
Abstract
Abstract
Background:
Infected urachal remnant is an uncommon benign disease but is generally symptomatic and commonly recurs. The standard of care for this disease is complete resection of all anomalous tissue including a bladder cuff to avoid recurrence. Recent minimally invasive laparoscopic techniques can effectively manage this disease, but multiport laparoscopic techniques are reported to still leave scars outside the umbilicus.
Subjects and Methods:
A novel technique of umbilical laparoendoscopic single-site (LESS) surgery for 2 patients with symptomatic urachal remnant is presented in this study.
Results:
In both cases, the entire urachal tissues from the umbilicus to the anterior bladder dome were successfully excised by the umbilical LESS technique without any extra ports or needlescopes. An articulating needle holder enabled water-tight bladder closure, resulting in early removal of the indwelling catheter. Without any signs of infection, the wound healings were completed 4 weeks after surgery in both cases. The patients had no complaints of symptoms at 6 months and 4 months, respectively, after surgery,and they were quite satisfied with their cosmetic results.
Conclusions:
We propose that the umbilical LESS technique is a promising surgical option for patients with a symptomatic urachal remnant and that this technique provides satisfactory cosmetic results.
Introduction
Recently, this disease has been recognized as one of the good candidates for minimally invasive techniques. Laparoscopic or robotic-assisted surgeries can completely cure the disease, reduce the morbidity of open surgery, and provide better cosmesis compared with conventional open surgery. 6 Nevertheless, various multiport laparoscopic techniques are reported to still leave scars outside the umbilicus.7–16 Here, we reported an umbilical laparoendoscopic single-site (LESS) technique for patients with a symptomatic urachal remnant. This novel approach promises complete excision of urachal tissue from the umbilicus to the dome of the bladder, enables secure bladder closure, and, in addition, provides satisfactory cosmesis for patients.
