
Abstract
Abstract
Background:
The aim of this study was to delineate the learning curve of single-port laparoscopic appendectomy for noncomplicated appendicitis.
Patients and Methods:
Thirty patients who underwent single-port laparoscopic appendectomy between July 2009 and June 2010 were compared retrospectively with 30 prior consecutive patients who underwent surgery in the three-port manner. Operative duration, number of conversions, time to resumption of oral intake, length of hospital stay, and complications were used as the indicators of the learning curve.
Results:
Demographics were similar between the single-port and three-port groups. A significant decrease in operative duration was noted after a surgical experience of 10 patients. An operative duration equivalent to that of the conventional three-port method could be achieved after 30 cases.
Conclusions:
Single-port laparoscopic appendectomy is a safe and feasible procedure. The learning curve could be overcome safely without major complications. Our preliminary analysis showed that 30 cases are sufficient to achieve an equivalent operative duration compared with conventional three-port laparoscopic appendectomy.
Introduction
Patients and Methods
From July 2009 to June 2010, in total, 418 patients who presented to our emergency department with right lower abdominal pain were diagnosed with acute appendicitis by either clinical manifestations or imaging studies. Abdominal computed tomography and ultrasonography were performed depending on clinical presentation. The patients who decided on nonoperative treatment were excluded; thus a total of 338 cases underwent either laparoscopic appendectomy or open appendectomy. During this period, 33 patients underwent single-port laparoscopic appendectomy, and 30 patients were diagnosed as having noncomplicated appendicitis intraoperatively. Complicated appendicitis was defined as either a perforated appendix or abscess formation due to perforation. In order to standardize the surgical procedures, all single-port laparoscopic appendectomies were performed by one surgeon. The charts of this surgeon's 30 consecutive prior patients who had undergone three-port laparoscopic appendectomy prior to the study were also reviewed. Data and outcomes were compared between patients who received single-port laparoscopic appendectomy (single-port group) and those who received three-port laparoscopic appendectomy (three-port group).
Patient demographic data, including age, sex, body mass index, and imaging study results, were recorded. Intraoperative data, including operative duration, use of the Surgitie™ loop (Covidien, Mansfield, MA), use of energy devices including LigaSure™ (Covidien) and the Harmonic® scalpel (Ethicon, Blue ASh, OH), and conversion from single-port to three-port laparoscopic appendectomy, were recorded as well. In addition, postoperative data regarding the time to resumption of oral intake, the length of hospital stay, and complications were reviewed.
Operative method
Single-port laparoscopic appendectomy was performed with the patient under general anesthesia and endotracheal intubation. The operative port was created through an infraumbilical incision. A wound protector (Alexis®; Applied Medical, Rancho Santa Margarita, CA) was positioned over the infraumbilical incision, and a number 6.5 sterile surgical glove was placed on the wound protector. Three working ports (10 mm, 10 mm, and 5 mm) were inserted into the first, third, and fifth fingers of the glove, respectively. A 30° 5-mm laparoscope was inserted through a 10-mm working port. After the abdomen was inflated with carbon dioxide, the patient was placed in the Trendelenburg position and tilted to the left side. The operator and first assistant (scope-holder) stood on the patient's left side and performed the appendectomy by using the endo Babcock™ (Covidien), hook electrocautery, energy device (including LigaSure and Harmonic scalpel), endoclips, Surgitie, and endodissectors. The surgery was initiated by ligation of the appendiceal vessel by either endoclips or energy devices depending on the operative situation. After the appendiceal base was identified, the ligation of the appendix was carried out either by Surgitie loop or by endoclips.
Statistical analysis
Data analysis was performed using SPSS version 17.0 (SPSS Inc., Chicago, IL) and R version 2.11.1 (R Foundation for Statistical Computing, Vienna, Austria) software. In statistical testing, two-sided P value ≤.05 was considered statistically significant. Continuous variables were expressed as mean±standard deviation values. Categorical variables were presented as frequency and percentage. In univariate analysis, Fisher's exact test and one-way analysis of variance were used as appropriate for group comparisons.
