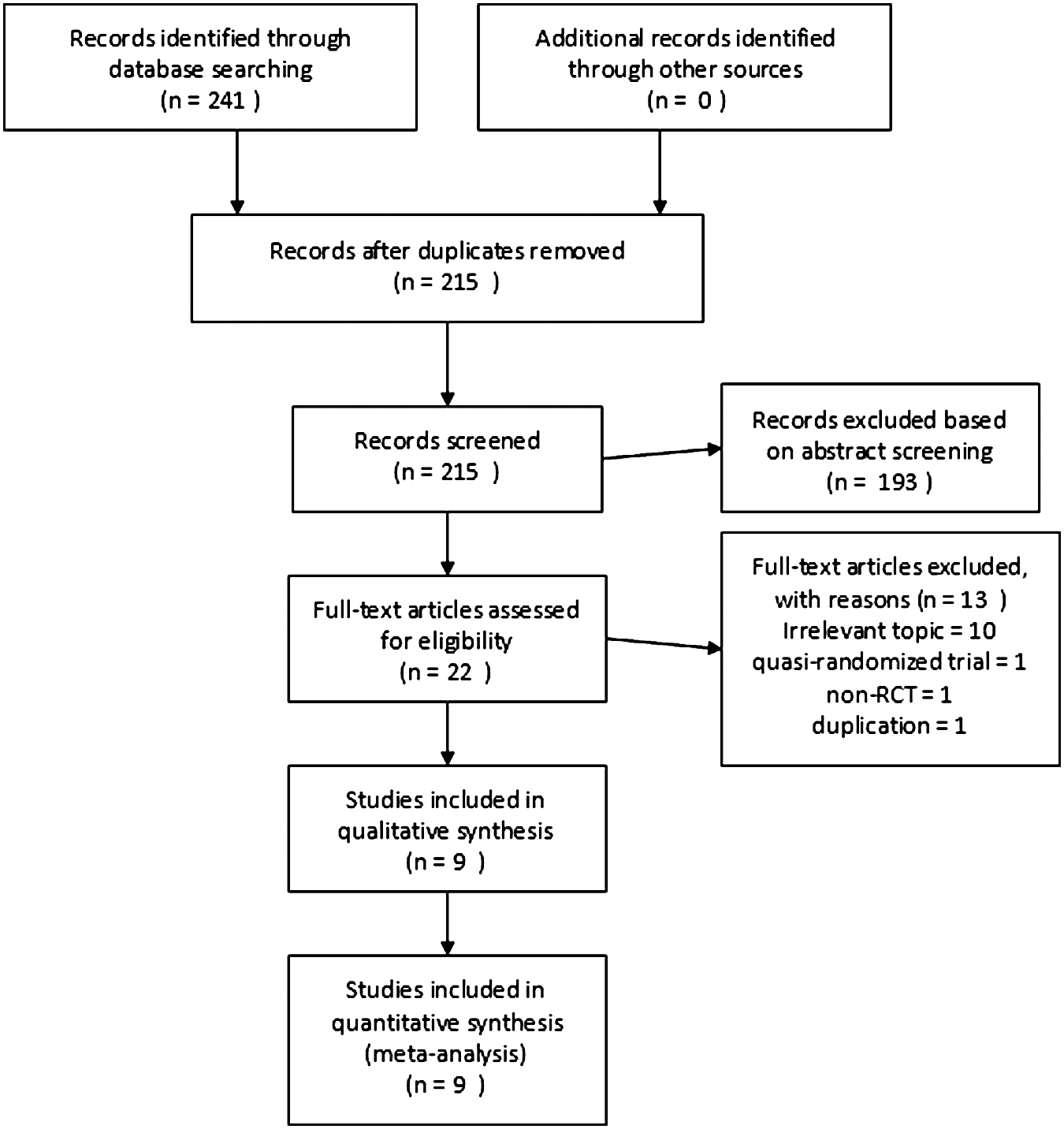
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart showing study selection process. RCT, randomized controlled trial.
