
Abstract
Abstract
Introduction:
To present the surgical technique and initial outcomes of bladder neck injection (BNI) of bulking agent under CO2-induced pneumovesicum to better visualize the bladder neck.
Subjects and Methods:
Three children (one 12 year old and two 14 year olds) who underwent polydimethylsiloxane BNI under pneumovesicum for treatment of bladder neck incompetence were retrospectively reviewed. Patient diagnoses included an imperforate anus, joint hypermobility syndrome, and an ectopic ureter, respectively. BNI was performed with an antegrade approach under 10 mm Hg CO2 pneumovesicum after insertion of a 5-mm diameter trocar in the bladder dome. A single injection was given in all cases.
Results:
BNI was successfully completed in all patients. Bleeding that developed during bladder access or injection did not interrupt accurate positioning of the needle or confirmation of mucosal coaptation in the bladder neck. At 6 months postoperatively, all patients reported social continence, defined as minimal incontinence requiring no more than one pad daily. No intraoperative morbidity or postoperative deterioration of the upper urinary tract due to technique was observed.
Conclusions:
Antegrade BNI under pneumovesicum affords better visualization of the bladder neck, resulting in more accurate needle placement and better mucosal coaptation confirmation. Studies of larger patient samples are necessary to better study the efficacy of BNI with the patient under pneumovesicum.
Introduction
In all of the cases described in the literature, retrograde or antegrade injections were performed using endoscopes while instilling irrigation fluid. Recent studies suggest that the antegrade approach offers several advantages, including better visualization and access to the incompetent bladder neck as well as confirmation of accurate needle placement. 8 However, bleeding during bladder access or injection often obscures the operative view, thereby impeding the subsequent procedure.
We investigated the use of an antegrade approach to BNI of polydimethylsiloxane under CO2 insufflation of the bladder (pneumovesicum) for improved visualization. To our knowledge, this is the first study to describe this technique. The surgical technique and its outcomes have been investigated in 3 cases.
Subjects and Methods
Since December 2009, one boy and two girls were treated with BNI of polydimethylsiloxane under pneumovesicum to restore urinary continence. The primary etiologies of the incompetent bladder neck in the 3 patients were an imperforate anus, joint hypermobility syndrome, and an ectopic ureter. Bladder neck surgery was not previously performed in any of the patients. Urodynamic investigations were performed on all patients before injection. All patients had stable and compliant bladders, and detrusor overactivity was not noted. Preoperative leak point pressure was 70, 65, and 63 cm of H2O in each patient. The criteria used to evaluate the results were based on changes of symptom scores. Symptom scores for continence were as follows: grade 0, no wetting; grade 1, occasional dampness; grade 2, wetting managed by one to two pads daily; grade 3, diapers needed with some dry periods; and grade 4, diapers required with wetting throughout the day. 8 For the postoperative upper tract evaluation, we performed a kidney ultrasound 3 months after the operation.
Operative procedure
The patient under general anesthesia was placed in the modified lithotomy position with abducted thighs. First, retrograde cystoscopy was performed followed by instilling irrigation fluid through a cystoscope to distend the bladder. Then, a small skin incision at the midline of the bladder dome was made, and a 5-mm diameter trocar was inserted into the bladder under cystoscopic vision. The anterior bladder wall was suspended to the abdominal wall to prevent trocar slipping. To suspend the bladder wall, a 17-gauge needle was inserted near the trocar, and a loop was made inside the bladder. A 21-gauge spinal needle was inserted into the bladder and passed into the loop, and a 3-0 suture was introduced into the loop through the spinal needle (Fig. 1B). This suture was trapped by the loop and was extracted outside the skin by pulling the loop upward. The suture was then tied. The bladder was emptied, and CO2 pneumovesicum at 10 mm Hg was initiated. A 14.5 French cystoscope was introduced through the port into the bladder, and a 4 French 18-gauge long needle was inserted through the cystoscope bridge.
