
Abstract
Abstract
Introduction:
Although laparoscopic major hepatectomy has frequently been performed, laparoscopic right anterior sectionectomy (Lap-RAS) has rarely been reported. In this report, we present three cases of totally Lap-RAS and the relevant technical maneuvers in each step of this procedure.
Patients and Methods:
Case 1 was that of a 40-year-old man who was admitted with abnormal intrahepatic bile duct dilatation containing multiple intrahepatic duct stones in S8. Preoperative imaging studies revealed the possibility of localized Caroli's disease. Case 2 was that of a 63-year-old woman who was admitted with hepatic masses detected by follow-up computed tomography scan for breast cancer. At first, these masses were suspected to be hepatic metastasis from breast cancer for which she had undergone right lumpectomy with axillary lymph node dissection, 1 year before. However, subsequent ultrasonographic biopsy showed a pathologic finding of hepatocellular carcinoma. Case 3 was that of a 54-year-old woman who was admitted for a hepatic mass noted on a health screening test, 2 weeks before. Imaging studies showed that a 2.7-cm-sized single mass was located in the border of S5 and S8, and the laboratory studies were positive for hepatitis B viral markers.
Results:
Operative times for Cases 1, 2, and 3 were 680, 600, and 540 minutes, respectively, and estimated blood loss during operations was 120, 400, and 500 mL, respectively. Intraoperative transfusion was not necessary. Patients 1, 2, and 3 were discharged on postoperative Days 30, 7, and 8, respectively.
Conclusions:
Lap-RAS is feasible for selected patients with benign and malignant liver disease, although the operative technique is still demanding.
Introduction
From an oncologic point of view, anatomic liver resection has been advocated as the recommended treatment in hepatocellular carcinoma (HCC). This procedure has been reported to offer several benefits, including obtaining safe surgical margins, reducing intraoperative blood loss, and improving the survival rate by complete resection of the tumor-bearing portal pedicles and corresponding liver parenchyma.5–7 Patients with HCC usually have concomitant chronic liver disease or liver cirrhosis, which may predispose to liver failure postoperatively. Therefore it is advantageous to preserve as much volume as possible to reduce the risk of postoperative hepatic failure. In this sense, anatomic right anterior sectionecomy would be one of the appropriate treatment options for patients who have tumors that are limited to the right anterior section. However, right anterior sectionectomy for HCC has been scarcely reported even in conventional open liver resection. The main reason for this is that right anterior sectionectomy is more technically demanding because it has two transection planes, and the surgeon will frequently encounter numerous branches from the in- and outflowing blood vessels of the remnant liver. 8
In this article, we report three totally laparoscopic right anterior sectionectomy (Lap-RAS) procedures. To our knowledge, these are the first reported cases that were totally performed via a laparoscopic procedure.
Case Reports
Case 1
A 40-year-old man was admitted to the hospital because of cystic mass in the liver. He had undergone a cholecystectomy at another hospital 6 months before, and follow-up imaging study revealed a cystic mass of the liver. During preoperative work-up, this cystic mass was diagnosed as localized Caroli's disease with intraductal multiple stones. The patient had no history of chronic liver disease or viral hepatitis. His physical examinations were unremarkable except for small incisions due to previous laparoscopic cholecystectomy. The preoperative liver function was normal. Abdominal computed tomography (CT) and magnetic resonance imaging (MRI) revealed a cystic lesion in S8 with stones. The preoperative diagnosis for the cystic mass was localized Caroli's disease. Lap-RAS was performed for the lesion.
Case 2
A 63-year-old woman was admitted to the hospital because of newly detected liver masses on the postoperative 1-year follow-up imaging studies for infiltrating ductal adenocarcinoma of the right breast. These lesions were presumed in the initial diagnosis to be metastatic tumors, but further imaging studies favored diagnosis of HCC. The patient was a chronic hepatitis C virus carrier. Her physical examinations were unremarkable. The preoperative liver function was Child–Pugh Class A, and the other laboratory studies, including the alpha-fetoprotein level, were normal. Abdominal CT and MRI showed two HCCs at S8 and the border of S4/8. Ultrasonography-guided gun biopsy was done for the mass lesion at the border of S4/8, and pathology of that tumor reported it to be HCC. An Lap-RAS was performed.
