
Abstract
Abstract
Background:
Placement of a primary gastrojejunal tube (GJT) can be technically challenging and often requires an open procedure to negotiate the tube past the duodenal sweep into the jejunum. The alternative approach is to first place a gastrostomy tube (GT), which is then changed to a GJT under endoscopic or fluoroscopic guidance after waiting 6–8 weeks to allow the stoma to mature. We report a case series of primary GJT placement using a combined laparoscopic-endoscopic approach.
Subjects and Methods:
We retrospectively reviewed patients who underwent a combined laparoscopic-endoscopic primary GJT placement. Patients' demographics and relevant clinical information were analyzed.
Results:
Six patients (4 male, 2 female) were identified. The median age at the time of operation was 30.2 months (range, 28 days–10 years). Five GJTs were successfully placed laparoscopically/endoscopically, and one procedure was converted to open. The mean operative time was 84 minutes (range, 63–102 minutes). Postoperative abdominal radiography confirmed post-pyloric tube position in all patients. Feedings were initiated on the first postoperative day. One intraoperative complication required conversion to an open procedure. No patients developed postoperative complications.
Conclusions:
Laparoscopic-endoscopic primary GJT placement is technically feasible and an excellent alternative in patients who require transpyloric feeding access.
Introduction
Subjects and Methods
After receiving approval from the Miller Children's Hospital (Long Beach, CA) Institutional Review Board (protocol number 998-11CR), we performed a retrospective review of all patients who underwent combined laparoscopic-endoscopic primary GJT placement at Miller Children's Hospital, between 2004 and 2009. Relevant data, including sex, age, indications for feeding access, surgical outcomes, time to initiate feeds, and complications, were collected and analyzed.
Operative technique
The initial steps of the procedure are similar to the laparoscopic GT insertion described by Georgeson. 1 Once the intragastric position of the needle is confirmed, an extralong guidewire is inserted into the stomach. After serial dilation of the gastrostomy site, a 16 French or 18 French MIC® transgastric-jejunal feeding tube (Kimberly-Clark, Irving, TX), at a predetermined length based on the size of the patient, is inserted over the guidewire into the stomach. An esophagogastroduodenoscopy is then performed. The prefastened silk tie at the tip of the tube is grasped with a biopsy forceps, and the tube is directed into the jejunum (Fig. 1). The stomach is then secured to the anterior abdominal wall. In patients with an existing GT, the gastrocutaneous fistula is intracorporeally closed with an Endo GIA™ (Covidien Surgical, Norwalk, CT), and a different site is chosen for the new GT.
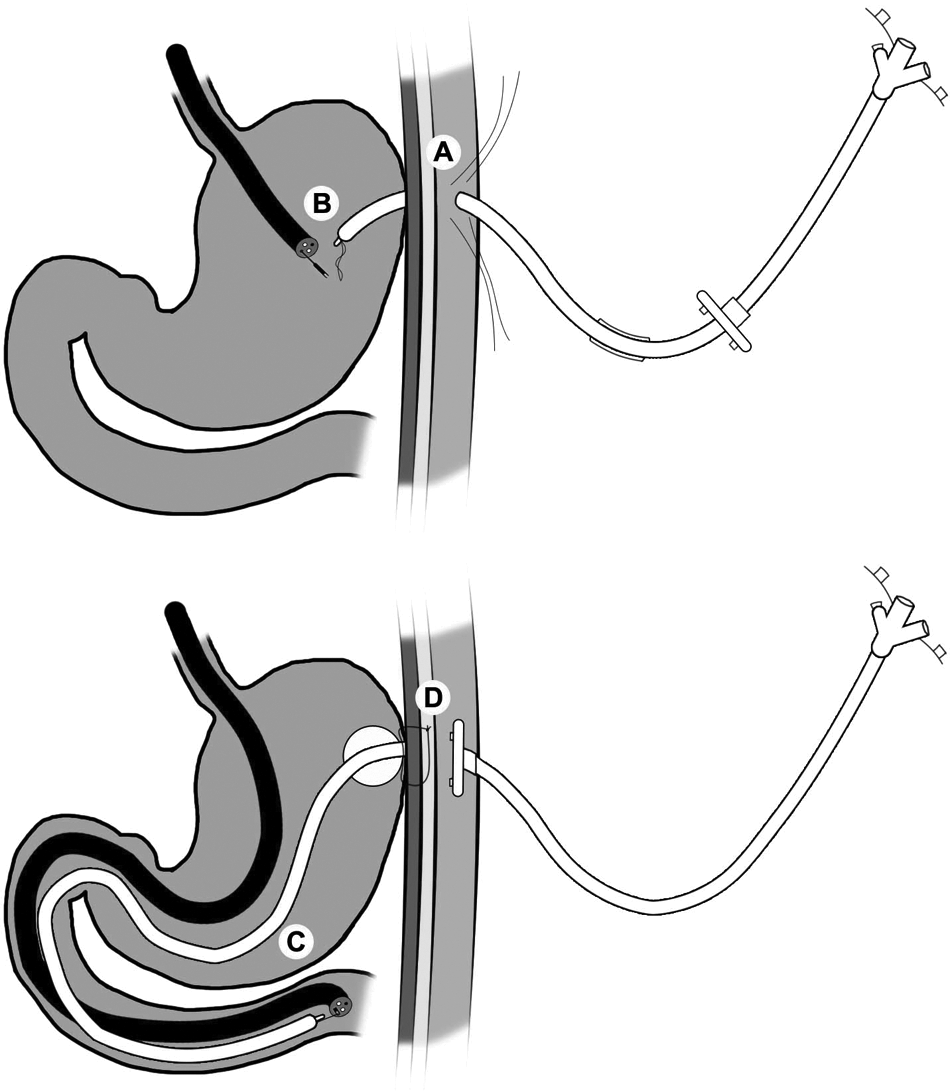
Operative technique.