LC, laparoscopic cholecystectomy; LESS, laparoendoscopic single-site surgery; MILS, multi-incision laparoscopic cholecystectomy; SILC, single-incision laparoscopic cholecystectomy.
Risk of bias
The risk of bias is summarized in Figure 2. All nine trials had a high risk of bias. Six trials10–13,20,22 failed to provide any details about randomization, and two studies19,21 did not specify the allocation concealment. Eight trials11–13,18–22 failed to blind the patients, and three trials10,13,19 did not blind the outcome assessors. It is widely known that the inability to blind participants and especially surgeons to surgical interventions is a common limitation in surgical research. 24 With taking into account the fact that some outcome variables analyzed in this meta-analysis are based on subject judgment, we consider these trials as high risk for blinding bias. One trial 10 had patients excluded after randomization and lost in follow-up. They did not make calculations based on the intention to treat. Therefore, we considered this trial as high risk in attrition bias. We failed to identify protocol of four trials,11,13,20,22 and thus these four were considered as unknown risk for selective bias. In two trials,10,19 there were significant differences in demographic features between the two groups. Both of these trials were considered as high risk for other bias.
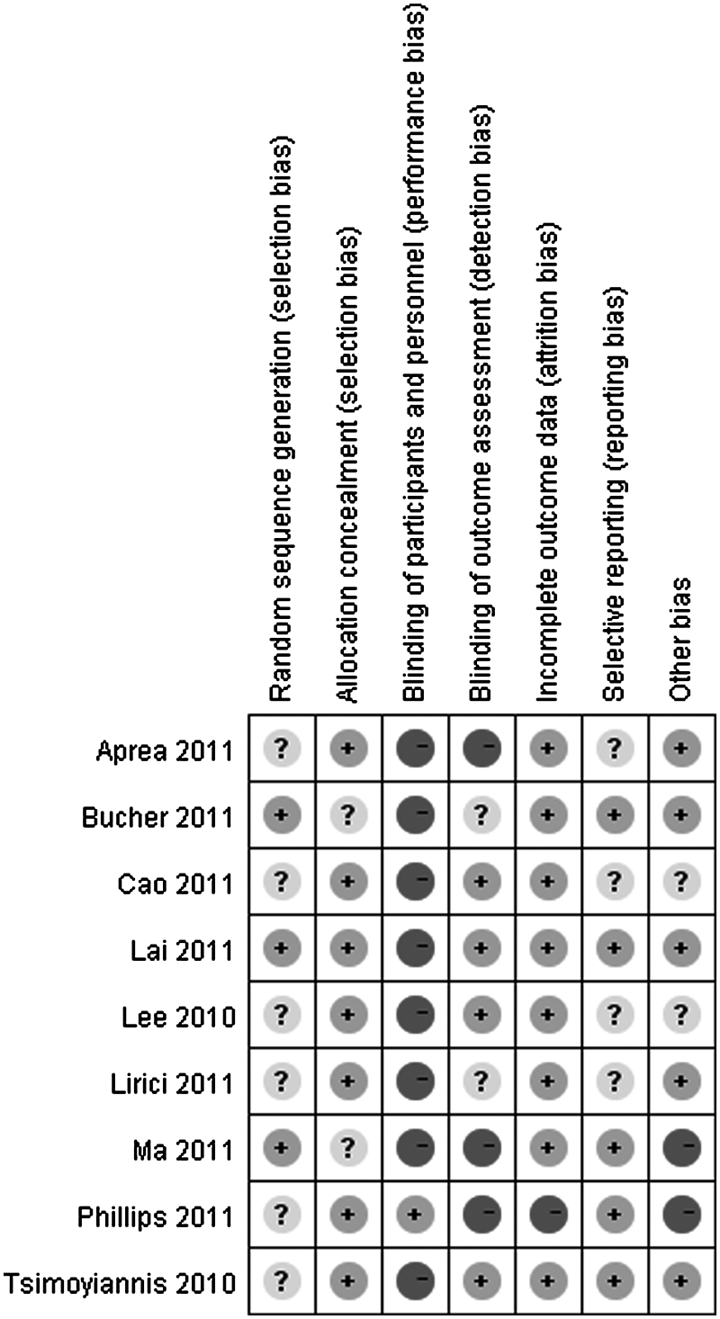
Risk of bias summary: review authors' judgments about the risk of bias for each of the nine included studies.