Case 3
A 54-year-old woman was admitted to the hospital for a hepatic mass that was incidentally found on a health screening test. She was a chronic hepatitis B virus carrier without any history of other diseases. The physical examination was unremarkable. The laboratory studies showed a normal alpha-fetoprotein level. The preoperative liver function was graded as Child–Pugh Class A. Abdominal CT and MRI revealed a 2.7-cm-sized single nodular tumor that was located in the superior portion of S5 (in the border of S5 and S8), and the lateral aspect of the tumor was in contact with the middle hepatic vein. The preoperative diagnosis was HCC. An Lap-RAS was performed.
Operative technique
Under general anesthesia, the patient was placed in the lithotomy position with a right-side-up adjustment (45° semilateral supine position). After the creation of a 12-mm umbilical port, a pneumoperitoneum was made with insufflation of CO2, and the intra-abdominal pressure was maintained below 12 mm Hg. A flexible laparoscope (Olympus, Tokyo, Japan) was used. Four additional ports (one 12-mm, two 10-mm, and one 5-mm ports) were placed at the sites, as shown in Figure 1. The operator initially stood on the left side of the patient for the cholecystectomy, and then he was positioned between the patient's legs. After placement of trocars, a cholecystectomy was performed in the usual manner. Thereafter, the falciform ligament was dissected away from the anterior abdominal wall without complete division of the round ligament, and the dissection of the ligament proceeded toward the cephalic direction, using a Harmonic® scalpel (Ethicon, Blue Ash, OH) until the middle vein was visualized. Without mobilization of the liver, the right anterior Glissonean pedicle was dissected from the hepatic parenchyma at the hilum. After isolation of the right anterior Glissonean pedicle, the right anterior Glisson was lifted up using nylon tape and temporarily clamped to check the boundary of the right anterior section (Fig. 2). After the ischemic demarcation line was marked, transection of the hepatic parenchyma of the medial side along the Cantlie line was started. The superficial hepatic parenchyma was transected using a Harmonic scalpel, and the deeper portion of the parenchyma was dissected by using a laparoscopic cavitron ultrasonic surgical aspirator (CUSA; Valleylab, Boulder, CO). Pringle's maneuver was not used during the parenchymal transection. Dissection was meticulously performed toward the cephalic direction along the right side of the middle hepatic vein until the insertion of the middle hepatic vein into the inferior vena cava, and toward the caudal direction until exposure of the hilar plate. In this manner, medial side dissection was completed.
