
Abstract
Abstract
This case report describes a 63-year-old man initially diagnosed as having a 2.5-cm gastric adenomatous polyp with low-grade dysplasia. In contrast to using conventional knives for endoscopic submucosal dissection, the standard diathermic snare tip was used as an alternative knife for endoscopic submucosal dissection of the lesion with successful en bloc resection. The procedure was performed without complications. The polyp was finally confirmed as a tubulovillous adenoma with focal high-grade dysplasia.
Introduction
Case Report
A 63-year-old man underwent gastroscopy because of symptoms of acid distress and the identification of a large flat polyp on the lesser curvature side of the lower gastric body, across the angle of the stomach (Fig. 1). The polyp was initially estimated as being approximately 2.5 cm. Biopsy confirmed the presence of an adenomatous polyp with low-grade dysplasia. The man's medical history included diabetes mellitus, hypertension, and uremia, for which he had been undergoing regular hemodialysis for more than 5 years. The components of his coagulation profile, including prothrombin time, activated partial thromboplastin time, and platelet count, were all within acceptable ranges. Following discussion with the patient and his family, it was decided the patient should undergo ESD of the large gastric polyp.
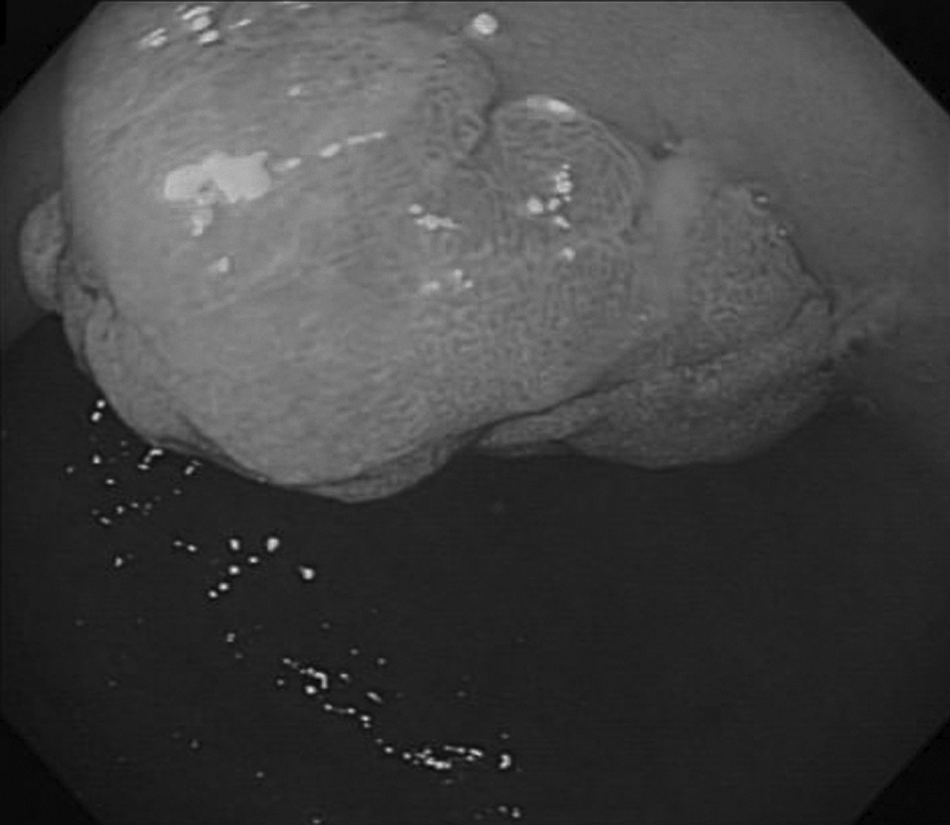
A large flat polyp was identified in the stomach.
The tip of a standard snare (model SD-9U-1; Olympus) (Fig. 2) with an electrosurgical generator (PulseCut slow mode 15 W, ForcedCoag 2 mode 20 W; model ESG-100; Olympus) was used for resection. A transparent attachment (model D-201-12402; Olympus) was fitted on the scope to secure the visual field, and a carbon dioxide insufflation system was used. The procedure occurred in stages that included the mixing of a solution of indigo carmine, epinephrine, and glycerin for submucosal layer injection, circumferential incision (Fig. 3), and submucosal dissection. Hemostatic forceps (model FD-410LR, Coagrasper; Olympus) were used in soft coagulation mode with a 80-W output. Clips were applied to bleeding points and blood vessels during and after dissection (Fig. 4). The polyp was en bloc resected and gently dragged out without complications or sequelae (Fig. 5). The polyp was finally confirmed as a tubulovillous adenoma with focal high-grade dysplasia (Fig. 6).