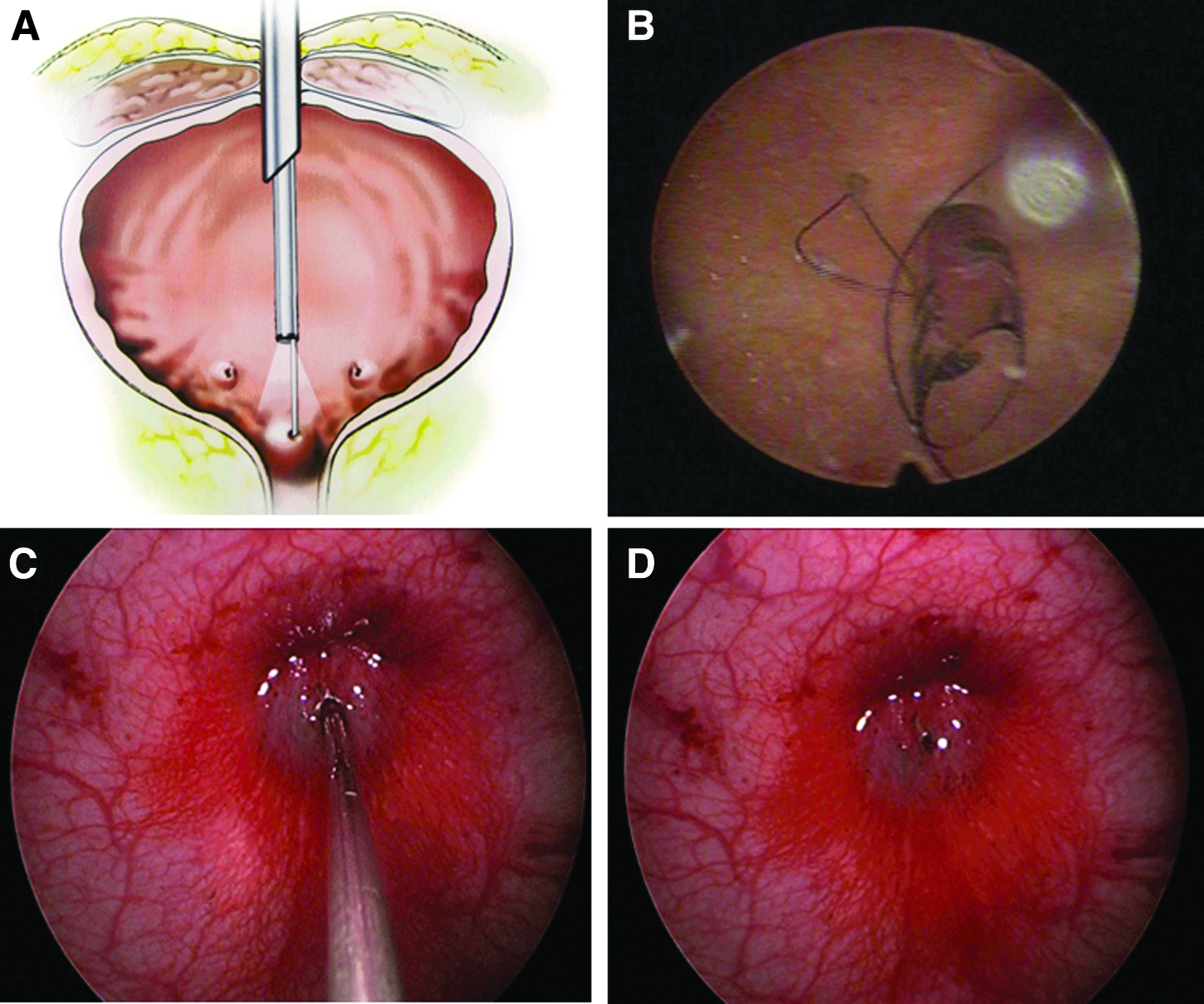
Transvesicoscopic bladder neck injection under pneumovesicum.
Polydimethylsiloxane (Macroplastique®; Uroplasty Ltd., Reading, United Kingdom) was placed just under the mucosa of the bladder neck at the 6 o'clock position under direct vision until visual coaptation occurred (Fig. 1C). If needed, additional agent was injected at the 3 and 9 o'clock positions. Upon completing the injection (Fig. 1D), the cystoscope and trocar were removed, and a 10 French suprapubic catheter was inserted into the bladder through the trocar site without additional incisions. The suprapubic catheter was kept in place for 3 days. Patients were evaluated at 6 months to assess postoperatively whether the injection resulted in the achievement of continence.