Subjects and Methods
From August to October 2011, 2 cases of symptomatic urachal remnant were treated with the identical umbilical LESS technique using a single-site access platform and an articulating needle holder.
Cases
Case 1
A 31-year-old man was referred to our hospital complaining of recurring pain and periumbilical discharge. The patient had no other significant history. Ultrasound, abdominal computed tomography scan, and magnetic resonance imaging revealed umbilical abscess and urachal remnant extending from the bladder dome to the umbilicus (Fig. 1).
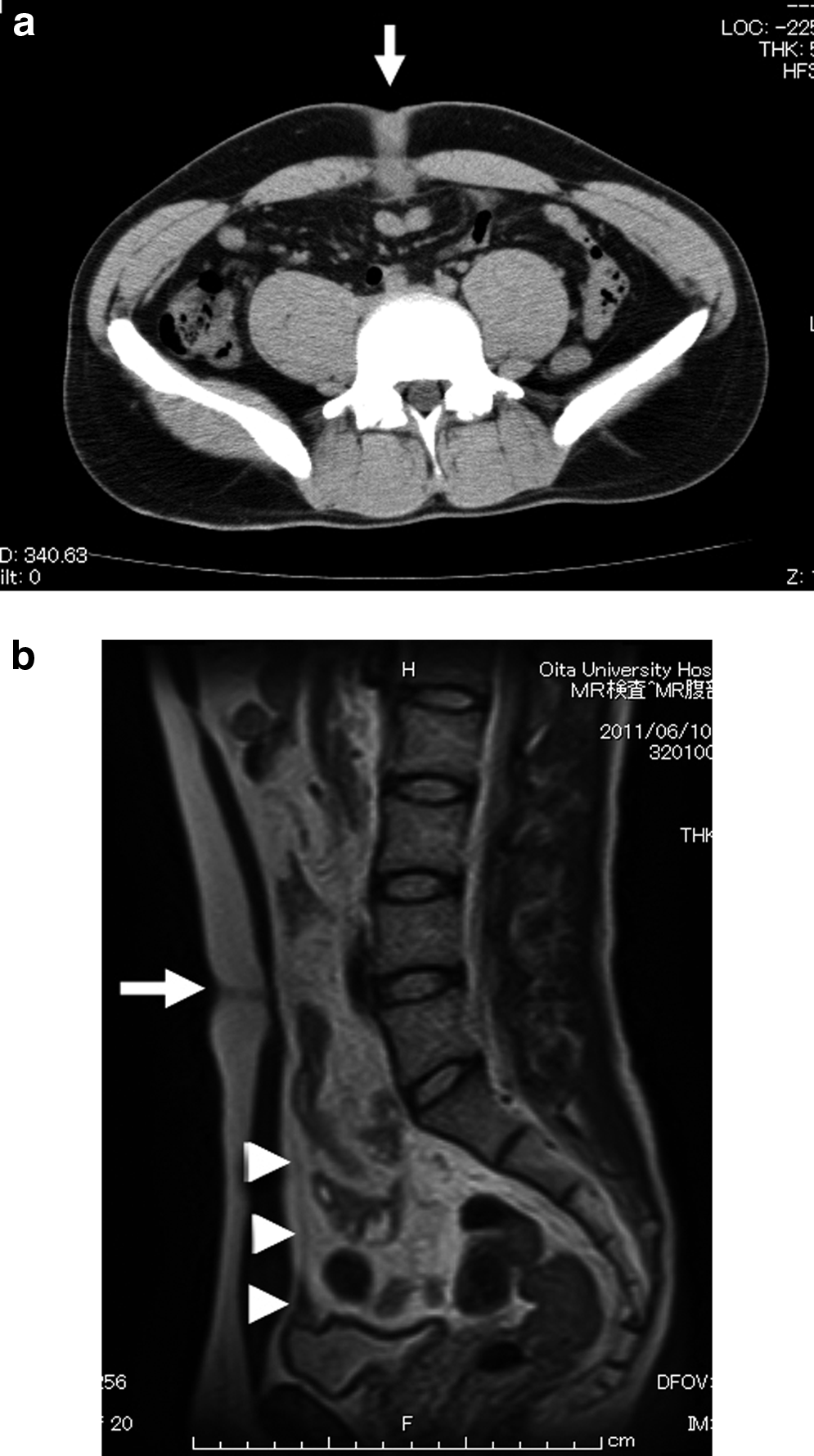
Case 1.
Case 2
A 35-year-old woman presented with complaints of repeated periumbilical discharge and umbilical swelling. The patient had a 10-year history of chronic rheumatoid arthritis, requiring long-term medication. Umbilical abscess and urachal remnant were also diagnosed with ultrasound, abdominal computed tomography scan, and magnetic resonance imaging (Fig. 2).
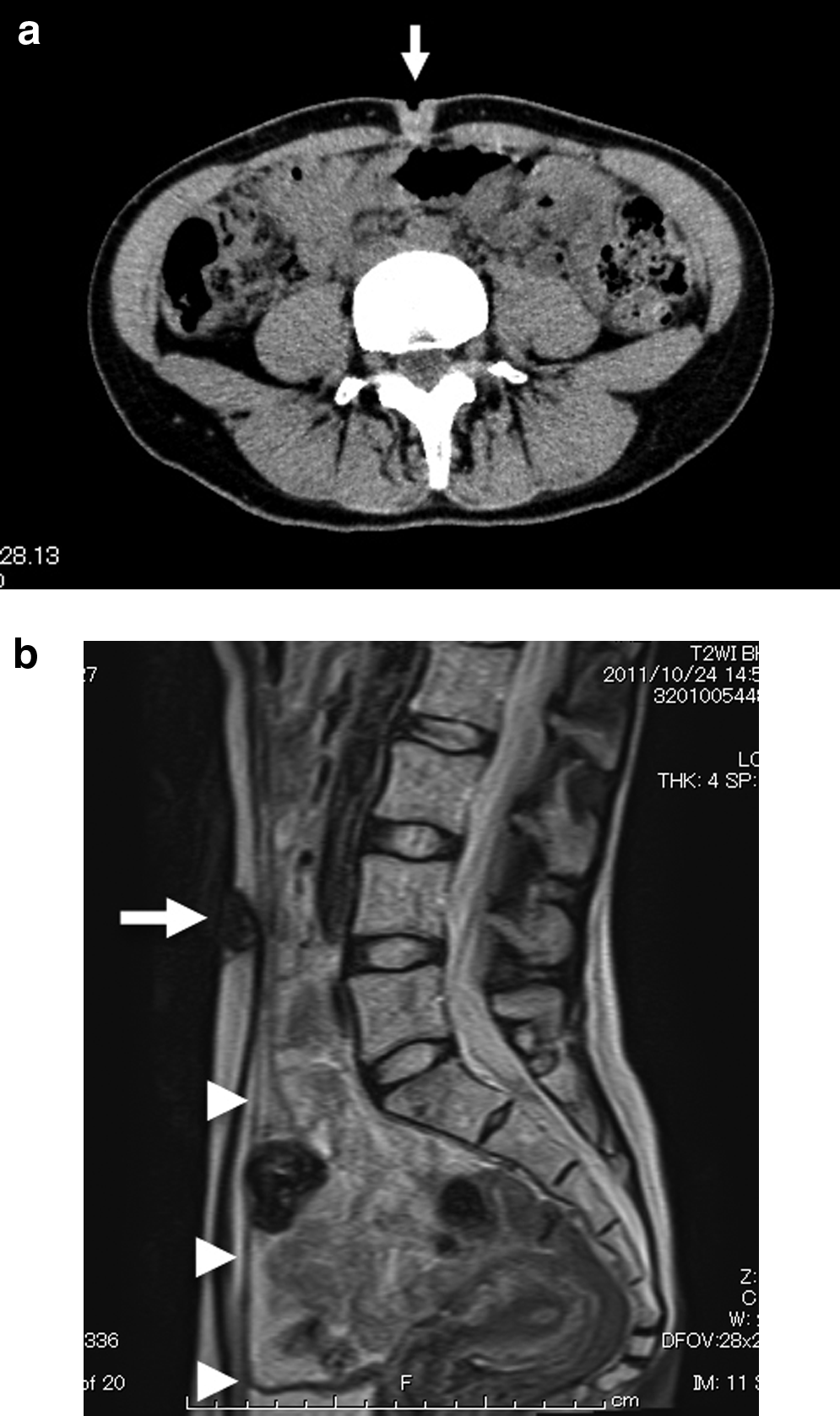
Case 2.
After anti-inflammatory drugs and oral antibiotics resolved their infection symptoms, staged LESS surgery for complete resection of symptomatic urachal remnant was planned.
Techniques
Under general anesthesia, each patient was placed in the supine position. A transurethral Foley catheter was placed into the urinary bladder to distend the bladder. Through a 2.5-cm umbilical skin incision, the subcutaneous tissue was dissected, and the proximal urachal remnant was identified just caudal to the umbilicus. The rectus fascia and peritoneum were incised, reaching the peritoneal cavity, and the umbilical edge of the urachal remnant was transected