The diathermic snare (right) was retracted into the sheath to expose the tip, leaving an approximately 1-mm length (left) for endoscopic submucosal dissection.
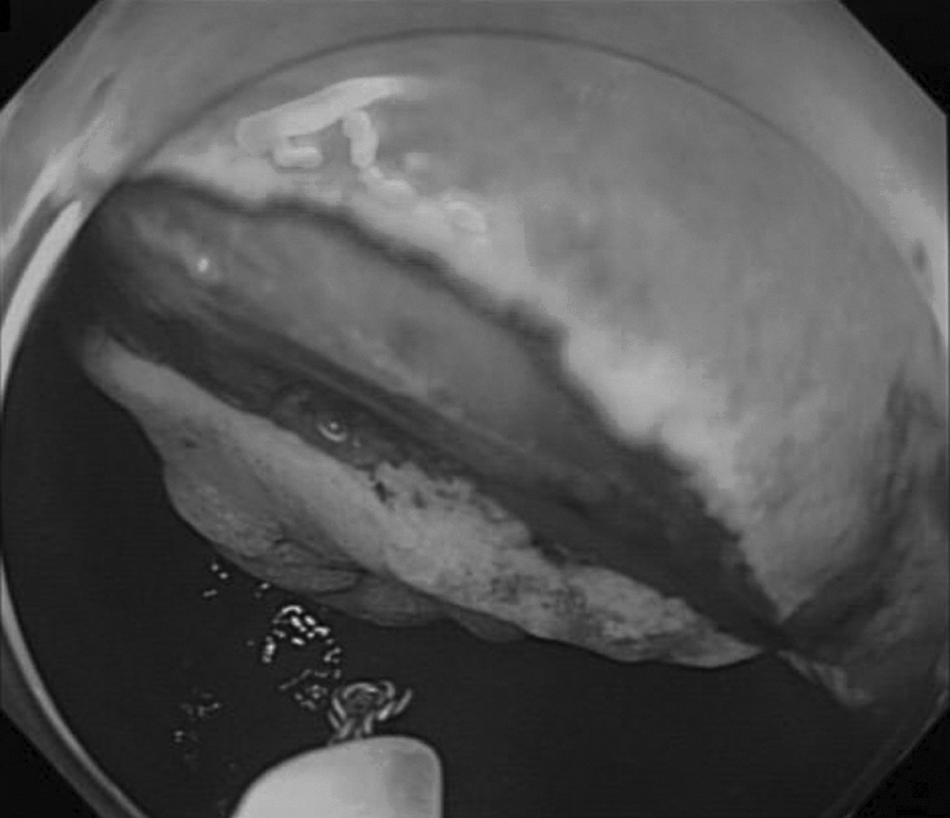
The snare tip was used for circumferential incision of the gastric polyp.
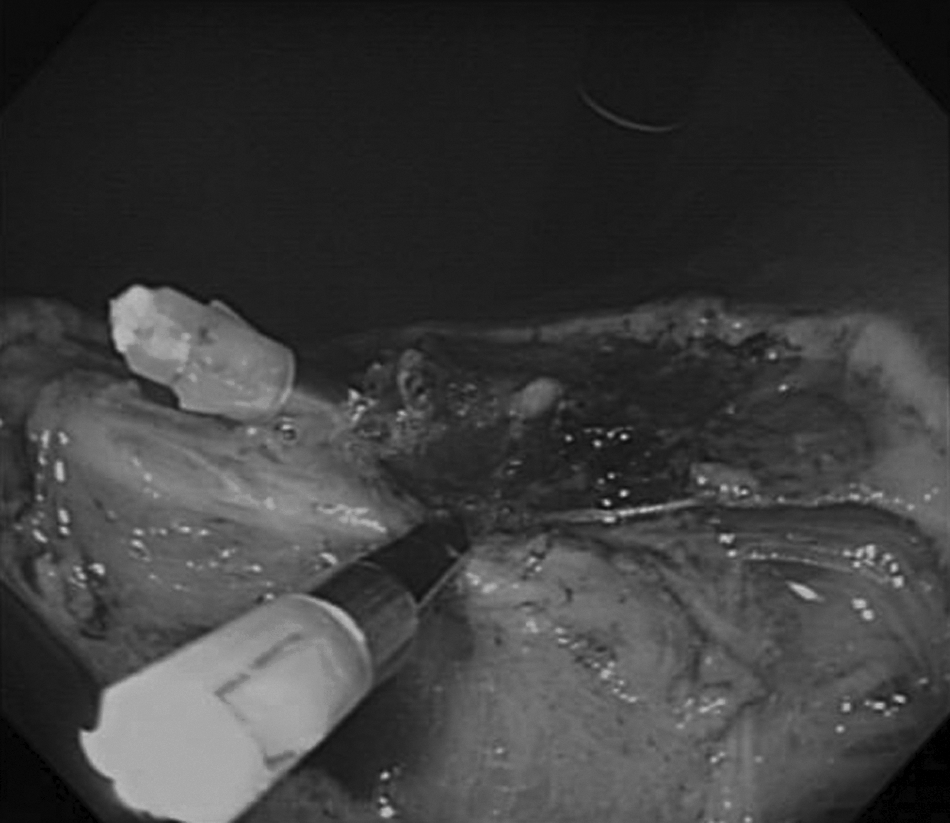
Thermal coagulation and clips were used to manage the bleeding points of the post–endoscopic submucosal dissection wound.