Postoperative pain score
All nine trials mentioned postoperative pain score, and eight10–13,19–22 of them provided enough details for meta-analysis. All the eight RCTs used visual analog pain score, but one 20 failed to describe it in detail. Therefore, SMD was calculated for pain score. Among these eight trials, one 19 was excluded because the researchers evaluated the pain score on the day of discharge and postoperative visit, and no details were provided about the exact day. Seven trials10–13,20–22 reported the pain score on postoperative Day 1, and three10,12,20 reported the results on Day 3. Heterogeneities were found, and thus the random-effects model was used. SILC was indicated in association with insignificant lower pain score than MILC on postoperative Day 1 (SMD −0.40; 95% CI −1.06 to 0.27; P=.24; Fig. 3) and Day 3 (SMD −0.47; 95% CI −1.34 to 0.41; P=.30; Fig. 4). The other two excluded trials also reported no significant difference between two groups, except one trial 18 found that patients in the SILC group suffered significantly more pain on postoperative Day 7 (P=.048).
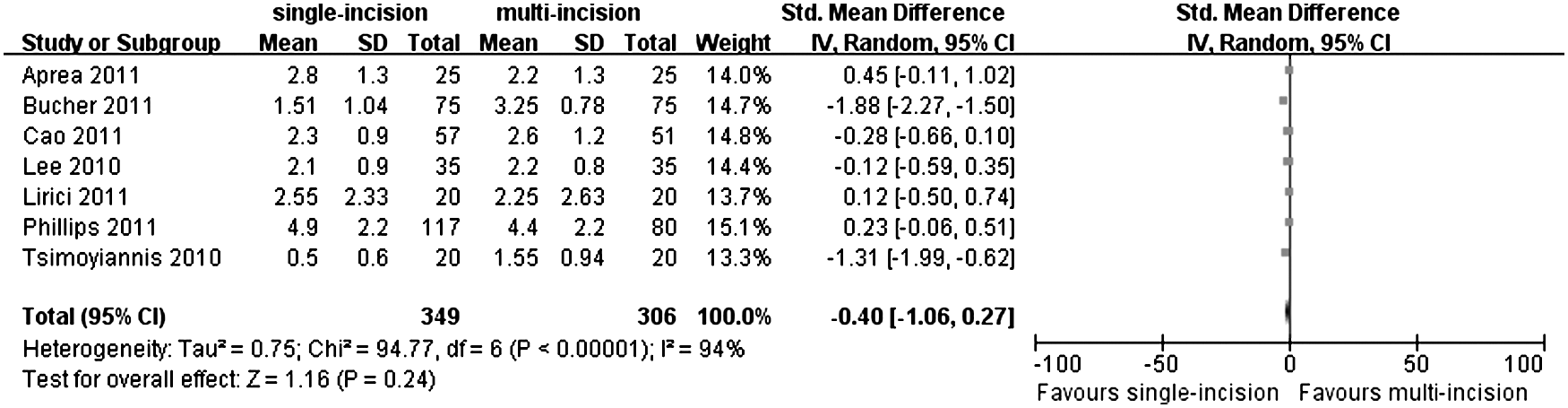
Forest plot for pain score on postoperative Day 1 showing single-incision laparoscopic cholecystectomy in association with insignificantly lower pain score than multi-incision laparoscopic cholecystectomy. CI, confidence interval; SD, standard deviation; IV, inverse variance.

Forest plot for pain score on postoperative Day 3 showing single-incision laparoscopic cholecystectomy in association with insignificantly lower pain score than multi-incision laparoscopic cholecystectomy. CI, confidence interval; SD, standard deviation.
