
Abstract
Abstract
Background:
We developed a new procedure called hybrid endoscopy-assisted breast-conserving surgery (EBCS), which consists of a combination of plastic surgery and endoscopic surgery techniques. The purpose of this study was retrospectively to analyze the clinical outcome of hybrid EBCS and compare the cosmetic outcomes between hybrid EBCS and conventional breast-conserving surgery (CBCS).
Patients and Methods:
We reviewed medical records of patients who had undergone hybrid EBCS (n=73) or CBCS (n=90) between May 2005 and April 2011 and had been followed up in our department until March 2012. The clinical outcomes and cosmetic outcomes of these two groups were compared. The safety of hybrid EBCS was also analyzed by confirming its complications and pathological surgical margin.
Results:
In the hybrid EBCS group, operation time was longer by 30–50 minutes. Blood loss was not significantly different between the two groups. The surgical margin of hybrid EBCS was as follows: 1 patient (1.4%) had a positive margin, 4 patients (5.5%) had a margin of <2 mm, in 9 patients (12.3%) the margin was ≥2 mm and <5 mm, and in 59 patients (80.8%) it was ≥5 mm. Seven cases (9.6%) of postoperative complications occurred in 6 hybrid EBCS patients. To date, no local recurrence has been observed in hybrid EBCS patients (postoperative observation period, 18.1±5.6 months). Compared with the CBCS group, the hybrid EBCS group had better cosmetic results, especially with a less noticeable operative scar (P<.01).
Conclusions:
Hybrid EBCS can provide sufficient free margin, and its surgical curability is acceptable. Additionally, this method is superior to CBCS in terms of cosmetic outcome.
Introduction
Patients and Methods
Patients
In this retrospective study, we reviewed medical records of patients who had undergone hybrid EBCS or CBCS between May 2005 and April 2011 and had been followed up in our department until March 2012. We began performing hybrid EBCS in September 2009 and have used this technique instead of CBCS as the standard operation for BCS ever since. BCS was indicated for patients who met the following criteria: no evidence of invasion to skin, nipple, or areola; tumor size <3 cm in diameter; mammary gland region to be resected less than one-fifth of total area; and feasibility of administering postoperative radiation therapy. Patients with tumors requiring quadrantectomy in the lower pole region were excluded from this study because they were not indicated for hybrid EBCS owing to difficulties in achieving a desirable cosmetic result.
Presurgical diagnosis and therapy
Preoperative patient workup included physical examination, mammography, ultrasound (US), bilateral high-resolution enhanced breast magnetic resonance imaging, and enhanced computed tomography or positron emission computed tomography. All the patients underwent mammography, US, magnetic resonance imaging, and enhanced computed tomography or positron emission computed tomography. For pathological diagnosis, US-guided vacuum-assisted biopsy or US-guided core needle biopsy was performed when the tumor could be identified with US. Stereotactic vacuum-assisted biopsy for histological diagnosis was carried out for calcifications identified by mammography. Twenty-nine patients (49%) with stage II or more advanced disease underwent neoadjuvant chemotherapy or neoadjuvant endocrine therapy if informed consent was obtained (Table 1).
Data are number (%) unless indicated otherwise.
Ax, axillary dissection; BCS, breast-conserving surgery; CBCS, conventional breast-conserving surgery; CR, complete response; EBCS, endoscopy-assisted breast-conserving surgery; PD, progressive disease; PR, partial response; SD, stable disease; SNB, sentinel lymph node biopsy; STD, standard deviation.
Presurgical marking
Before surgery, US-guided planning of the resection range of the mammary gland and mobilization range of the preserved mammary gland was carried out after considering magnetic resonance imaging findings. For nonpalpable tumors with calcification that were identified by mammography, initial stereo-guided insertion of a hookwire into the calcification was performed. After this, US-guided planning was performed.
During planning, patients were laid in the operative position. The surgical margin was marked 1.5–2 cm distant from the tumor edge. Next, we marked the penetrating branch of the internal thoracic vessels in the parasternal area on the tumor side by US, so as not to damage these vessels during surgery. The internal thoracic vessels are important to maintain blood supply to the preserved mammary gland.
Sentinel lymph node biopsy and axillary lymph node dissection
Sentinel lymph node biopsy (SNB) was carried out under direct vision through a 2.5-cm skin incision made in the axillary area using both radioisotope and dye methods. In patients with micro- or macrometastasis diagnosed by rapid intraoperative pathological diagnosis, the skin incision was enlarged to 4–5 cm, and after insertion of a wound protector (Lap-Protector®; Hakko Co., Nagano, Japan), axillary lymph node dissection was performed with complete resection of the I, II, and III levels. To minimize false-negative sentinel lymph node cases by obtaining precise pathological diagnosis through examination of permanent sections, we have performed SNB with the patient under local anesthesia in our institution since July 2009. More than 50% of the hybrid EBCS patients underwent SNB with local anesthesia.
