
Abstract
Abstract
Objective:
In transoral robotic surgery (TORS), if an endoscopic arm equipped with two integrated cameras is placed close to a lesion, a three-dimensionally magnified view of the operative field can be obtained. More important is that the operation can be performed precisely and bimanually using two instrument arms that can move freely within a limited working space. We performed TORS to treat several diseases that occur in the parapharyngeal space (PPS) and subsequently analyzed the treatment outcomes to confirm the validity of this procedure.
Patients and Methods:
Between February 2009 and February 2012, 11 patients who required surgical treatment for the removal of a parapharyngeal lesion were enrolled in this prospective study. Nine patients received TORS for parapharyngeal tumor resection, and 2 patients with stylohyoid syndrome underwent TORS for resection of an elongated styloid process. The average age of the patients included in this study was 42 years. Five patients were male, and 6 patients were female.
Results:
TORS was successfully performed in all 11 patients. The average robotic system docking and operation times were 9.9 minutes (range, 5–24 minutes) and 54.2 minutes (range, 26–150 minutes), respectively. Patients were able to swallow normally the day after the operation. The average blood loss during the robotic operation was minimal (11.8 mL). The average hospital stay was 2.6 days. There were no significant complications in the perioperative or postoperative period. All patients were extremely satisfied with their cosmetic outcomes.
Conclusions:
PPS surgery via a transoral approach using a robotic surgical system is technically feasible and secures a better cosmetic outcome than the transcervical, transparotid, or transmandibular approach. This new surgical method is safe and effective for benign diseases of the PPS.
Introduction
Various surgical approaches have been attempted to access the PPS because of its anatomic complexity as described above. The precise surgical approach used is selected depending on the size and location of lesion, the relationship of the PPS to the great vessels, etc. However, it should be adapted to minimize the morbidity related to surgery. Although the transcervical, transparotid, and transmandibular approaches are commonly used to access the PPS, these approaches leave a visible scar on the face or neck, and all have the disadvantage of a high rate of morbidity.1–3 On the other hand, although a transoral approach does not leave a visible scar on the face, it is not widely used to remove PPS lesions because of the risks of significant bleeding, nerve injury, and insufficient resection of the lesion.
In recent years, transoral robotic surgery (TORS) using the da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) has been actively researched as a minimally invasive surgery in the field of head and neck surgery.4–9 In TORS, if an endoscopic arm equipped with two integrated cameras is placed close to the lesion, a three-dimensionally magnified view of the operative field can be obtained. Also, the operation can be performed precisely and bimanually using two instrument arms that can move freely within a limited working space. We performed TORS to treat several diseases that occur in the PPS and analyzed treatment outcomes to confirm the validity of this procedure.
Patients and Methods
Patients
Between February 2009 and February 2012, 11 patients who required surgical treatment for the resection of parapharyngeal lesions were enrolled in this prospective study. Nine patients underwent TORS for the resection of a parapharyngeal tumor, and 2 patients with stylohyoid syndrome received TORS for the transoral resection of an elongated styloid process (Fig. 1). The Institutional Review Board of Yonsei University (Seoul, Korea) approved this research. The average age of the patients was 42 years. Five patients were male, and 6 were female. Other relevant clinical patient information is summarized in Table 1.