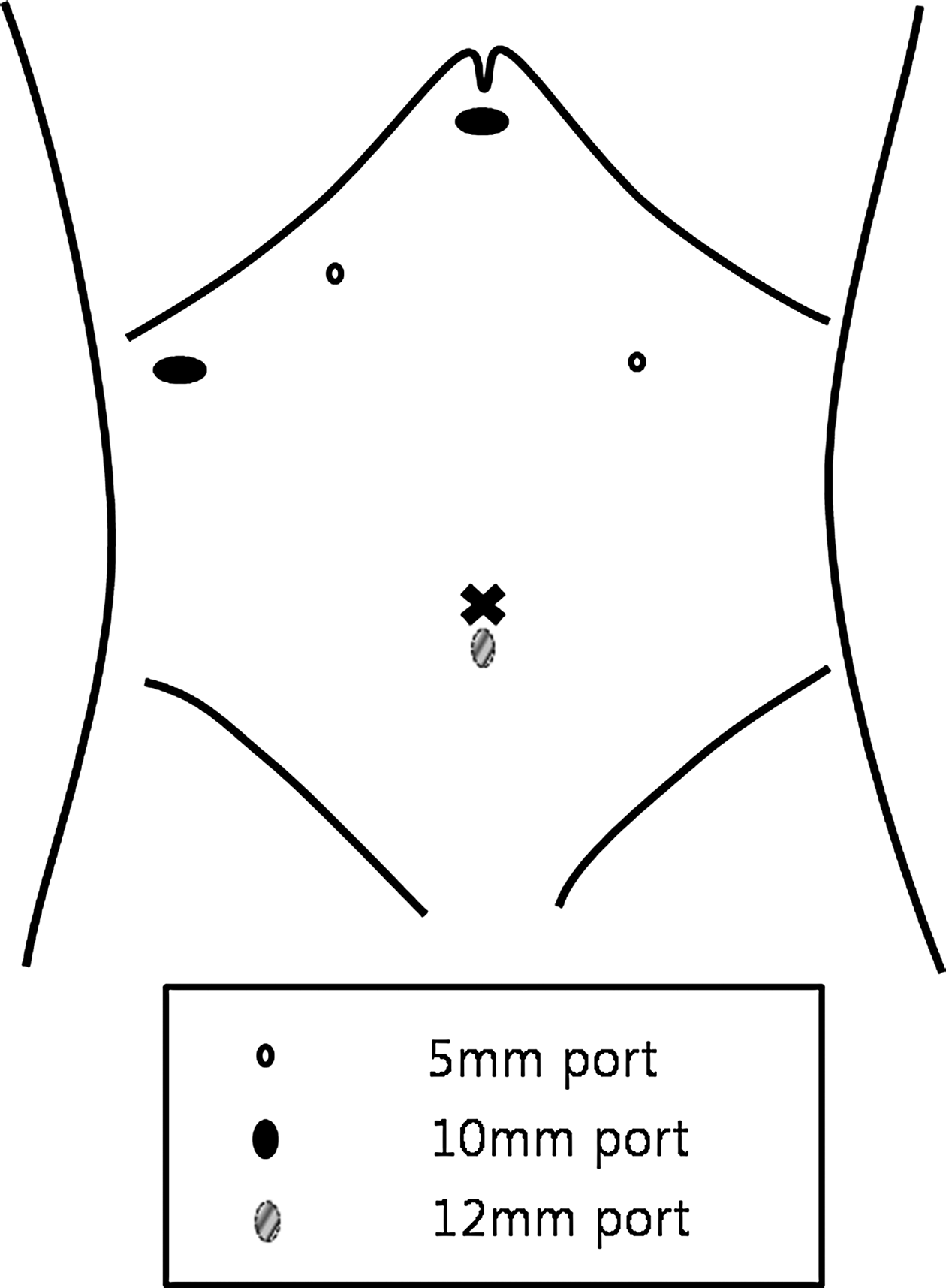
The position of the trocars.

Laparoscopic view of the dissection of the right anterior Glissonean pedicle.
Transection on the lateral side was performed along the demarcation line between the right anterior and posterior sections. The superficial hepatic parenchyma was transected using a Harmonic scalpel, and the deeper parenchyma was transected with the laparoscopic CUSA. The small branches of the hepatic veins were controlled with endoclips, and the large branches of the right hepatic vein were transected with an Endo GIA™ stapler (Tyco Healthcare, Norwalk, CT). The main right hepatic vein was preserved. Prior to complete division of the resected specimen, the right anterior Glissonean pedicle was transected using an Endo GIA stapler.
Once the resected specimen was completely divided, it was inserted into a plastic bag (LapBag; Sejong, Seoul, Korea) and extracted through a 5-cm incision that was created by extending the wound at the umbilical port or via a separate Pfannenstiel incision. After careful hemostasis, fibrin glue was sprayed onto the raw surface (Fig. 3). After irrigation, a drain was inserted, and the wound was closed in layers.

Laparoscopic view after completion of a right anterior sectionectomy. RHV, right hepatic vein; MHV, middle hepatic vein.