Injection of color marking
All the BCS procedures were performed with the patient under general anesthesia. During surgery, the resection range of the mammary gland and the location of the tumor were confirmed with US from the body surface. After the skin was marked with gentian violet ink, a 1:1 mixture of indigo carmine and xylocaine jelly (Astra Zeneca, Wilmington, DE) was injected along the previously marked resection margin into the mammary gland and subcutaneous adipose tissue (Fig. 1a).
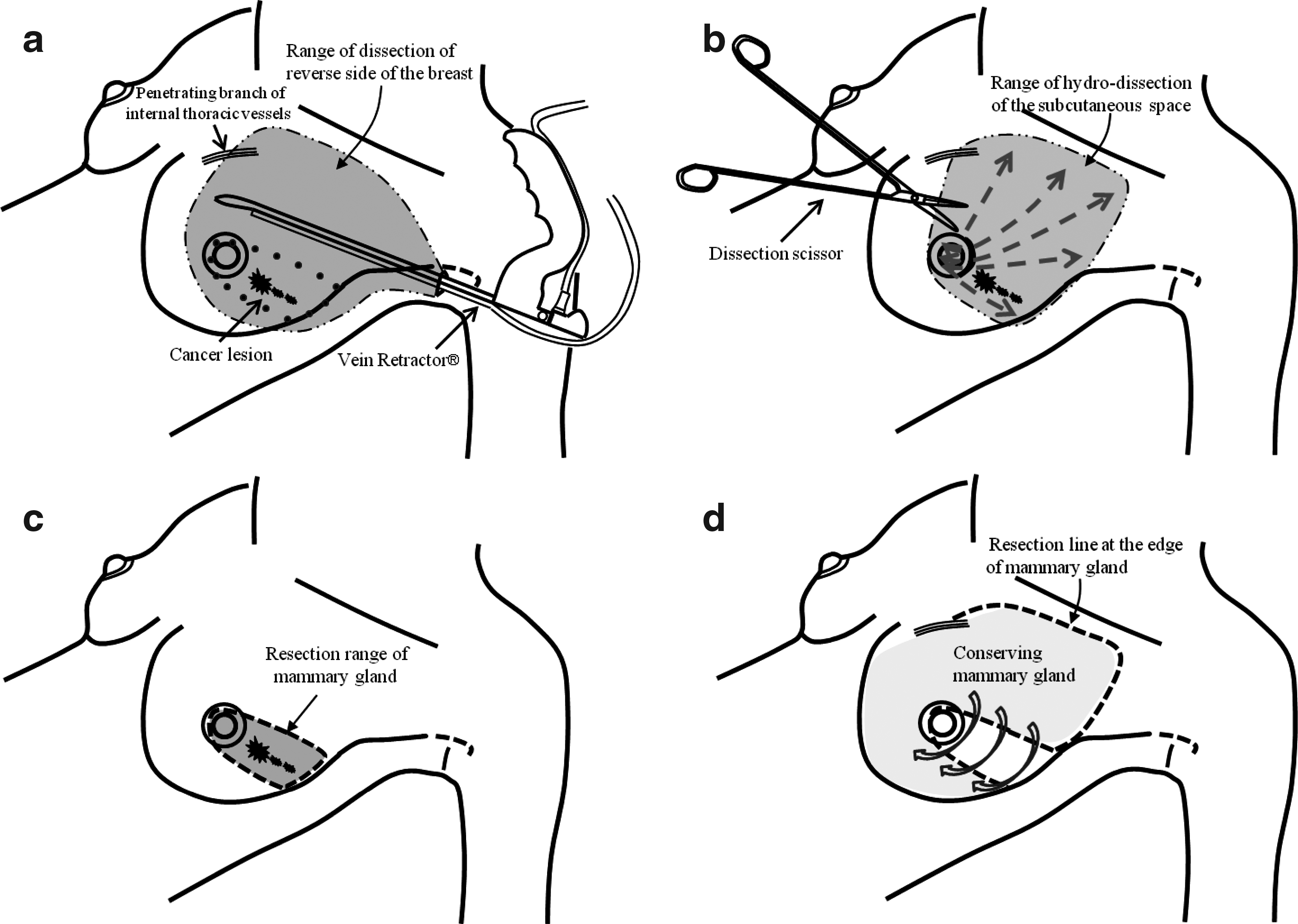
Operative procedure of hybrid endoscopy-assisted breast-conserving surgery.