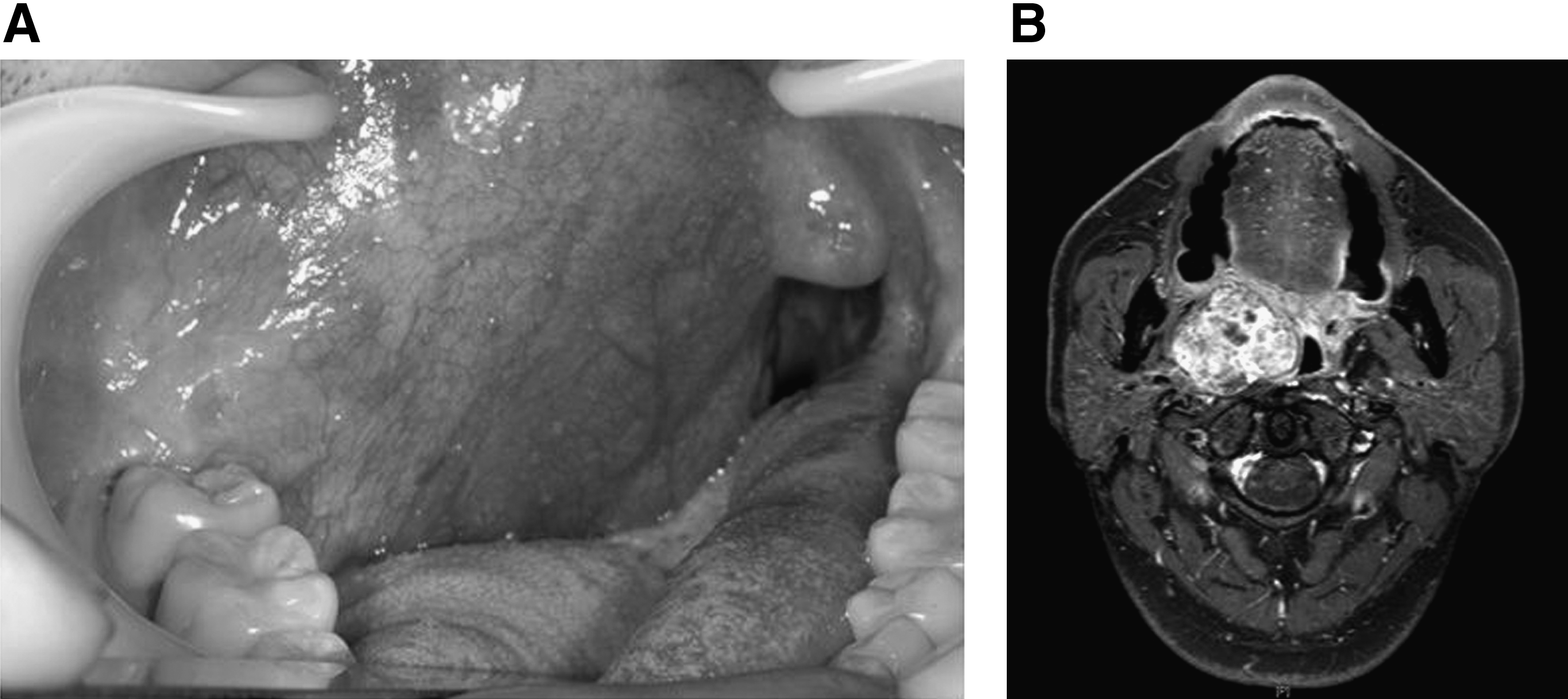
Preoperative photographs and computed tomography scan of Patient 3 with a parapharyngeal tumor.
I, extremely satisfied.
EBL, estimated blood loss; F, female; M, male.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) at least 18 years old at the time of diagnosis and (2) patients in whom surgical treatment was required for the removal of a benign lesion in the PPS. Exclusion criteria were as follows: (1) contraindication to general anesthesia or surgery and (2) cases in which either the transmandibular or transcervical approach was required for the removal of PPS lesions.
da Vinci robot system settings
After induction of general anesthesia, nasotracheal intubation was performed to secure the airway. The surgical bed was rotated 180°, and the head was positioned at the foot side of the surgical bed. Then, a shoulder roll was inserted beneath the shoulders to extend the neck and head. After the mouth was opened using a Crowe–Davis retractor, the endoscopic arm was inserted through the oral cavity, and the robotic instrument arms were positioned on either side of the endoscopic arm. The robot arm on the side of the lesion was equipped with spatula cautery, and the arm on the contralateral side was equipped with Maryland forceps. The assistant and nurse were located near the patient's head during the operation and suctioned secretions and blood and ligated blood vessels using a hemoclip.
Surgical procedure
TORS alone was performed in 9 patients to remove benign parapharyngeal tumors. The oral cavity was exposed using a Crowe–Davis retractor (Fig. 2). A vertical incision was made on the oropharyngeal mucosa overlying the tumor after the tumor boundary was confirmed by digital palpation. Careful dissection was performed around the tumor to reduce the risk of damage to the cranial nerves and major vessels. The resection was done with monopolar cautery after important structures under the surgical plane were identified by dissecting the surrounding tissues with the Maryland dissector. The axes of the articulated robotic arms were positioned to form an obtuse angle with the carotid artery to avoid damaging it. A needle driver loaded with polyglactin 910 (Vicryl®, Ethicon, Blue Ash, OH) was used to suture the incision site after the tumor was extirpated.