away from the base of the umbilicus. With the open technique, the urachal remnant was continuously dissected as far distally as possible, reaching about 3–4 cm further. Then, the dissected part was dropped into the abdominal cavity, hanging down from the abdominal wall. Then, the SILS™ port (Covidien, Mansfield, MA), having three trocar insertion sites, was inserted through the 2.5-cm incision (Fig. 3). This device assures three ports, and a 5-mm flexible laparoscope (EndoEye™; Olympus, Tokyo, Japan) and 5-mm conventional laparoscopic devices are mainly used. With electrocautery, the dissection of the urachal remnant with the umbilical ligament continued toward the bladder dome (Fig. 4a). After the bladder was filled with 200–300 mL of air to better define the anatomy, a bladder cuff including the urachal insertion was marked and excised circumferentially using electrocautery (Fig. 4b). The entire urachal remnant from the umbilicus to the anterior bladder dome was freed, and the resected specimen was placed in a 10-mm specimen bag (Endo Catch™ Gold; Covidien). To close the bladder wall, an articulating needle holder (Autonomy™ Laparo-Angle™ needle holder; Cambridge Endoscopic Devices, Framingham, MA) was used. The distal tip of this needle holder bends in any direction mapping the handle motion and turns 360° at any angle by rotating the knob in the handle. The bladder was tightly closed in two layers with 2-0 polyglactin 910 absorbable running suture (Vicryl™; Ethicon, West Somerville, NJ) (Fig. 4c and d). Each patient showed a negative intraoperative leak test filling with 300–400 mL of sterile water. The specimen bag was retrieved, and the SILS port was detached. After the rectus fascia and peritoneum were closed, the bottom of the umbilicus was sutured with the rectus fascia, and the incised skin was closed with absorbable buried suture. A drain tube was not inserted in either case.