Analgesia requirements
Five trials10–12,21,22 mentioned analgesia requirements, and three11,12,21 provided enough details. They adopted different types of drugs for analgesia. Heterogeneity was found, and thus the random-effects model with SMD was used. There was no significant difference between the two groups with an SMD of −0.49 (95% CI −1.22 to 0.24; P=.19) (Fig. 5).

Forest plot for postoperative analgesia requirements showing no difference between the procedures. CI, confidence interval; SD, standard deviation.
Morbidity
Six trials10,11,18–21 provided specific information about operation-related morbidity. No heterogeneity was found, and thus the fixed-effects model was used. Based on intention-to-treat analysis, 69 patients among the 335 in the SILC group suffered different complications, whereas 42 among the 290 patients in the MILC group developed various complications with an OR of 1.38 (95% CI 0.87–2.17; P=.17; Fig. 6), which demonstrates that there was no significant difference between the two groups in terms of morbidity. This result did not alter on the basis of available case analysis.
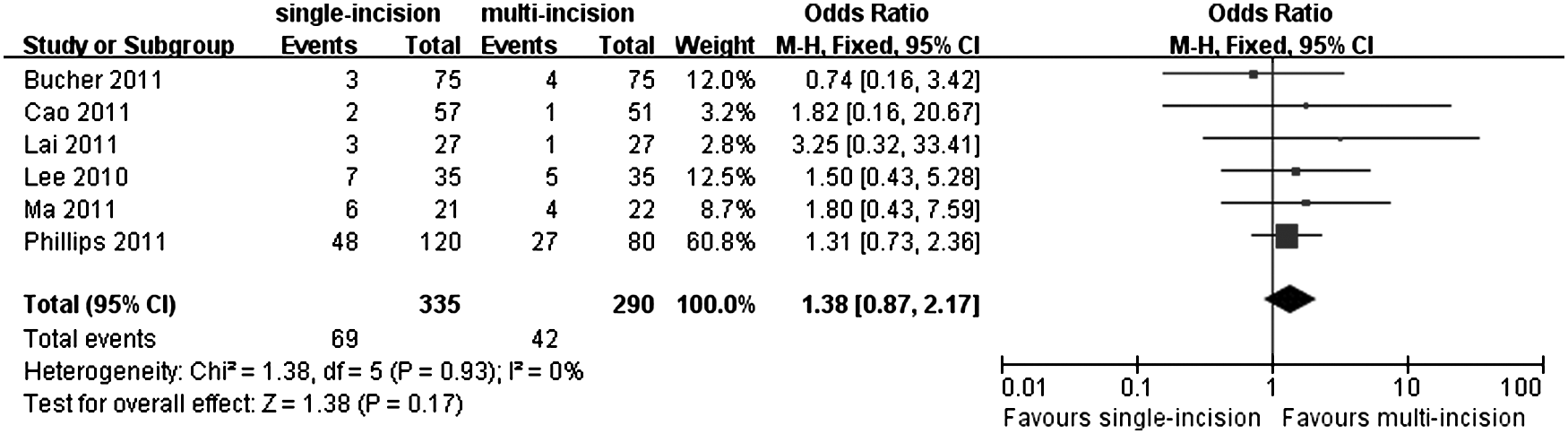
Forest plot for postoperative morbidity showing single-incision laparoscopic cholecystectomy in association with insignificantly higher morbidity rate than multi-incision laparoscopic cholecystectomy. CI, confidence interval; M-H, Mantel–Haenszel.
Conversion rate
Six trials10,11,18–20,22 mentioned conversion rate. No heterogeneity was found, and thus the fixed-effects model was used. Based on intention-to-treat analysis, the SILC group did not increase conversion rate significantly more than the MILC group with an OR of 3.00 (95% CI 0.95–9.45; P=.06; Fig. 7). Meanwhile, this result was not altered after we performed an available case analysis (P=.43).