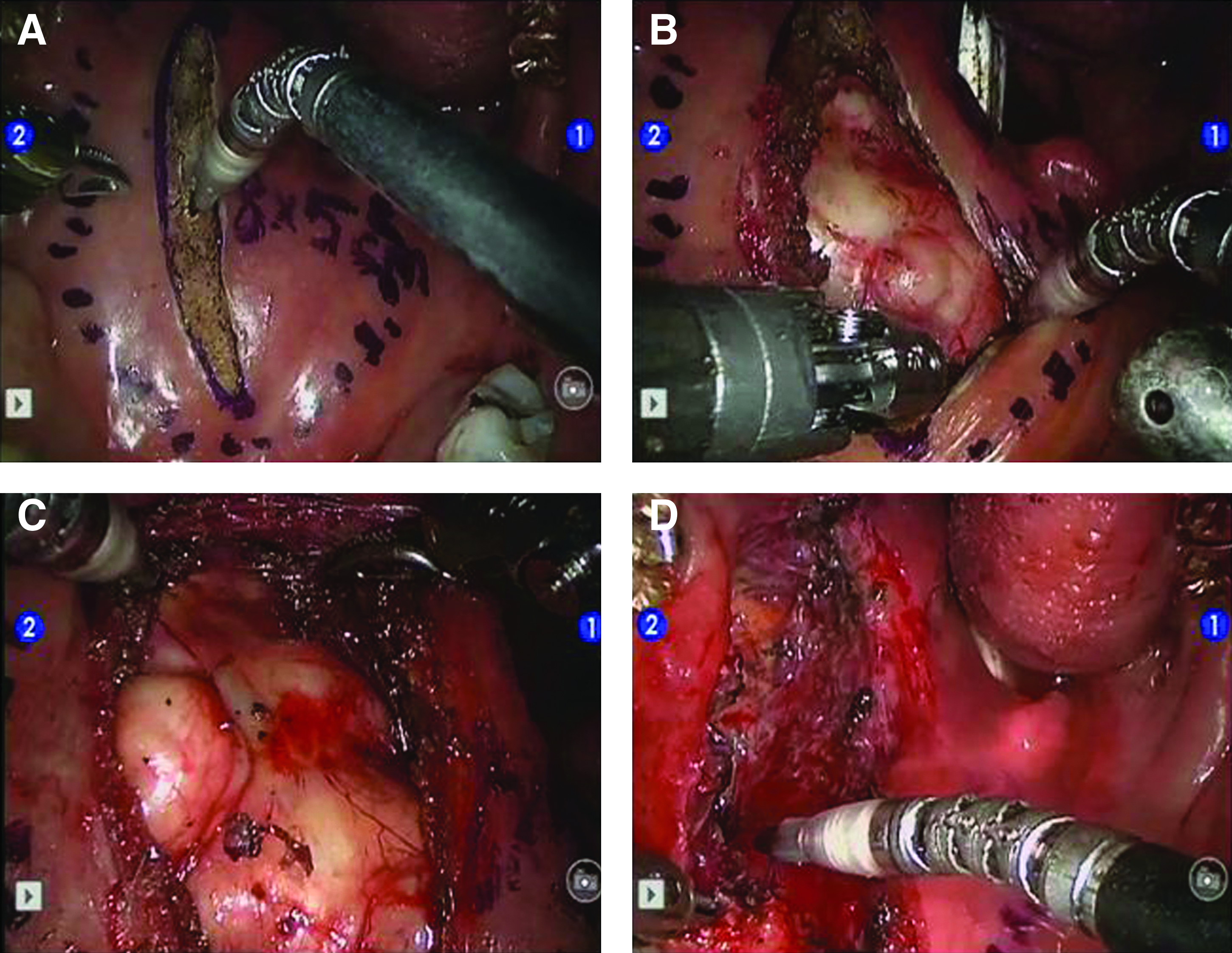
Transoral robotic surgery for the resection of parapharyngeal tumors.
Transoral robotic resection of an elongated styloid process was performed as follows (Fig. 3). After palpation of the lesion through the oral cavity, the location was marked on the oral mucosa. Then, the robotic surgical system was set in the oral cavity. First, a vertical incision was done on the oral mucosa and superior constrictor muscle. Dissection carefully proceeded through the parapharyngeal fat pad and muscle fibers along the direction that was previously marked on the mucosa. After the styloid process was identified, the distal portion was exposed as much as possible using the robotic instrument arms. After that, an assistant who was located near the patient's head cut the exposed styloid process using Rongeur forceps. Finally, the incised oral mucosa was sutured with Vicryl 3-0 using the robotic arms.