Case 1. Intraoperative view shows the SILS port with three trocars via a single umbilical incision. A 5-mm flexible laparoscope, a 5-mm conventional laparoscopic device, and an articulating needle holder are used.
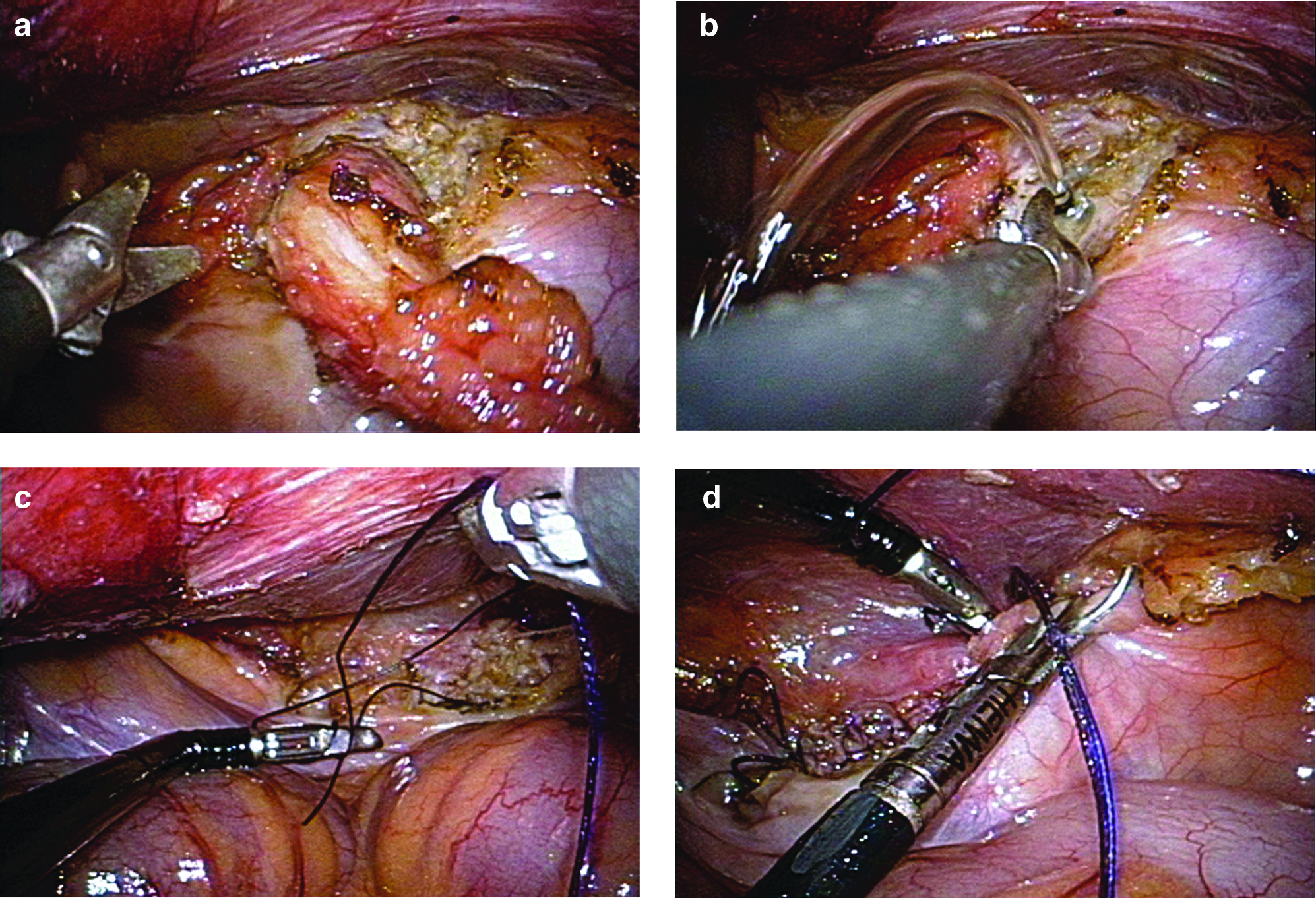
Intraoperative laparoscopic views.