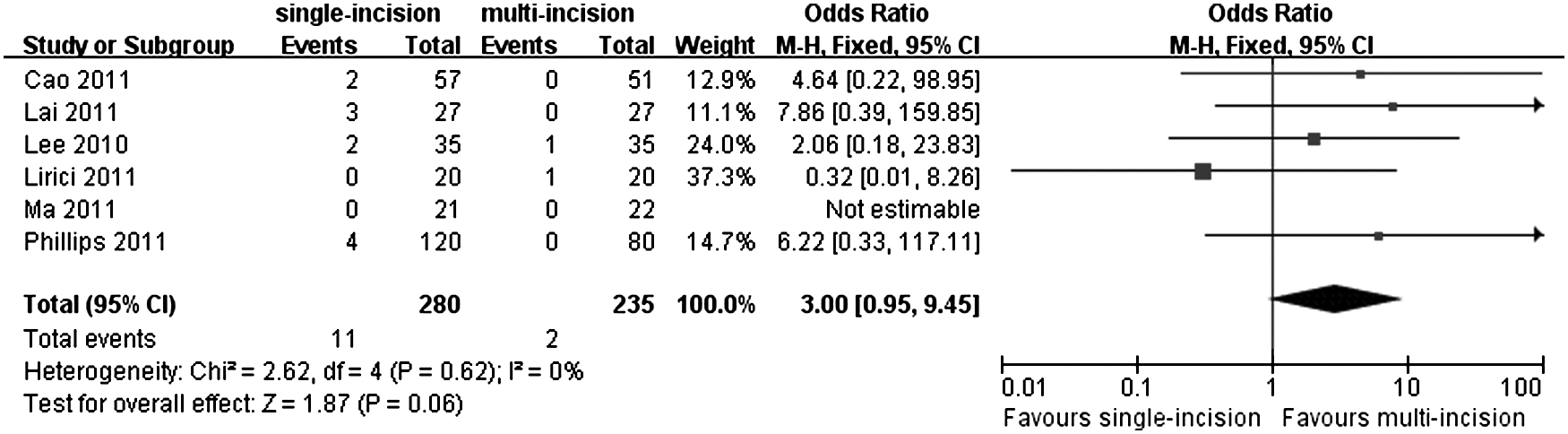
Forest plot for conversion rate showing showing single-incision laparoscopic cholecystectomy in association with insignificantly higher conversion rate than multi-incision laparoscopic cholecystectomy. CI, confidence interval; M-H, Mantel–Haenszel.
Operative time
All nine trials mentioned results about operative time, and eight11–13,18–22 of them provided enough details about operative time. Heterogeneity was found, and thus the random-effects model with MD was used. The SILC took significant longer time to perform the procedure than the MILC group (MD of 10.69; 95% CI 3.28–18.11; P=.005; Fig. 8). A sensitivity analysis was performed by excluding one trial, 19 and it did not alter the results. SILC still requires significantly more time than MILC (MD of 8.55; 95% CI 1.30–15.80; P=.02).