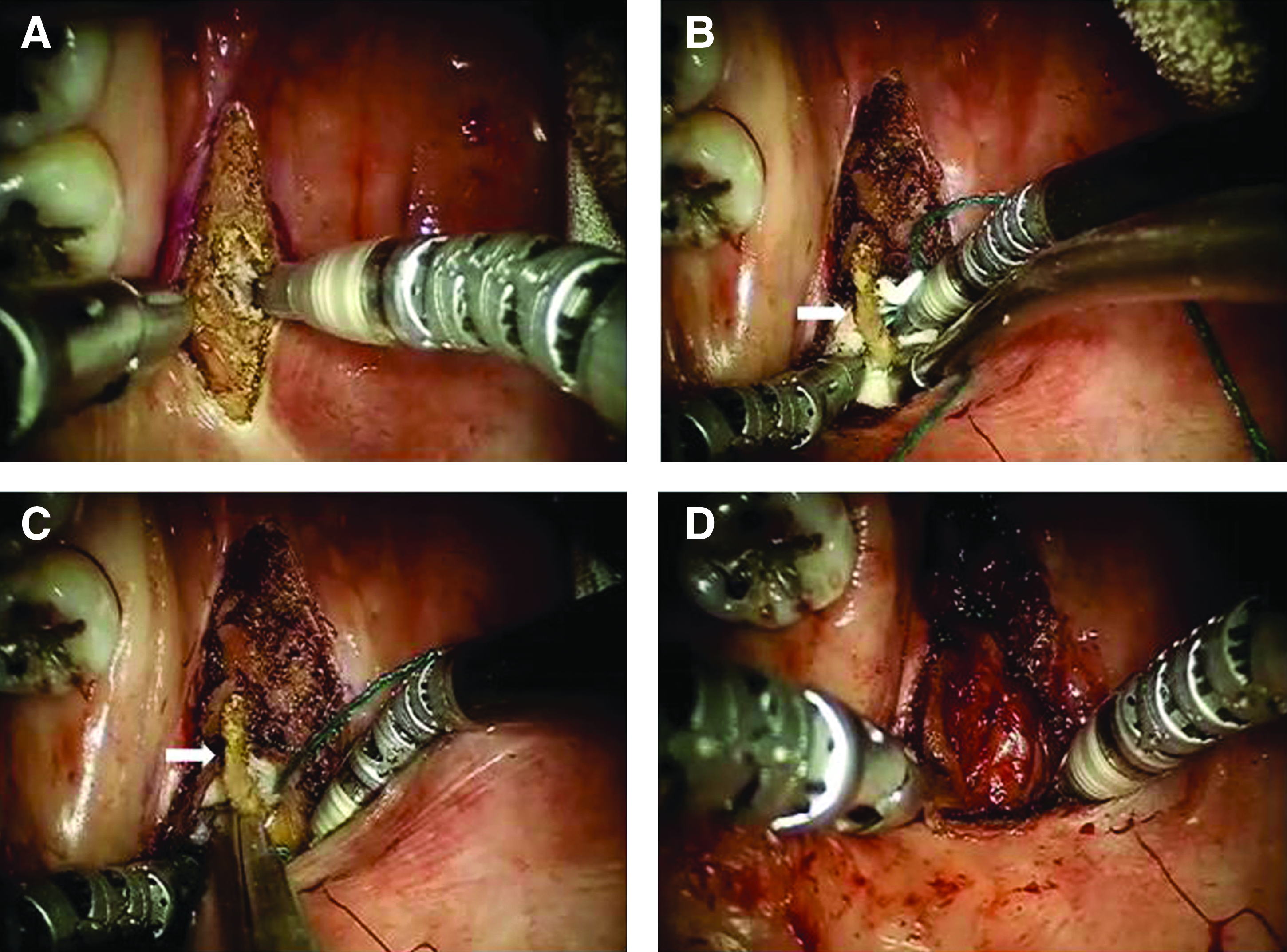
Transoral robotic resection of an elongated styloid process.
Results
Ability to perform TORS in the PPS
TORS was successfully performed in all 11 patients who were enrolled the study. Parapharyngeal tumors were successfully removed using TORS in 9 patients, and an elongated styloid process was resected transorally using TORS without significant complications in 2 patients.