Results
Six patients (4 males, 2 females) were identified as having had combined laparoscopic-endoscopic GJT placement during our study period (Table 1). All patients were diagnosed with neurological delay and gastroesophageal reflux disease (GERD) proven by pH studies. One patient, who had failed two previous fundoplications and was on GJT feedings, developed significant gastric mucosal prolapse and required closure of the existing gastrostomy site and insertion of a new GJT. In 2 patients, the parents refused fundoplication and GT. A 1-month-old infant, in addition to GERD, had severe oral secretions and oropharyngeal aspiration, which raised concerns of her inability to handle the saliva with the fundoplication. The mean age at operation was 30.2 months (range, 28 days–10 years).
endo, endoscopic; F, female; Fr, French; GERD, gastroesophageal reflux disease; GJ, gastrojejunostomy; GJT, gastrojejunostomy tube; GT, gastrostomy tube; lap, laparoscopic; M, male; MRCP, mental retardation with cerebral palsy; VP, ventriculoperitoneal.
MIC transgastric-jejunal feeding tube from Kimberly-Clark.
Five patients had the GJTs successfully placed using the described method; 1 patient had the procedure converted to an open surgery. The conversion occurred in a 28-day-old infant, who sustained a gastric perforation. During an attempt to negotiate the scope into the duodenum, the “bend” of the scope caused a linear tear in the greater curvature of the stomach. The gastric injury was repaired, and the tube was manually manipulated into the jejunum. The patient recovered uneventfully. The mean operative time was 84 minutes (range, 63–102 minutes). Postoperative abdominal films confirmed proper position of the tubes in all patients. Of the 5 patients with successful GJT placement, feedings were initiated on the first postoperative day. None of the patients developed postoperative complications, aside from hypertrophic granulation tissue and the need for tube replacement. Mean follow-up time of all patients was 3.5 years (range, 2–7 years).
Discussion
Intolerance to oral feeding in children, whether due to GERD or poor gastric emptying, poses a difficult challenge to pediatric surgeons. Consequently, significant numbers of these children end up requiring fundoplication and GT, which remains the third most common pediatric surgical procedure. 2 This procedure, however, is associated with a significant rate of perioperative morbidity. Fonkalsrud et al. 2 and others3–5 reported perioperative complications in nearly 20% and a wrap failure rate approaching 50% in neurologically impaired children. For these reasons, many surgeons advocate placement of a GJT rather than fundoplication and GT in this subset of patients. Srivastava et al. 6 demonstrated that fundoplication/GT and GJT are equally effective in regard to postoperative aspiration pneumonia and mortality. Wales et al. 7 published similar outcomes with fundoplication versus GJT. However, others reported a higher mortality rate with fundoplication than with GJT placement.8,9
Typically, a GJT is placed via an open procedure to negotiate the tube into the small bowel. Commonly, a GT is established first and then switched to a GJT after the stoma is mature, which may take 6 or more weeks. Although these techniques are acceptable, full enteral feeding is often delayed. The clear advantage in our technique is earlier initiation of full enteral feeding. In our series, all the patients who underwent successful combined laparoscopic-endoscopic primary GJT placements had feeds started on the first postoperative day. To our knowledge, this is the first report utilizing a combination of laparoscopy and endoscopy for GJT placement.
A percutaneous approach to accessing the stomach, either radiographically or endoscopically guided, has been used effectively in placing a GJT. However, accessing the stomach with this techniques is considered “blind.” Consequently, hollow viscus injuries are of great concern. Chait et al. 10 reported extragastric misplacement and small bowel transgression in their series. Additionally, Wragg et al. 11 published much higher (14% versus 3.5%) “major” complications (including tube dislodgement, pneumoperitoneum, and viscus injuries) with percutaneous endoscopic gastrostomy than with laparoscopic GT insertion. We identified one gastric perforation in a 28-day-old infant in our series. During an attempt to advance the endoscope into the duodenum, the “bend” or “elbow” of the scope caused a linear tear along the greater curvature. Because laparoscopy was being performed concurrently, the complication was recognized immediately. The procedure was converted to open, the perforation was repaired, and the tube was manually manipulated into the jejunum. The patient recovered uneventfully. We postulate that the small size of the patient may be have been a factor in this complication. Although both endoscopic and laparoscopic gastrostomy placements are well described in the neonatal population, 12 endoscopy is has a higher complication rate in younger children. 13 Futhermore, endoscopy has significant limitations in very small infants due to available equipment. Based on our limited experience, we feel that infants may not be ideal candidates for this procedure.
Although it may not be ideal for all patients, the combined laparoscopic-endoscopic placement of a GJT is a safe and acceptable alternative in a select group of patients. However, this study has several limitations. First, this is a preliminary retrospective review. Second, and more importantly, the cohort in this report is limited in size. More study and review of additional patients are needed to further validate the technique, especially in neonatal patients.
Footnotes
Disclosure Statement
No competing financial interests exist.