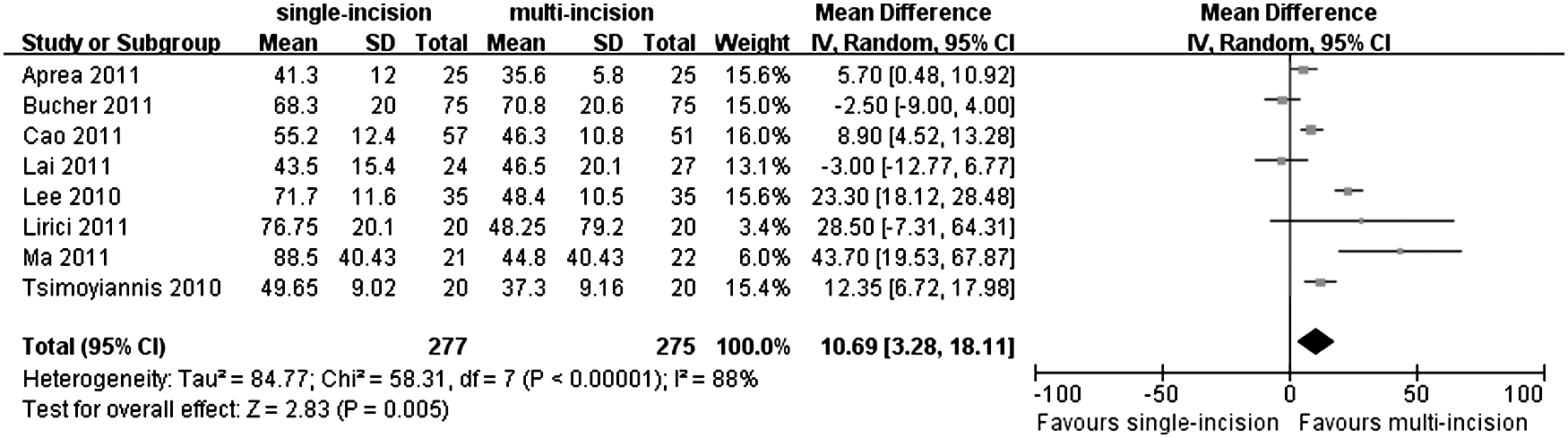
Forest plot for operative time favoring multi-incision laparoscopic cholecystectomy requiring less operative time. CI, confidence interval; SD, standard deviation.
Postoperative hospital stay
Seven trials11–13,18,20–22 reported results about postoperative hospital stay. Heterogeneity was found, and thus the random-effects model with MD was used. There was no significant difference between the SILC and MILC group in terms of postoperative hospital stay (MD of −0.40; 95% CI −0.81 to 0.01; P=.06; Fig. 9).
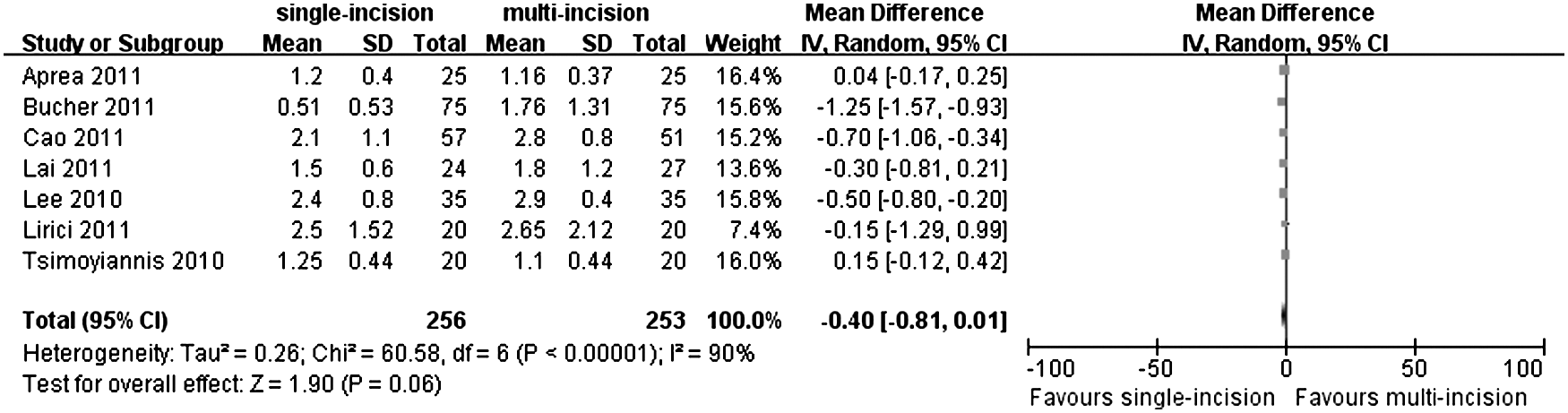
Forest plot for postoperative hospital stay showing no difference between the procedures. CI, confidence interval; SD, standard deviation.