Dissection of the posterior surface
Extensive endoscopic dissection of the posterior surface was performed with a vein retractor (Karl Storz Endoscopy, Tuttlingen, Germany) attached to a suction tube inserted through the incision used for SNB (Figs. 1a, 2f, and 3a and b). To avoid exposing the tumor, the fascia pectoralis in the region directly under the tumor was included in the dissection of the posterior surface. This procedure mainly consisted of blunt dissection with the vein retractor. However, if small vessels and cord-like ligaments were present, precoagulation using Power Star® (Ethicon Inc., Somerville, NJ) and some sharp dissection were performed (Figs. 1a, 2f, and 3a). This procedure includes two important points. First, the penetrating branch of the internal thoracic vessels must be preserved so that the blood supply to the remaining mammary gland can be maintained, as long as this does not affect the effectiveness of the surgery. Second, dissection must be carried out in an area larger than the tumor lesion. Especially in the lateral field, it is important to completely dissect the area on the fascia of the serratus anterior muscle and over the fascia pectoralis (Fig. 3b). Such complete dissection enables mobilization of mammary gland and adipose tissue to the lateral area.
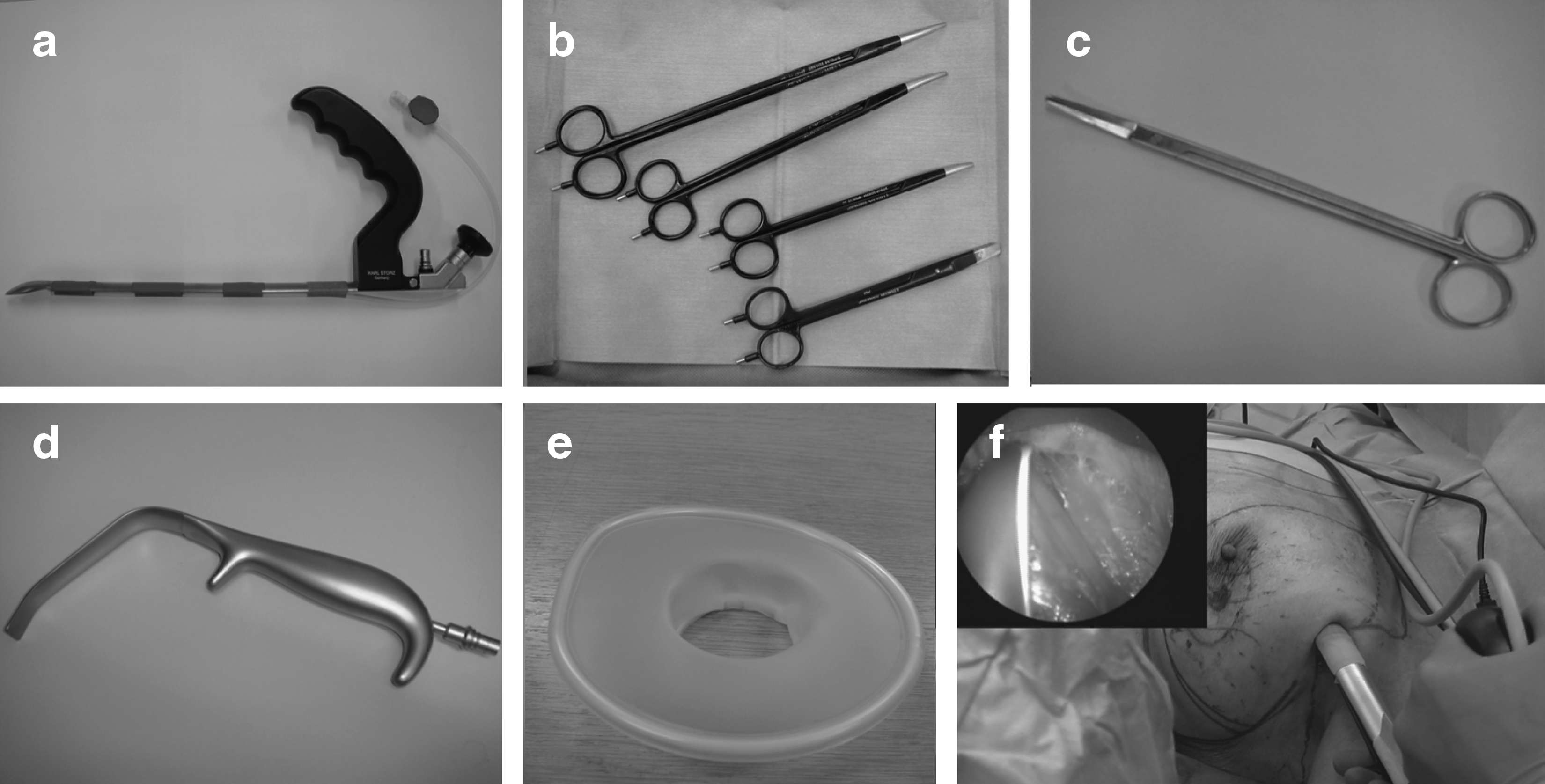
Instruments for performing hybrid endoscopy-assisted breast-conserving surgery.