Results
Three patients (1 boy and 2 girls) underwent injections of the bladder neck to treat urinary incontinence. A single injection was given in all cases. BNIs were successfully completed in all patients, with good visualization of the bladder neck. Bleeding that developed during bladder access or injection did not interrupt accurate positioning of the needle or confirmation of mucosal coaptation in the bladder. The 12-year-old male patient underwent imperforate anus repair after birth that was not associated with a spinal abnormality. The pretreatment symptom score was 4, which decreased to 2 following injection with 2 mL of polydimethylsiloxane. The pretreatment symptom score of the 14-year-old female patient with joint hypermobility was 3. The post-treatment symptom score decreased to 0 after BNI with 5 mL of polydimethylsiloxane. In the other 14-year-old female patient with an ectopic ureter, injection of 5 mL of polydimethylsiloxane (Fig. 2) decreased the symptom score from 3 to 1. All patients (100%) reported social continence, defined as minimal incontinence requiring no more than one pad daily, at 6 months postoperatively. We performed a kidney ultrasound for the postoperative evaluation of upper tract after 3 months postoperatively, and we could not find hydronephrosis in any of the patients. Also, the post-void residual volume measured less than 20 mL in all 3 patients using ultrasound. There was also no morbidity due to the technique or complaints after surgery, including any complaints of cosmesis.
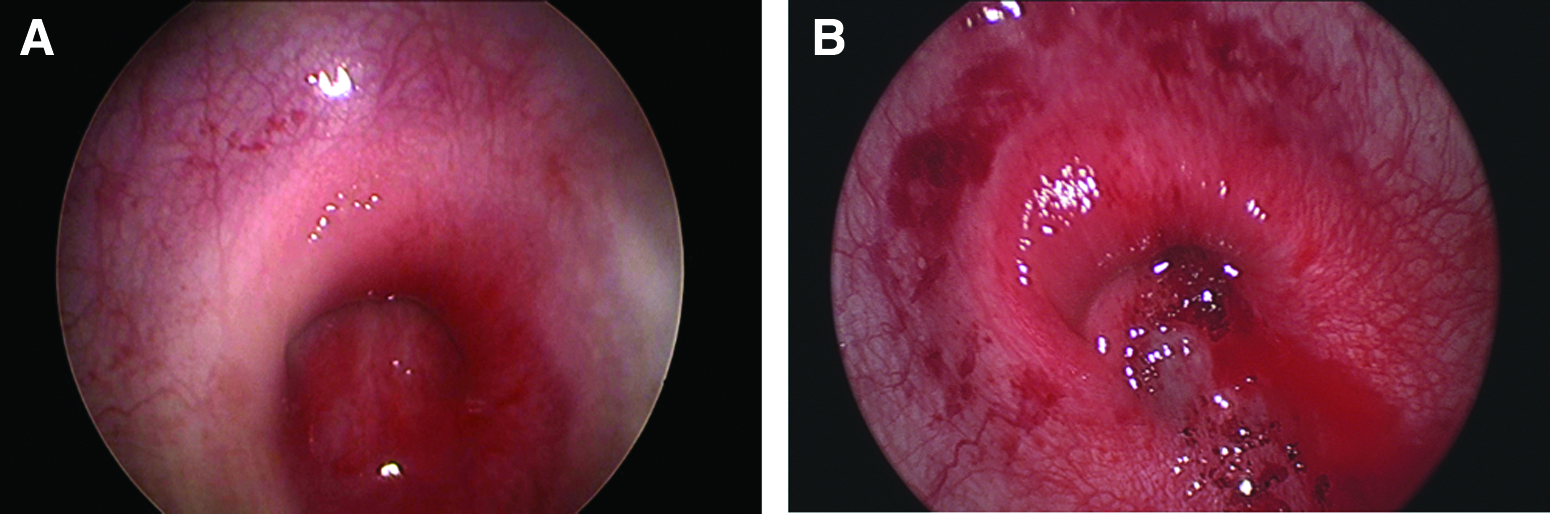
Transvesicoscopic bladder neck injection in a patient with an ectopic ureter: transvesicoscopic view
Discussion
Injections of bulking agents at the bladder outlet to improve continence in children were first reported in 1985. 1 Materials such as polytetrafluoroethylene particles, 1 collagen, 9 and autologous fat 10 have been used to help increase bladder outlet resistance. Dextranomer/hyaluronic acid copolymer and polydimethylsiloxane have recently been used to achieve continence, with favorable results.5,6 The continence rate of BNI was reported to be between 40% and 100% depending on the diagnosis, definition of continence, and duration of follow-up.11–13
Traditionally, bulking agent has been injected in a retrograde fashion using cystoscopic guidance in children with sphincteric incontinence. Antegrade injection has also been described, but its use has been limited to application through a Mitrofanoff stoma. 14 To date, reports of a percutaneous antegrade technique in children have been scarce. Abel and Gough 15 first described the percutaneous antegrade technique in 1996, and Dean et al. 8 reported the results of using a percutaneous antegrade technique as well as a retrograde approach in 34 children. The percutaneous antegrade technique is considered to offer several advantages, including improved visualization and better overall results for appropriate patients. Whether outcomes differ between the retrograde and antegrade approaches remains a matter of debate.