Postoperative cosmetic score
Seven trials10,11,13,18,19,21,22 reported scar satisfaction scores at different time points after surgery, and the most commonly used one is 1 month after operation. Therefore, we meta-analyzed the cosmetic score by pooling the data at 1 month, and three studies10,11,22 were included. Different scales were applied in these trials. Heterogeneity was not found, and thus the fixed-effects model with SMD was used. The SILC was favored with significant higher cosmetic score on Day 30 after surgery than the MILC group (SMD of 0.84; 95% CI 0.60–1.09; P<.00001; Fig. 10).

Forest plot for postoperative cosmetic score, favoring single-incision laparoscopic cholecystectomy with higher cosmetic score. CI, confidence interval; SD, standard deviation.
Discussion
This systematic review with meta-analysis of RCTs suggests that SILC is as safe and effective as MILC to remove the gallbladder and results in a longer operative time and higher cosmetic satisfaction on Day 30 after surgery.
During the era of laparoscopic surgery, less postoperative pain and early recovery are major goals for achieving better patient care and cost-effectiveness. However, in the current study, no statistically significant difference was detected between the SILC and MILC groups in terms of postoperative pain on both postoperative Day 1 and Day 3. Only two12,21 trials reported a significant lower pain score in the SILC group, whereas all the other trials failed to show any significant reduction of pain in SILC. It is interesting that one trial 18 from Hong Kong found that patients in the SILC group suffered greater pain on postoperative Day 7 and that another trial 10 from the United States showed that SILC was associated with significantly more pain on postoperative Day 3 and Day 5. This is different from the presumption that SILC provides patients with less trauma and postoperative pain. Several reasons may contribute to this difference. First, the increasing size of the port incision, which is larger than that of the conventional subumbilical incision, may offset the advantage of reducing the number of ports and even cause more postoperative pain.18,19 Second, intraoperative bile leakage due to gallbladder rupture during the suturing or retraction is a main reason for abdominal pain after removal of the gallbladder. 11 Third, imbalance in the baseline of age may lead to different pain score results because older patients reported much more pain and discomfort than younger ones. 19
Visual analog pain scores are subjective outcomes and thus might be inaccurate. 25 Therefore, the results of analgesia requirements, which were relatively objective, were also pooled in this study. Only three trials provided enough details, and their results were conflicting. One trial 21 found the SILC group consumed less analgesia than the MILC group. In the other trials,11,12 no significant difference was found. These results agreed with the pain score results from another perspective. However, it should be pointed out that the analgesia requirement is not as objective as we think. The unblinding of patients about the procedure performed could potentially lead to a bias when they determined whether or not analgesia was needed.
Compared with MILC, SILC is technically more demanding and thus would presumably be associated with more postoperative complication, higher conversion rate, and longer operative time. This current study failed to detect any difference between the SILC and MILC groups in terms of complication and conversion rate on the intention-to-treat analysis. Operative time was significantly longer in the SILC group. All of the six included trials10,11,18–21 did not report any difference regarding complication. These results were similar to those of other retrospective studies.26,27 However, these results should be interpreted with caution. Five of the included trials11,12,18,19,21 were aiming to detect the difference in pain score, not complication rate. Because complications in LC are rare, much larger numbers of patients were needed to be involved to determine the long-term safety parameters. In the current study, only one included trial 10 was intending to evaluate the safety with a sample size target of 200 patients, and there was no significant difference in their results in terms of total complication. Therefore, the results regarding complication in this review might be underpowered, and the available evidence might not be sufficient to evaluate the relationship between SILC and morbidity. To study this correlation from a more accurate perspective, more rigorously designed studies with a large sample size are needed in the future. Moreover, five included trials11–13,19,20 reported SILC was associated with significantly longer operative time, whereas the other three did not. Besides the technical difficulty, the learning curve may contribute to the difference in operative time. As defined by previous studies,28,29 a learning curve of 5–10 cases was required before the operative time reached a plateau. Conversely, according to the study by Hernandez et al., 30 a significant reduction in surgical times was identified with the experience of a single surgeon after completion of 75 SILC procedures. In the included trials, four10,11,18,21 mentioned the number of SILCs performed before they started their RCTs, ranging from 5 to 50, and consequently two10,11 of them reported significantly longer operative time with SILC. It is interesting that one 18 of the included trials even found that SILC took less operative time than conventional MILC (mean±standard deviation, 43.5±15.4 versus 46.5±20.1 minutes; P=.716), although the difference was not significant. This may partially suggest that it is the surgical experience, not the technique itself, that caused longer operative time.