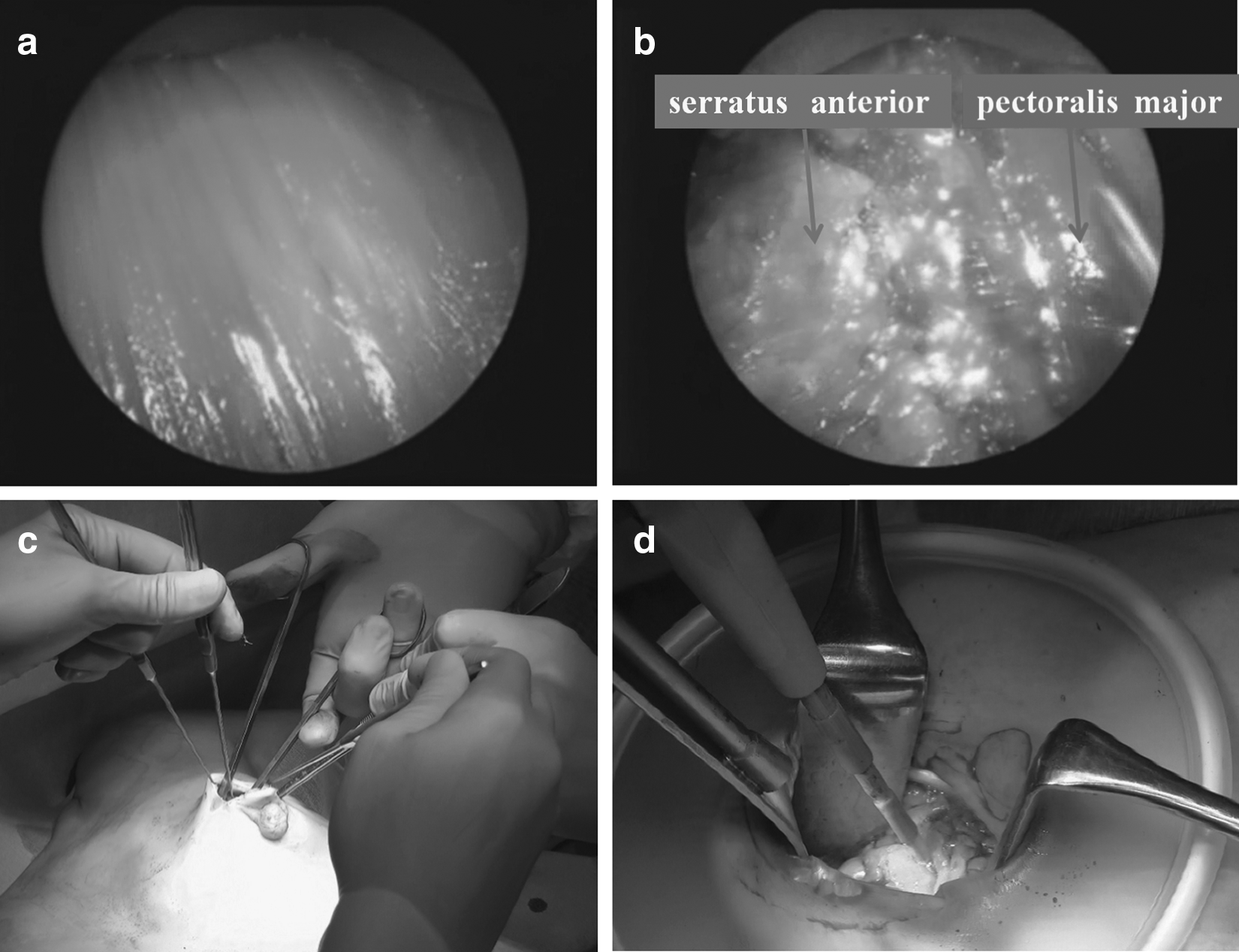
Operative findings.