Then, multivariate analysis was conducted by fitting multiple linear regression models to identify important predictors of operative duration. To ensure the quality of analysis results, basic model-fitting techniques for (1) variable selection, (2) goodness-of-fit assessment, and (3) regression diagnostics were used in our regression analysis. The generalized additive models were applied to detect nonlinear effects of continuous covariates. The coefficient of determination (R2) was examined to assess the goodness-of-fit of the fitted final multiple linear regression model, which is equal to the square of the correlation between the observed and predicted values of outcome variables.
Results
Baseline characteristics
In total, 30 consecutive patients with noncomplicated acute appendicitis treated with single-port laparoscopic appendectomy from July 2009 to June 2010 were enrolled in this study. There were 10 men and 20 women with a mean age of 39.0 years (range, 19–77 years). There was no significant difference in average body mass index between the groups of single-port laparoscopic appendectomy (n=30) and three-port laparoscopic appendectomy (n=30). The preoperative image study including computed tomography and ultrasonography did not show a significant difference between these two groups of patients either. Also, all appendices were checked by pathologists and evenly distributed between the single-port and three-port groups (Table 1).
AA, acute appendicitis; ASA, acute suppurative appendicitis; BMI, body mass index; CT, computed tomography.
Operative results
The usages of dissection instruments did not significantly differ between the single-port and three-port groups (Table 2). The comparisons of five learning curve-related variables, including operative duration, number of conversions, time to resumption of oral intake, length of hospital stay, and any complications, between the single-port and three-port groups are shown in Table 3. The operative duration of single-port groups was longer than that of three-port groups (85.8 minutes versus 72.0 minutes, P=.048). One case among the first 10 cases (Series 1) was converted from the single-port method to conventional three-port laparoscopic appendectomy because of severe local inflammation of the appendix. Patients of the single-port group resumed oral intake on average at 0.4 days versus 0.8 days in the three-port group (P=.110). The mean length of hospital stay was 47.2±29.5 hours in the single-port group and 51.6±25.7 hours in the three-port group (P=.542). No statistical difference was found between these two groups of patients in the results of the time to resumption of oral intake and the length of hospital stay. Two complications occurred in Series 1 of the single-port group, one fever and one ileus, and both were improved after conservative treatment with antibiotics. Also, no patient developed major complications during hospitalization.
P value was calculated between the four groups by the overall F-test of analysis of variance.
Energy device includes LigaSure or the Harmonic scalpel.
P value was calculated between the four groups by the overall F-test of analysis of variance.
P value was calculated within the four groups; statistical significance was compared with that of Series 1.
Learning curve
The recruited 30 patients who underwent single-port laparoscopic appendectomy were sequentially in time divided into three groups of 10 patients: Series 1 (the first 10 cases), Series 2 (the second 10 cases), and Series 3 (the third 10 cases). As shown in univariate analyses (Table 3), the learning curve-related five variables were compared across the three consecutive single-port groups and the three-port group. The mean operative durations in the Series 2 and Series 3 of the single-port groups and the conventional three-port group were significantly shorter than that of Series 1 (102.6±29.1 minutes versus 79.5±27.2 minutes versus 75.3±25.0 minutes versus 72.0±23.7 minutes, P=.017). Although no statistical difference was found in operative duration among Series 2, Series 3, and the three-port group, the tendency was that the operative duration was shortened with the accumulation of experience. No statistical differences were found in number of conversions, time to resumption of oral intake, length of hospital stay, and number of complications among the four groups of patients.
It was not feasible or ethical to randomize the 30 consecutive patients in the single-port group into the three series of 10 patients. To reduce the effects of confounding variables such as patient's age, body mass index, and severity of appendicitis, multivariate analysis of the predictors of operative duration was conducted by fitting multiple linear regression models. We found that the operative duration was significantly associated with the temporal order of patients' surgeries (especially for Series 1), body mass index, severity of appendicitis, and the use of Surgitie loop (Table 4). After adjusting for the effects of all the other significant predictors, the nonparametric smoothing plot from the fitted generalized additive models for modeling the mean value of operative duration revealed that cases in Series 1 had a much steeper downward slope (–1.5 minutes/case) than those in Series 2 and 3 (–0.65 minutes/case) (Fig. 1).