A significantly higher cosmetic satisfaction at Day 30 after operation was shown with SILC in the current study. Two10,11 of the pooled trials detected a significant difference between two groups favoring SILC, whereas the other 22 failed to detect this. SILC is an important step towards the goal of being scarless and cosmetic satisfaction. The umbilicus is the natural scar at the abdominal wall, and the umbilical access is a well-known and standardized site for access to the abdominal cavity for laparoscopy. 31 Therefore, the careful reconstruction of the umbilicus and the percutaneous stitch used in some trials for gallbladder suspension yields a completely invisible scar. 12 This may be the reason SILC has drawn so much attention all around the world.
During the preparation of this article, a meta-analysis 32 with 375 involved patients comparing single-incision laparoscopic surgery with conventional multiport cholecystectomy was reported. Only four outcome measures were analyzed, and their results were similar with ours. The current study included more RCTs with more patients, and seven outcome measures were analyzed. Therefore, our review can be considered as an updated meta-analysis on SILC.
Meta-analysis and systematic review are considered the best methods of summarizing the existing evidence, but the quality of such reviews relies on the quality of the primary studies, which may lead to bias and clinical heterogeneity and also may potentially distort our results.33,34 Possible sources of bias and limitations of this review are discussed below.
This current study has included a small number of trials. In most included trials, randomization processes were unclear, and there was no blinding for patients. Although blinding is difficult to perform in surgical trials, subjective outcomes, including pain scores and cosmetic scores, can be open to bias, which could be possibly avoided in future trials by blinding the outcome assessors and patients. Also, attrition bias was noticed in some trials. Publication bias detection was not performed because of the small number of included trials, although it was planned. Definitions of outcome parameters varied or even were not mentioned, which could cause heterogeneity for the outcomes such as operative time and postoperative hospital stay.
Heterogeneity was found between the included trials in terms of several outcomes, such as pain score and analgesia requirements, which were important outcome variables in the current study. Perioperative pain reduction managements applied differed in the included trials. Preincisional local infiltration plus intraperitoneal infusion of ropivacaine at the beginning of LC, combined with normal saline infusion at the end of the procedure, has been proven as a valid way of postoperative pain relief. 35 Only one trial 12 applied this method, whereas another one 10 injected 5 mL of 1% bupivacaine hydrochloride and epinephrine (Marcaine®) into the skin around each incision at the conclusion of the procedure. In addition, postoperative pain reduction managements were different among the included trials. One trial 11 gave patients oral paracetamol four times a day routinely, whereas the others did not. These differences could possibly cause heterogeneity and impair the reliability of these results.
In one trial, 10 BMI was higher in the MILC group (P=.011), and their results indicated that SILC required more operative time and led more wound complication. But, the total adverse events were similar between the two groups. Theoretically, high BMI usually means a great deal of abdominal fat and consequently surgical difficulty. Although according to different studies36–39 higher BMI was not a prognostic factor of more complication and longer hospital stay for LC, some studies38,39 indicated being overweight and obesity correlated with longer duration of surgery. Therefore, from a more conservative perspective, this included trial 10 was considered as having high risk of bias.
Conclusions
This review currently provides the best available evidence for comparison of SILC versus MILC. No evidence was found for SILC in which the procedure would result in less operative pain than MILC. Until further evidence from RCTs with a low risk of bias and a large sample size becomes available, SILC appears to be as safe and effective as MILC although associated with a longer operative time and better cosmetic satisfaction on Day 30 after surgery.
Footnotes
Disclosure Statement
No competing financial interest exists.