Subcutaneous hydrodissection using the tumescent technique
For hydrodissection between the mammary gland and the skin of the breast, a sufficient amount (more than 150 mL) of physiological saline containing epinephrine (diluted 1:1,000,000) was injected into an extensive area of subcutaneous breast tissue, including the resection range and the mammary gland to be mobilized (Fig. 1b). It is important to inject a sufficient amount of saline to a depth at which injection can be carried out without resistance and then to dissect between the mammary gland and the skin of the breast. If the lesion is located near the skin, saline should be injected superficially.
Skin flap development
A skin flap was developed in the same area as hydrodissection using Nagumo dissecting scissors (Sawkenn Co., Ltd., Japan) (Figs. 1b, 2c, and 3c). If sufficient hydrodissection was performed, development of a skin flap could be easily achieved without major bleeding. Care was taken to preserve the adipose tissue of the skin flap as much as possible. If the skin flap is too thin, skin flap necrosis may occur.
Resection of mammary gland using light guidance
A small periareolar semicircular (up to two-fifths of a circle) incision was made. If the lesion was located on the lateral side of the breast, an incision was made in the lateral edge of the breast. After dissection with Nagumo dissecting scissors, the Lap-Protector was inserted to protect the wound and ensure adequate visualization. The mammary gland was cut along the injected marking (Figs. 1c and 3d) using a light-guided retractor (FourMedics, Tokyo, Japan) (Fig. 2d). To ascertain the surgical margin on the nipple side and on the side opposite the nipple, marking with 3-0 silk thread was made along these two margins of each resected specimen.
After a negative result was confirmed from histological examination of the four edges of the surgical margin, surgical clips were placed at each margin as landmarks for postoperative radiation therapy.
Mobilization
To repair the breast, widely dissected mobilized mammary gland and adipose tissue was moved to the affected area and sutured with absorbable thread (Fig. 1d).
Skin closure
After the surgical area was washed with physiological saline and hemostasis was confirmed, a ReliaVac® drain (C.R. Bard Inc., Murray Hill, NJ) was inserted under the skin. The incision was closed with 4-0 polydioxanone (Ethicon) and 5-0 nylon thread.
Compression of the surgical region
We placed gauze on the surgical region and compressed it evenly with a breast band. Attention was paid to avoid local strong compression on the skin flap, as this results in failure of blood supply to the skin.
Care of operative scar
The wound was sealed and covered with Micropore® (3M, St. Paul, MN) for 3 months after surgery.
Rapid intraoperative pathological diagnosis
Rapid pathological diagnosis was performed for the four edges of the resected mammary gland and the sentinel lymph nodes during surgery using hematoxylin and eosin staining.
Permanent pathological diagnosis
Tissue from partial resection of the breast was sectioned at a thickness of 5 mm. After the breast cancer lesion was mapped, the distance to the margin was confirmed. The resected sentinel lymph nodes were also re-examined with immunohistochemical staining.
All patients underwent radiotherapy (50 Gy) of the conserved breast and adjuvant therapy according to specific stage and risk factors.
Methods of cosmetic evaluation
Four breast surgeons with more than 10 years of experience in breast surgery performed cosmetic evaluation by using the cosmetic evaluation method recommended by the Japanese Breast Cancer Society (JBCS) after the breast-conserving therapy11,12 and with a 4-point scoring system (excellent, good, fair, or poor) reported by Winchester and Cox. 13 Using the JBCS method, eight elements were evaluated: breast size, breast shape, breast scarring, breast hardness, nipple/areolar size and shape, nipple/areolar color, nipple position, and lowest point of the breast. These elements were scored as shown in Table 2.
Each case of a apositive margin and bclose margins in permanent margin status was a ductal carcinoma in situ lesion.
Data on patient characteristics, clinical outcomes, cosmetic assessment of the two groups, and the surgical margin and complications of the hybrid EBCS group were compiled and analyzed for all patients.
Statistical analysis
Data were analyzed using SPSS version 12.0 for Windows (SPSS Inc., Tokyo). All data are expressed as mean±standard deviation values, proportions, or absolute numbers. Continuous data were compared using t tests, and categorical data were analyzed using chi-squared or Fisher's exact tests. A P<.05 was considered significant.
Results
Patient characteristics and clinical findings
Age and postoperative follow-up period were significantly different between the two groups. On the other hand, clinical T-factor, stage, method of surgery, and tumor location were not significantly different. The number of patients who received presurgical therapy was 19 and 10 for hybrid EBCS and CBCS, respectively, and all presurgical therapy resulted in a partial response or a complete response (Table 1).