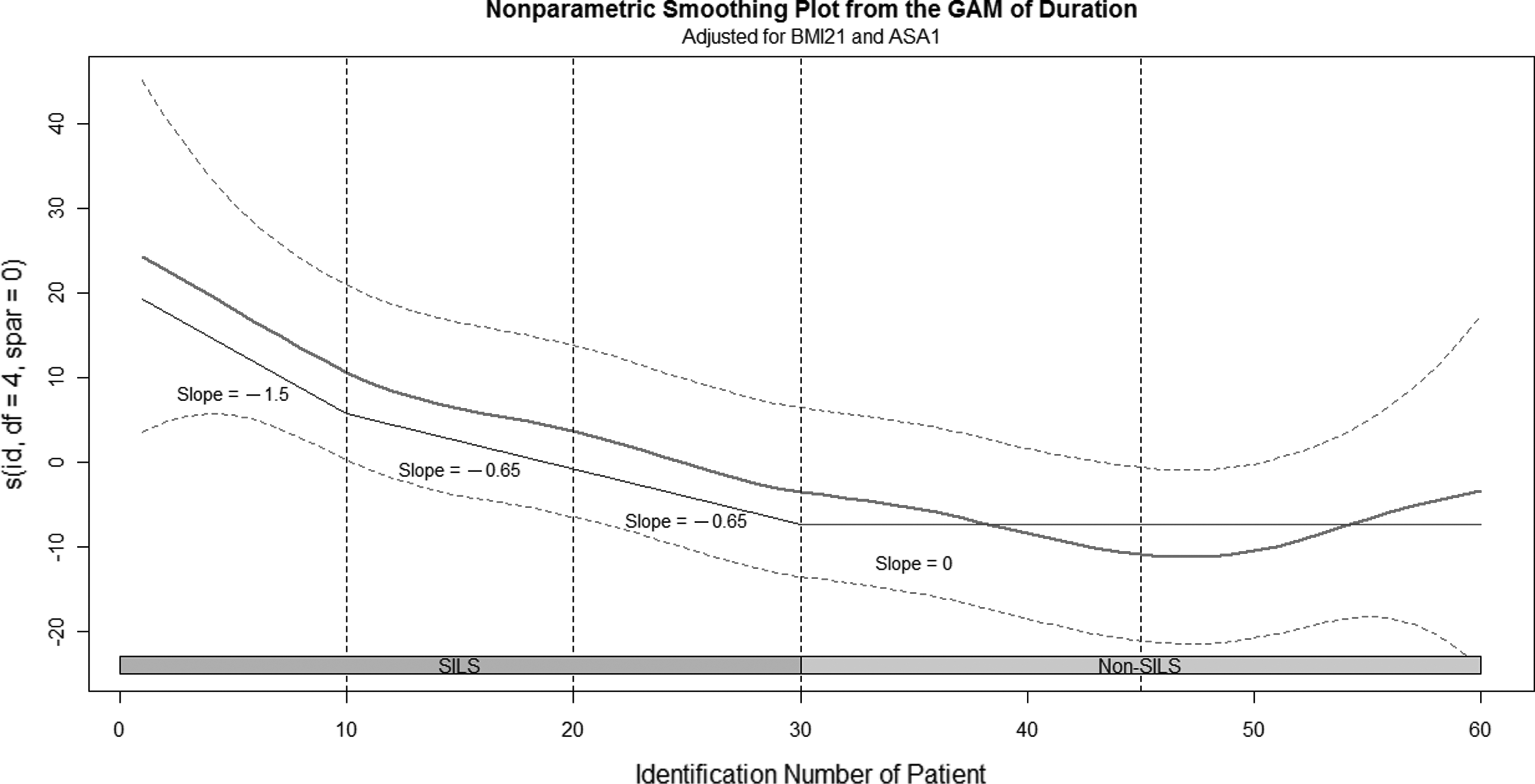
Nonparametric smoothing plot from a generalized additive model (GAM) for modeling the nonlinear effect of accumulated cases over time on the mean value of operation duration. Operative duration decreases as more cases were experienced in the single-port group. The first 30 cases were treated by single-port surgery, and those in Series 1 have a much steeper slope (–1.5 minutes/case) than the slope (–0.65 minutes/case) of Series 2 and Series 3, assuming the control group has a nearly horizontal slope. Clearly, the learning effect is strongest in Series 1 and accumulates in the next two series. ASA, acute suppurative appendicitis; BMI, body mass index; SILS, single-incision laparoscopic surgery.
By the multiple linear regression model: n=60, residual standard error=21.7 (df=55), R2=0.405, overall F test statistic=9.36, P<.0001 (df=4, 55).