From our experience, the antegrade injection technique has several advantages over the retrograde approach. First, it allows a direct view of the bladder neck. This provides better visualization and access to the incompetent bladder neck, which easily facilitates submucosal needle placement. Second, the antegrade approach permits more free movement for injection. During the retrograde technique, bladder neck bulking in the male means that endoscopic movement is limited to 2 degrees of freedom: forward, back, and rolling. In contrast, the antegrade approach provides 2 additional degrees of freedom: up and down and side to side. Third, antegrade observations of the bladder neck and urethra allow for the direct view of tissue coaptation from above without distending the urethral lumen. This allows the surgeon to better assess the completeness of the procedure and to assess when bladder neck bulking is sufficient.
We treated 15 children with an endoscopic injection of polydimethylsiloxane using the percutaneous antegrade technique in bladders distended with irrigation fluid between 2006 and 2009 (authors' unpublished data). In this series of patients, 60% of patients (9/15) reported social continence, defined as wetting managed by one pad daily at 3 months postoperatively, which is comparable to rates reported in other antegrade injection series. 16 However, we experienced that bleeding developed during bladder access or injection and sometimes spread rapidly through the bladder, which was filled with sterile irrigation fluid. In these situations, it was very difficult to expect improved visualization of the bladder neck, which is considered an advantage of the antegrade approach. The subsequent procedure including accurate needle placement and confirmation of mucosal coaptation would then also be impeded. Visual confirmation of good mucosal coaptation is an important factor to determine procedural completeness because there is no objective way to determine whether the mucosal coaptation is sufficient to resist a specific deficit in stress leak point pressure. Decisions regarding completeness are made only by the surgeon's visual assessment of mucosal coaptation. Dean et al. 8 observed that a good mucosal coaptation detrusor leak point pressure was always greater than 60 cm of H2O and provided visual evidence. However, in our experience it was very difficult to confirm good mucosal coaptation when the operative view was obscured because of intravesical bleeding. Uncertain decisions regarding procedure completeness may lead to poor results.
Since 2010, we have performed percutaneous antegrade injections under CO2 pneumovesicum. The potential benefit of this approach is that bleeding during bladder access does not interrupt the operative view. In all 3 cases, visualization of the bladder neck was better than in cases of antegrade injection with the bladder distended with irrigation fluid. If bleeding developed during bladder access or injection, blood trickled from the bladder neck to the trigone rather than spreading through the irrigation fluid in the bladder when we used sterile irrigation fluid for bladder distension. The improvement in visualization enhanced precise needle placement and confident decisions regarding procedure.
Although the use of antegrade BNI under pneumovesicum has obvious advantages, including better visualization of the bladder neck and mucosal coaptation, whether better visualization improves patient outcomes remains unclear because of the small sample size and short-term follow-up in this study. This is the main limitation of the present study. To perform the antegrade approach using pnemovesicum, we needed to make a small incision about 5 mm to insert the trocar into the bladder. This invasive procedure, in comparison with the other methods including the retrograde approach or the antegrade approach using bladder irrigation, required more hospitalization for recovery. However, using a small incision and more hospitalization days for recovery were not big issues for the patients and parents because the parents wanted a more precise and delicate procedure for their children to improve incontinence all at once.
Nevertheless, antegrade BNI under CO2 pneumovesicum allowed for better visualization of the bladder neck than antegrade injections in bladders distended with sterile irrigation fluid in this study. The antegrade BNI under pneumovesicum approach results in accurate needle placement and better confirmation of mucosal coaptation in the bladder neck. However, studies including a larger patient population and longer follow-up period are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.