Perioperative outcomes, surgical curability, complications, and short-term follow-up results of hybrid EBCS
In the hybrid EBCS group, the operation time was longer by 30–50 minutes (P<.01) than that in the CBCS group. Blood loss was not significantly different between the two groups. Surgical margins were as follows: 1 case (1.4%) had a positive margin, 4 cases (5.5%) had a margin of <2 mm (close margin), in 9 cases (12.3%) the margin was >2 mm and <5 mm, and 59 cases (80.8%) had a margin of >5 mm. Each case of a positive margin or close margins was diagnosed as ductal carcinoma in situ. Only 1 case with exposed ductal carcinoma in situ in the margin was treated by additional partial resection. In this case, the remnant lesion was identified on the opposite side of the nipple. During the second surgery, the surface of the surgical margin was exposed, and additional resection was performed from a periareolar incision under light guidance. A remnant ductal carcinoma in situ lesion was noted, but the rapid intraoperative and permanent pathological diagnosis was negative margin.
Seven cases (9.6%) of postoperative complications occurred in 6 patients: 4 cases (5.4%) had partial areolar necrosis, 2 cases (2.7%) had partial skin flap necrosis, and 1 case (1.4%) had postoperative bleeding (Table 2). All cases were cured with conservative treatment.
To date, there has been no local recurrence (postoperative observation period period, 18.1±5.6 [range, 12–30] months).
Cosmetic assessment of surgical methods
The JBCS evaluation method showed that the hybrid EBCS group had a better cosmetic result, with less difference in size between the right and left breasts, a less noticeable operative scar, and a higher total score (Fig. 4). Using the 4-point scoring system reported by Winchester and Cox, 13 the hybrid EBCS group demonstrated a better cosmetic result, with a higher portion of patients evaluated as excellent or good (Table 3).
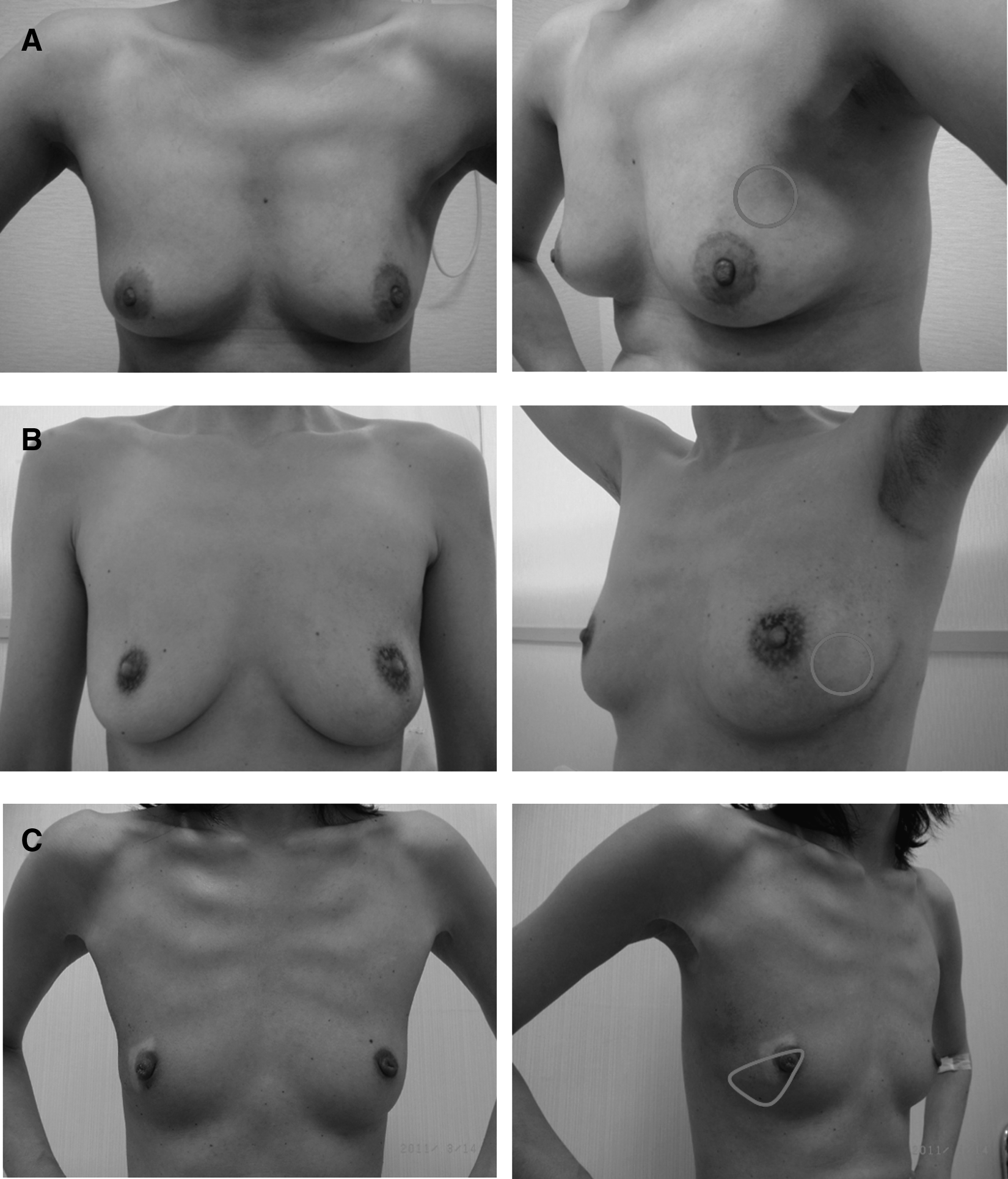
Postoperative appearance after hybrid endoscopy-assisted breast-conserving surgery. Circles and a quadrant line showing the resection lines of the breast tissue.