Results
The operative time was 680, 600, and 540 minutes for Cases 1, 2, and 3, respectively. The estimated intraoperative blood loss was about 120, 400, and 500 mL for Cases 1, 2, and 3, respectively, and there was no need for intraoperative transfusion. Two patients were discharged on postoperative Day 8 without any postoperative complications, but 1 patient with Caroli's disease was discharged on postoperative Day 30 because of fluid collection along the raw surface of the liver. This patient was managed conservatively with percutaneous drainage, and he was completely recovered at the time of discharge. The postoperative pathology of all the cases confirmed Caroli's disease and HCC with a tumor-free margin.
Discussion
Although the number of reports on laparoscopic liver resection has increased, the location of lesions still remains a major obstacle to applying laparoscopic liver resection. 8 It is still difficult to perform laparoscopic liver resection for lesions in the posterosuperior part of the liver because of poor visualization of the operative field and difficulty in controlling bleeding during parenchymal transaction. 9 However, because of recent improvement of laparoscopic techniques and the development of new equipment, reports of successful anatomic right hemihepatectomy, isolated caudate lobe resection, and right posterior sectionectomy have been published.2,10–12 The limitations of the location for laparoscopic liver resection are mainly based on the problem of poor visualization, and these limitations are being overcome by using a 30° or flexible laparoscope. 10 These laparoscopes allow us to get a superior view of the resection plane. Furthermore, a CUSA was applied in laparoscopic surgery, and this allowed us to dissect hepatic parenchyma meticulously and to prevent massive bleeding from major vessels.8,10 These brought major changes to the indication for laparoscopic liver resection in that this procedure can be applied not only for peripherally located lesions (Couinaud segments 2–6), but also for lesions located in posterosuperior segments (Couinaud segments 1, 7, and 8).
From an oncologic point of view, anatomic liver resection has been advocated as the preferred treatment in HCC because it allows for complete removal of the tumor-related domain, including possible venous tumor thrombi around the main tumor.5,13–15 Because patients with HCC usually have concomitant hepatic dysfunction or liver cirrhosis, minimizing the volume of resection and leaving as much liver volume as possible are usually recomended.16–18 Therefore, anatomic right anterior sectionectomy would be a more appropriate surgical option than right hepatectomy if the tumor is limited to the right anterior section. When compared with right hemihepatectomy, right anterior sectionectomy has an advantage in that the remaining volume of the right posterior section can be preserved. This strategy may also apply to laparoscopic liver resection, but until now there has been no report about laparoscopic anatomic right anterior liver resection in the English literature.
The major concerns in laparoscopic right anterior liver resection are how to precisely maintain two transection lines properly with a safe resection margin and how to preserve securely the vascular structures that drain or supply the remnant liver. This procedure is technically demanding as the surgeon will frequently encounter numerous branches from the in- and outflowing blood vessels of the remnant liver. 8 Careful dissection and control of all the vessels are critical for a safe resection, especially in the hilum and deep portion around the hepatic veins and inferior vena cava.
There are several ways to perform anatomic liver resection. As mentioned in our previous reports, the laparoscopic Glissonean approach can be a safe method for segment-oriented hepatectomy, and this facilitates performing a tailored liver resection by removal of only the involved liver segments.2,16,19 Furthermore, accumulated experience in laparoscopic liver resection, more precisely determined pre- and intraoperative plans, and developed techniques and instruments, including laparoscopic ultrasonography, have facilitated safe and feasible parenchymal transection and vascular control. Laparoscopic ultrasonography is quite useful for providing information about the tumor's location and its relationship with the vascular structures and for helping achieve an adequate margin.2,8,16,20
In summary, these cases confirm that totally Lap-RAS is a feasible operative procedure in patients with lesions in the right anterior section of the liver. However, the long operative time should be lessened so that this procedure becomes a reproducible operative technique with greater safety through further accumulation of experience and technical refinements.
Footnotes
Disclosure Statement
No competing financial interests exist.