Results
In both cases, the entire urachal tissues from the umbilicus to the anterior bladder dome were successfully excised by the umbilical LESS technique without any extra ports or needlescopes. Operative time and insufflation time were 212 minutes and 136 minutes, respectively, in Case 1 and 220 minutes and 139 minutes, respectively, in Case 2. The blood loss was 10 mL in Case 1 and 5 mL in Case 2. There were no intraoperative complications. The Foley catheter was removed on postoperative Day 3 in Case 1 and postoperative Day 2 in Case 2, and no postoperative complications were noted. The histological evaluation revealed a urachal remnant with chronic inflammation change without any malignant findings. Without any signs of infection, the wound healings were completed 4 weeks after surgery in both cases (Fig. 5). The patients had no complaints of symptoms at 6 months and 4 months, respectively, after surgery, and they were quite satisfied with their cosmetic results.
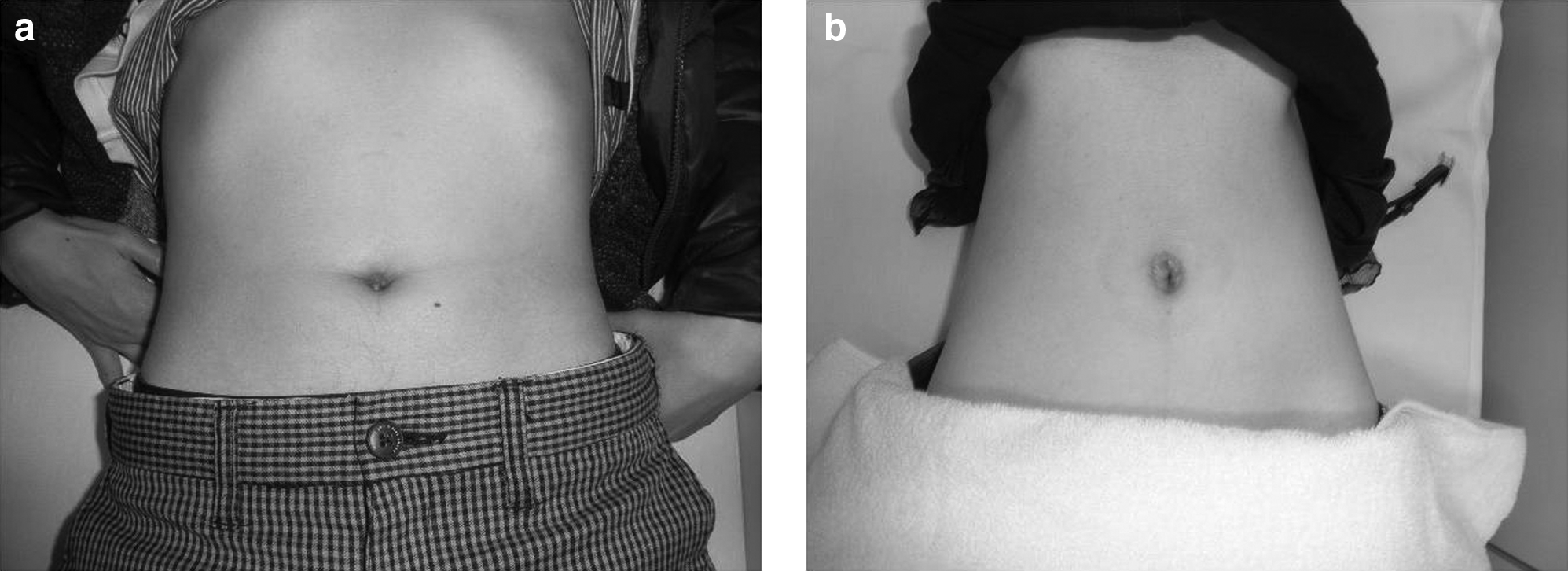
Postoperative views of the patients' abdominal wall 3 months after surgery:
Discussion
After the initial description about laparoscopic resections of the urachal remnant by Neufang et al. 17 in 1992, several reports about laparoscopic technique have been published.7–16 Although each report is a case report or a relatively small case series and some technical variations exist, the laparoscopic technique for the urachal remnant is suggested to be safe and technically feasible, and this procedure can reduce the morbidity of open surgery. Some authors suggested that the laparoscopic technique is more suitable to excise the distal involvement completely because of the better visualization and recognition of the distal urachal structure.7,10,18 It is also suggested that laparoscopic techniques provide better cosmesis, even though multiport laparoscopic techniques have been reported to still leave scars outside the umbilicus.7–18
Today, single-site surgery has been developed in an attempt to further reduce the morbidity and scarring associated with surgical intervention in the fields of general surgery, urology, gynecology. and others. 19 Although the quality of evidence of previous studies about LESS surgeries for urological diseases remains low, the obvious objective benefit of LESS surgeries was supposed to be the improved cosmetic outcome. 20 In terms of treatment strategy for the urachal remnant, the cosmetic outcome is quite important for patients because urachal remnant is basically congenital and a benign inflammatory disease. In this sense, LESS surgery is theoretically more ideal than multiport laparoscopic surgery.