Elements of the Japanese Breast Cancer Society classification: (1) breast size, 2 points=almost equal (within 10% of difference), 1 point=small difference, 0 points=remarkable difference (>30% difference); (2) breast shape, 2 points=almost equal, 1 point=small difference, 0 points=significantly different; (3) breast scar, 2 points=inconspicuous, 1 point=slightly conspicuous, 0 points=conspicuous, determined from the wideness of the scar (>5 mm), presence of redness/depigmentation, and conspicuousness of scar; (4) breast hardness, 2 points=almost equal, soft, 1 point=slightly hard, partially hard, 0 points=significantly hard; (5) nipple/areolar size and shape, 1 point=no bilateral difference, 0 points=presence of bilateral difference; (6) nipple/areolar color, 1 point=no bilateral difference, 0 points=presence of bilateral difference; (7) nipple position, 1 point=less <2 cm, 0 points=>2 cm, measured using the bilateral difference of the distance from the sternal notch; and (8) position of lowest point of the breast, 1 point=< 2 cm, 0 points=>2 cm, measured using the bilateral difference of the distance from the lowest point of the breast.
On a 4-point scoring system.
Discussion
In this study, we compared hybrid EBCS and CBCS with regard to their surgical and cosmetic outcomes. We also verified the clear margin and risk of complications of hybrid EBCS. Patient characteristics of the two groups were similar except for age and postoperative observational period. As for surgical outcomes, operation time was significantly longer in the hybrid EBCS group, but the amount of blood loss did not differ. In addition, the positive rate of tumor cells in the surgical margin was only 1.4% (1 case), and the incidence rate of postoperative complications was 9.6% (7 cases) in the hybrid EBCS group. To date, no local recurrence has been observed in hybrid EBCS patients (postoperative observation period, 18.1±5.6 [range, 12–30] months). In contrast, the positive rate in the surgical margin was 18.9% (17 cases), and 1 patient (1.1%) showed recurrence of breast cancer in the CBCS group (postoperative observation period, 43.7±22.9 [range, 14–70] months). Postoperative cosmetic evaluation revealed that the hybrid EBCS group had a better result with respect to the shape of the breast and inconspicuous surgical scarring and was not inferior to the CBCS group in other elements of evaluation. Hybrid EBCS was considered a feasible procedure and an effective surgical method for achieving good cosmetic results. To our knowledge, this is the first study to compare postoperative cosmetic evaluation after EBCS and CBCS.
Endoscopy-assisted surgery for breast cancer was introduced more than 10 years ago, and its efficacy and long-term follow-up results have been reported in several Asian countries. Studies have reported that EBCS requires a longer operation time but achieves better cosmetic results.7–9 The advantage of EBCS is that it can be performed through an incision made in an inconspicuous area, preserving its curability with the addition of better cosmetic results.