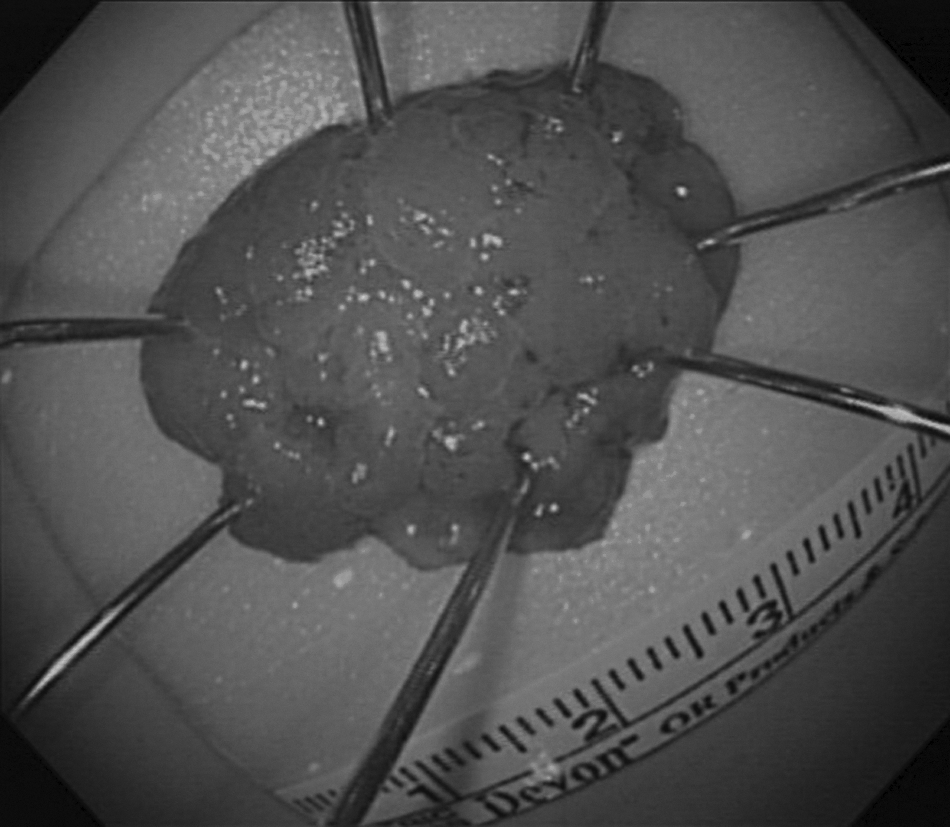
The gastric polyp was measured as 2.4×2.6 cm in size.