Treatment and functional outcomes
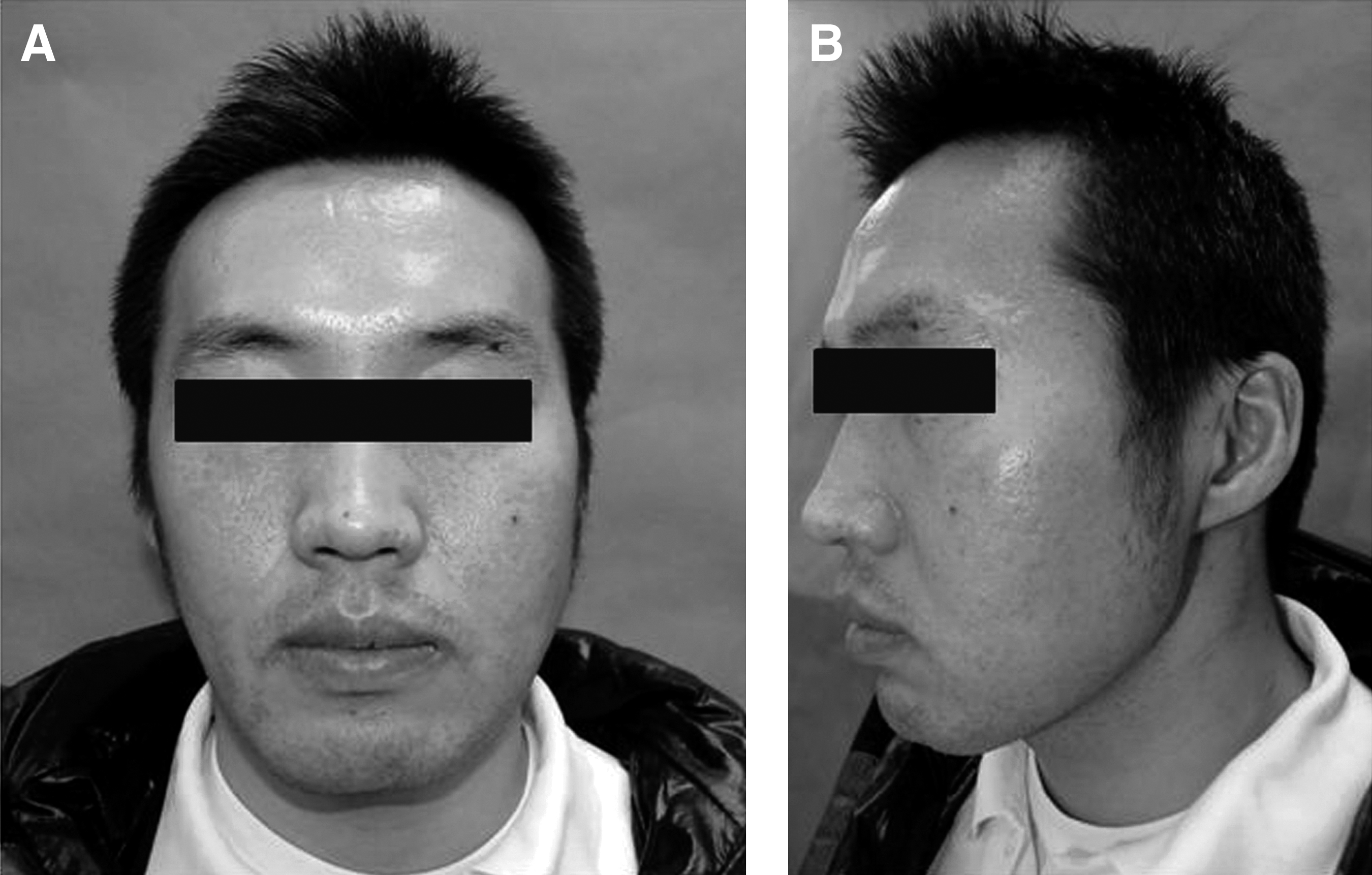
The average robotic system docking and robotic operation times were 9.9 minutes (range, 5–24 minutes) and 54.2 minutes (range, 26–150 minutes), respectively. No one required a nasogastric feeding tube after the operation, and the patients were able to swallow normally on postoperative Day 1. There were no cases of orocervical fistula after TORS. The average hospital stay was 2.6 days. Parapharyngeal tumors were removed without tumor spillage, preserving the capsule of the tumor in 9 patients. The 2 patients who received TORS to resect an elongated styloid process had resolution of their symptoms after the operation. Patient satisfaction with the cosmetic results was measured on a graded scale of I (extremely satisfied), II (satisfied), III (average), IV (dissatisfied), and V (extremely dissatisfied). All patients were extremely satisfied with their cosmetic outcomes (Fig. 4 and Table 1).