The important features of our hybrid EBCS method are endoscopic dissection of posterior surface and development of a skin flap with the tumescent method. Using endoscopic assistance gives the advantage that extensive dissection of posterior surface can be performed through a small incision in the axillary area or lateral edge of the breast. Furthermore, an extended good visual field enables us to carry out the surgical procedure and antihemostatic maneuvers to prevent bleeding from small vessels simultaneously, which makes this surgery safe. 14 When we perform this technique, it is important to confirm the location of the penetrating branch of the internal thoracic vessels with US prior to surgery to avoid damaging these vessels during the procedure. Preserving these vessels maintains the blood supply to the preserved mammary glands and also improves the cosmetic result of surgery. An initial training period is needed to become proficient in this endoscopic procedure. Continuous repetition of approximately 20 cases under the supervision of a proficient breast surgeon provides adequate training. In this study, approximately half of the cases in the hybrid EBCS group were operated on by three breast surgeons not proficient in this procedure, because of which the mean operation time became longer. In addition, initial investment is required to purchase a vein retractor, which is used during this surgery. However, the vein retractor is not damaged much by any load because its axis is made of stainless steel. Compared with conventional devices, which can impair scopes when they are damaged, the vein retractor is considered to be useful. Development of skin flaps with the tumescent method is a plastic surgery technique. By injecting a large amount of physiological saline containing epinephrine subcutaneously, extensive subcutaneous hydrodissection is possible. This makes the subsequent development of skin flaps with dissection scissors easy. The procedure reduces blood loss, shortens operation time, and prevents skin burns. Care must be taken to maintain the thickness of the subcutaneous adipose tissue in order to preserve blood flow in the skin flap.15,16 To do so, it is essential that the skin flaps should not be thinner than the layer of subdermal fascia.
Requirement for expensive disposable devices is reported as one of the disadvantages of endoscopy-assisted surgery. 17 However, we use a reusable vein retractor for endoscopic dissection of the posterior surface and the tumescent method for skin flap development, which allows a minimum requirement for disposable devices. 18 The only disposable item we use is a wound protector (Figs. 2e and 3d). The wound protector is necessary to protect the wound and secure the visual field and is not expensive. 17
With regard to the surgical margin, only 1 case had exposed lesion in the margin, and ≥2 mm of free margin was secured in more than 90% of patients. We obtain magnetic resonance imaging images of both breasts in all BCS patients. After accurate evaluation of tumor invasion, US-guided marking was performed for the resection area of BCS. The importance of US-guided conservation surgery for both palpable and nonpalpable lesions has been reported previously.19–23 Moore et al. 21 reported that a longer free margin was secured (7.6 versus 4.8 mm, respectively) and the volume of resected mammary gland was less (104 cm3 versus 114 cm3, respectively) in a US-guided group compared with a palpation-guided group in conservation surgery for palpable lesions. Therefore, it is considered that US-guided marking of the resection area is useful for both palpable and nonpalpable lesions when partial resection of the breast is performed and contributes to postoperative cosmetic satisfaction. Our technique using US-guided marking achieved the same or better results than previous reports, and we believe that hybrid EBCS is able to provide sufficient free margin and good cosmetic results.
In the hybrid EBCS group, no skin burning of the flap was observed, although this is a characteristic complication of EBCS. All patients who had partial skin flap necrosis were early patients who were treated soon after we had started using the tumescent method, and there were no such cases after we became accustomed to the technique.
It is important for BCS to achieve consistent surgical curability and better cosmetic results. It is reported that even after curative BCS, patients can suffer physically and mentally. BCS can negatively affect quality of life in patients when the cosmetic result is not satisfactory. 24 Therefore, it is important to evaluate postoperative cosmetic results of the breast. In this study, we evaluated cosmetic results using two methods. One method was reported by Winchester and Cox 13 and classifies cosmetic results on a 4-point scale: excellent, good, fair, and poor. The second method was developed by the JBCS and evaluates cosmetic results by assessing the symmetry of the entire breast, the nipple, and the areola and scoring the cosmetic results.11,12 Both methods of evaluation revealed that the hybrid EBCS group had better cosmetic results than the CBCS group. The JBCS method showed that hybrid EBCS was superior because of its less noticeable scar. Hybrid EBCS was not inferior to CBCS in all other aspects.
The follow-up period until cosmetic evaluation was shorter in the hybrid EBCS group. However, cosmetic results in the hybrid EBCS group would not worsen over time because appearance of the breast after BCS generally recovers over time in most cases.
The present study has several limitations. The results were obtained from a single institution, and the sample size was relatively small. In addition, the follow-up period was different between the two groups and, especially the follow-up period with respect to in-breast events, was shorter in the hybrid EBCS group. Therefore, further multicenter studies using long-term observational periods are required.
Conclusions
Although the operation time for the hybrid EBCS was longer than that for the CBCS, hybrid EBCS provided sufficient free margin, and its surgical curability was considered equivalent to that of CBCS. Moreover, with regard to cosmetic evaluation, hybrid EBCS was especially superior because of its less noticeable surgical scar and may contribute to improved postoperative cosmetic outcomes. In addition, this operative method is cost-beneficial compared with conventional EBCS because it can be performed with minimal use of disposable devices.
Footnotes
Disclosure Statement
No competing financial interests exist.