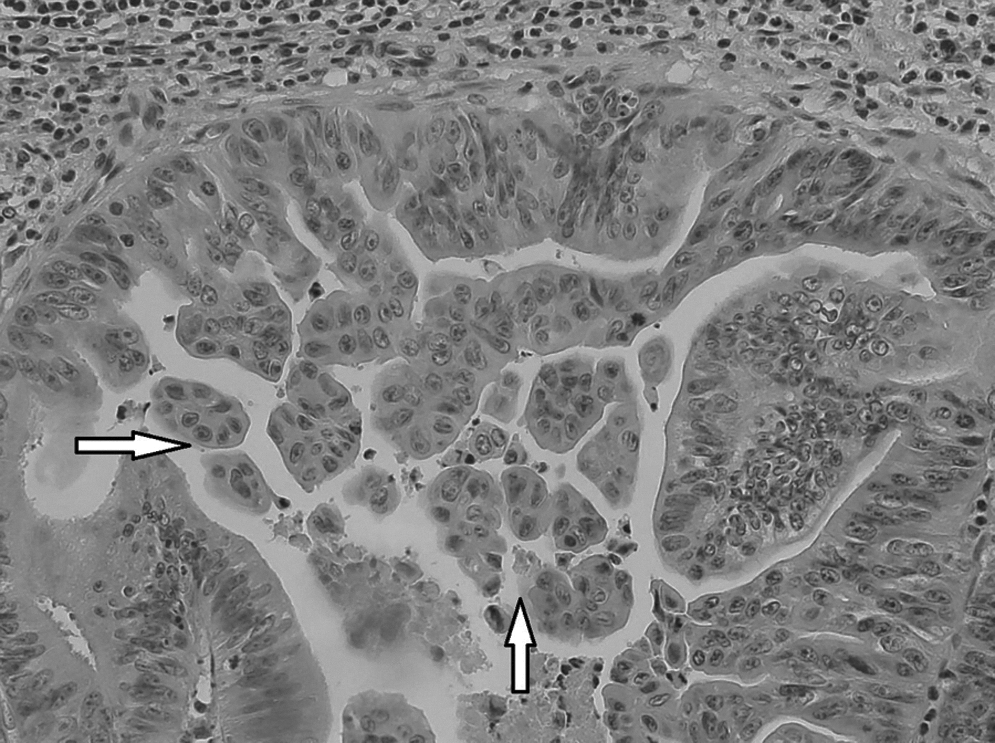
The gastric polyp was tubulovillous adenoma with focal high-grade dysplasia (arrow). Hematoxylin and eosin stain, magnification×400.
Discussion
Gastric dysplasia can arise as a flat or depressed process or present as a raised circumscribed lesion protruding above the mucosal surface, occasionally referred to as an adenoma. 3 Most gastric adenomas are sessile and display tubular, tubulovillous, or villous architecture. 3 Risk factors for malignant transformation of gastric adenomas including histologic type (tubulovillous), high-grade dysplasia, redness, ulceration, depressed type, and size no smaller than 2.0 cm.4–6 High-grade dysplasia is the most important risk factor for malignant change. Gastric adenomas are all considered precursors of gastric cancer; therefore, complete removal of the adenoma is recommended, even in low-grade dysplasia.7,8
Intraluminal endoscopic resection, including EMR and ESD, represents an alternative strategy to surgery for management of gastric dysplasia. Previous studies have established that ESD is superior to EMR for en bloc removal, increases histologically complete resection rates of gastrointestinal mucosal tumor, and reduces recurrence rates,1,2,9 especially when the tumor size is larger than 2 cm.1,10
In EMR techniques, a diathermic snare is a pivot instrument used for resection of the lesion. No previous study has described its use in ESD. Several commercially available knives have been developed for ESD, include needle, hook, flex, and isolated-tip knives. 11 In the authors' experience, the snare tip maneuver for ESD displays similarities to operating the flex knife: both instruments have adjustable loop-like tip lengths. Compared with needle-shaped knives, loop-tip knives are able to contact larger areas of the lesion and can therefore offer more extensive incision and dissection ability. In addition, the cost of a diathermic snare is lower than that of other commercially available knives. However, care must be taken when adjusting the length of the snare tip to prevent unintended perforation. For safety and to facilitate operations in a limited space during ESD, the outer sheath of the snare should not be extended too far from the working channel of the scope, so that an approximate 1-mm length of the snare tip is exposed, by retracting the other part of the snare into the sheath. In addition, we recommend that the use of such a technique should be done by surgeons experienced in ESD and in the case of gastric lesions because of the thickness of the gastric wall it is safer to avoid the complication of perforation.
Conclusions
The diathermic snare is a commonly used instrument in an endoscopy examination unit. In addition to its use as the standard diathermic snare in EMR, the snare tip can be used as a knife in ESD with a lower cost. Although this report suggested that the snare tip can provide a safe and efficient instrument for ESD, further investigations are still needed for confirmation.
Footnotes
Disclosure Statement
The authors have no conflict of interest to disclose. C.-W.Y. performed the endoscopic therapy and writing and drafting of the manuscript and gave final approval for publication. H.-H.Y., Y.-Y.C., M.-S.S., and C.-J.C. performed the drafting of the manuscript and gave final approval for publication.