Complications
In this study, there were no cases of cranial nerve paralysis or cases that required transfusion due to significant bleeding and were converted to open surgery. The average blood loss during the robotic operation was minimal (11.8 mL).
Follow-up
During the follow-up period of 17.7 months (range, 8–42 months) on average, there was no recurrence of tumor or symptoms after the operation in this study.
Discussion
The approach to surgery in the PPS is challenging because of the complexity of the area and the vicinity of vital neurovascular structures. Work and Hybels 10 advocated the external surgical approach as the treatment of choice in managing benign parapharyngeal tumors and described the intraoral approach as a “blind” surgical approach that can damage the vessels or nerves. Varghese et al. 11 reported a case of pleomorphic adenoma that developed in the minor salivary gland of the PPS that was excised via the mandibular swing approach with no surgical complications. However, these kinds of invasive approaches left a visible scar on the face or neck and had a high morbidity rate.
O'Malley et al. 4 reported the feasibility of TORS using the da Vinci Surgical System for the resection of parapharyngeal tumors. With the advantages of conventional transoral surgery, it is easier to manage the neurovascular structures of PPS through the precise technology and superior visualization of the robot. In our study, the authors successfully removed benign lesions of the PPS without significant bleeding and postoperative cranial nerve palsies. Thanks to a three-dimensionally magnified view of the operative field supported by the robot's endoscopic arm, even tiny vessels that could not be seen with the naked eye could be managed with a hemoclip or electrocautery.
Stylohyoid syndrome consists of characteristic cervicopharyngeal pain caused by elongation or ossification of the styloid process–stylohyoid ligament complex without a history of trauma or surgery. 12 Patients who do not respond to medical treatment should undergo surgical treatment to resolve their symptoms. If an external approach such as the transcervical approach was used to resect the styloid process, it was easier than the transoral approach because of better visualization and maneuverability of neurovascular structures.13,14 However, these external approaches leave a visible scar on the face or neck, and there is morbidity related to the procedure. Therefore, the transoral approach is preferable to the external approach. Although the transoral resection has better cosmetic results than the transcervical approach, it also has several disadvantages. Because of the restricted working space, it is difficult to resect the lesion precisely and completely. There are also risks of injury to the great vessels and cranial nerves because of the proximity to these neurovascular structures. In our study, we used a robotic surgical system to resect the styloid process transorally. During the operation, estimated bleeding loss was minimal (5 mL), and the operation time was short (22.5 minutes). The patients were able to tolerate an oral diet at postoperative Day 1 and on average discharged 2.5 days postoperatively.
There are risks of significant bleeding and neural injury during transoral surgery because of the proximity to the great vessels and cranial nerves. However, in TORS, an endoscopic arm equipped with two integrated cameras can be positioned close to the operative field through the oral cavity and gives the surgeon a three-dimensionally magnified view of the operative field. This robot's superior visualization helps the surgeon identify even tiny vessels that are difficult to identify with the naked eye, and then these can be ligated using a hemoclip or electrocautery. Also, a precise operation can be performed within a limited working space using robotic instrument arms, which can move 360° freely. Accordingly, the surgical plane could be kept as close to the lesion as possible during the operation. If resection was done with monopolar cautery after identification of important structures under the surgical plane by lifting and spreading the surrounding tissues with a Maryland dissector, significant neurovascular structures could be easily preserved without iatrogenic injury.
The major advantages of PPS surgery via the TORS approach are no external incision and minimal damage to the vital structures such as the carotid vessels or cranial nerves by an exact understanding of the surrounding structures through a magnified three-dimensional view. With the TORS approach, elaborate dissection is possible because of the 360° freely movable distal end of the robotic arm directed by the surgeon. These magnified three-dimensional views and elaborate movement of robotic arms are important factors that have overcome the disadvantage of a “blind” transoral approach. The estimated blood loss was minimal, and the operation time was largely reduced compared with conventional open approaches. Also, the patients who underwent TORS showed a rapid recovery of swallowing function in the postoperative period and were discharged on average 2.6 days postoperatively.
Conclusions
PPS surgery via a transoral approach using a robotic surgical system is technically feasible to remove PPS lesions without an external scar. Even if there should be a longer follow-up period for these patients and a copious accumulation of similar cases, this research suggests that the TORS approach is a safe and feasible modality for the excision of benign lesions of the PPS.
Disclosure Statement
No competing financial interests exist.