Recently, Patrzyk et al. 21 described a case report of a urachal remnant treated with a single-incision laparoscopic technique. The single incision site they chose was the supraumbilical midabdominal area, and they directly inserted three trocars via a 2.5-cm skin incision without any single-site access platforms. They successfully excised the urachal remnant en bloc with the urachal fistula and closed the bladder wall with absorbable clips. In our cases, the SILS port was inserted via an umbilical incision. We believe that a direct incision on an umbilical site is reasonable to excise the umbilical edge of the urachal remnant and leads to a better cosmetic result. In an attempt to succeed in this umbilical LESS surgery, it should be emphasized that the umbilical edge of the urachal remnant needs to be dissected as far distally as possible by an open surgical procedure. The proximal umbilical part of the urachal remnant is too close to start dissection via an umbilical access site with the laparoscopic technique, and 3–4 cm dissection of the urachal remnant via a 2.5-cm incision is more comfortable with the open surgical technique. After proximal dissection is done reaching about 3 cm further, an effective countertraction and sharp dissection of the urachal tissue can be provided with the umbilical LESS technique. Using this technique, the dissection of the distal urachal remnant and incision of a bladder cuff are performed without any particular difficulty, the same as multiport techniques reported before.7–18
The other point of our LESS technique is the stage of bladder closure. The articulating needle holder we used was quite useful to handle a needle in that challenging aspect, and a tight two-layer running suture yielded negative leak test filling with 300–400 mL of water, resulting in early removal of the indwelling balloon catheter after surgery.
In conclusion, we propose that the umbilical LESS technique is a promising surgical option for patients with a symptomatic urachal remnant, and this technique provides satisfactory cosmetic results.
Footnotes
Acknowledgments
We thank Hachiro Yoshida (Division of Photography and Medical Imaging, Research Promotion Project, Faculty of Medicine, Oita University) and Sean Chidlow (Department of Applied Linguistics, Humanities and Basic Sciences for Medicine, Faculty of Medicine, Oita University) for their support.
Disclosure Statement
No competing financial interests exist.