ASA, acute suppurative appendicitis.
Discussion
Our main finding was that significant improvement in operative duration was accomplished after the first 10 cases. We showed that an experience of 30 cases achieved an operative duration equivalent to conventional three-port laparoscopic appendectomy.
In an attempt to achieve a less invasive procedure, modifications of laparoscopic appendectomy have been proposed such as either minimizing the size of the ports or decreasing the number of ports.14,15 Innovations have been introduced for surgical procedures such as the use of needlescopic surgery or the utilization of appendix-traction methods.16,17
Despite the introduction of many techniques for single-port laparoscopic surgery, the procedures have not been standardized.4,5,18,19 For single-port laparoscopic appendectomy, procedures vary mainly in the setting of multiple-port systems, including the introduction of commercialized multiple-instrument access ports or the placement of surgical gloves upon the wound protector to facilitate multiple-instrument access.20,21 The latter method was used in our study, and some procedures were modified compared with the original one such as the size of the ports and the instruments introduced.
Concern remains regarding the cost-effectiveness of learning and performing single-port laparoscopic appendectomy. High technical complexity was encountered because of limited operative view, difficult retraction, coaxiality of the instruments, and compromised manipulation. 11 Reports have shown that the operative duration of single-port laparoscopic appendectomy is slightly longer than that of the three-port laparoscopic procedure. 22 Furthermore, obstacles exist in managing complicated appendicitis.9,11–13,20,23,24 The conversion rate to conventional three-port laparoscopic appendectomy is increased in cases of complicated appendicitis.9,12,20,22,25
Although many parameters have been described to evaluate the learning curve of conventional three-port laparoscopic appendectomy, including blood loss, complication rate, conversion rate, operative duration, and length of hospital stay, the last two have been used most frequently.26,27 For surgeons completely unfamiliar with laparoscopic surgery, the minimum experience required to achieve a notable decrease in operative duration and length of hospital stay is reported to be around 20 cases.27,28
We observed that the operative duration decreased as the surgeon's experience with single-port laparoscopic appendectomy increased, which is most likely because our surgeon had already been well trained to perform conventional laparoscopic surgery. An experience of 10 cases was sufficient to reduce operative duration. With the accumulation of surgical experience, the operative duration for single-port laparoscopic appendectomy may reach nearly an equivalent operative duration to that of three-port laparoscopic appendectomy (Fig. 1).
Our series did not show a significant reduction in complications, conversions, and length of hospital stay. It is reported that the maturation of skills of conventional laparoscopic appendectomy can minimize the complication rate to less than 10%.24,28 A possible explanation for the finding that the number of complications encountered in the single-port laparoscopic appendectomy group is small may be that single-port laparoscopic appendectomy can be safely performed early in the learning curve by surgeons who are already experienced in conventional laparoscopic surgery. 29
In our series, all conversion was avoided with the accumulation of surgical experience except 1 patient in Series 1 of the single-port group, which can be explained by the surgeon still being at the beginning in developing single-port skills.
No differences were found in length of hospital stay among the three sequential series of single-port patients. It is interesting that the length of hospital stay shortened in the single-port group compared with that of the conventional three-port group, although the result did not reach statistical significance. Early discharge after appendectomy can be attributed to various factors. 30 Because our average length of hospital stay was only 2 days (47.2 hours), it is too short to display significant differences compared with the hospital stay of other groups.
Two limitations exist in our study. The first is that our learning curve is only the reflection of the experience of a single surgeon. More data should be collected to delineate the learning curve of a general population of surgeons. Second, 3 cases of complicated appendicitis were encountered and underwent single-port laparoscopic appendectomy in our consecutive series. Because an improvement in operative duration was observed after 10 cases, we suppose that the learning effect of the three cases is small and negligible. We suggest that a further prospective study should be done to minimize the bias.
In conclusion, although postoperative results of the single-port laparoscopic appendectomy are similar to those of conventional three-port laparoscopic appendectomy, including the time to resumption of oral intake and hospital stay, our results encourage us to believe that the single-port laparoscopic appendectomy may be an alternative choice in the emergency setting. Our study demonstrates that a surgeon who already has experience with three-port laparoscopic appendectomy can quickly and easily overcome the learning curve for single-port laparoscopic appendectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.