
Abstract
Abstract
Background:
Portal vein system thrombosis (PVT) is an infrequent but potentially serious complication after laparoscopic splenectomy. Patients with β-thalassemia are at higher risk as they have splenomegaly and hypercoagulability.
Subjects and Methods:
Forty-eight β-thalassemia patients who underwent hand-assisted laparoscopic splenectomy or laparoscopic splenectomy were studied prospectively with pre- and postoperative Doppler ultrasonography or computed tomography scanning.
Results:
The incidence of PVT was 8.3% (95% confidence interval [CI] 0.2%–16.4%) (4 of 48 patients). Spleen weight was the only independent factor associated with the presence of PVT. The odds ratio for spleen weight (100 g increase) was 1.46 (95% CI 1.10–1.94, P=.010). Receiver operator characteristic curve analysis showed that the optimal cutoff of spleen weight to the prediction of PVT was 1543 g. Thrombosis resolution was observed after a median of 165 days.
Conclusions:
Patients with β-thalassemia who undergo laparoscopic-assisted splenectomy are at high risk of postoperative PVT. Close postoperative surveillance and aggressive coagulation prophylaxis are needed in these patients. Larger studies are required to confirm the present findings.
Introduction
Progressive and significant splenomegaly is a common finding in β-thalassemia patients, often requiring splenectomy. 3 These patients are at a hypercoagulable state due to diverse factors (deregulation of nitric oxide homeostasis, thrombophilia, increased platelet aggregation, formation of reactive O2 species, hepatic-cardiac-endocrine dysfunction) 4 and are at high risk of thrombosis.
The aim of this prospective exploratory study was to determine the incidence and identify risk factors of PVT after laparoscopic-assisted splenectomy in a high-risk patient group.
Subjects and Methods
Between 2005 and 2010, 48 β-thalassemia patients with symptomatic splenomegaly and/or hypersplenism (worsening anemia with increased transfusion requirements) underwent surgery. Perioperative data were entered prospectively in a database. All patients had preoperative abdominal ultrasound or computed tomography scan with no evidence of PVT, used desferrioxamine or deferiprone, and had been immunized against Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis 1–3 weeks before surgery.
The majority of patients underwent hand-assisted LS (HALS), and the surgical technique has been described previously in detail. 5 In brief, the operative strategy consisted of sequential performance of a HALS through a Pfannenstiel incision, a laparoscopic cholecystectomy, and laparoscopic wedge liver biopsies. The rest of the patients underwent standard LS. Selection of the procedure was based to the surgeon's preference.
All patients were given low-molecular-weight heparin the afternoon before the operation and postoperatively starting 12 hours after the operation for 7 days. Since the publication of the European Association for Endoscopic Surgery guidelines, 6 patients were maintained on low-molecular-weight heparin (2500 IU) for 4 weeks postoperatively. All patients were prescribed long-term oral penicillin (at least 1 year) after discharge.
Doppler ultrasonography of the portal vein system was performed on postoperative Day (POD) 7 and POD 30 or when indicated according to patients' symptoms. As the symptoms of PVT often are only vague (diffuse abdominal pain, nausea, fever, ileus, diarrhea, and decreased appetite), patients with nonspecific abdominal symptoms were promptly investigated by radiological imaging.
Once the diagnosis of PVT was established, the patient was given oral anticoagulants (warfarin) for at least 6 months. These patients were followed up with Doppler ultrasound or computed tomography scans every 2 months until thrombosis resolution.
Statistical analysis
Quantitative values are expressed as median (with interquartile range [IQR]). Qualitative variables are expressed as absolute and relative frequencies. Fisher's exact test was used for the comparison of proportions. For the comparison of quantitative variables between the study groups, nonparametric Mann–Whitney tests were used. In order to find independent factors associated with portal vein system thrombosis, stepwise multiple logistic regression analysis was conducted (P for removal was set at .1 and P for entry was set at .05). Odds ratios with 95% confidence intervals (CIs) were computed from the results of the logistic regression analyses. Receiver operator characteristic analysis was used to determine the optimal sensitivity and specificity of various cutoff values of spleen weight for the prediction of portal vein system thrombosis. It was estimated that with the current sample size the study had 85% power to detect an effect size of 1.5 or more for the difference (α=0.05). All reported P values are two-tailed. Statistical significance was set at P<.05, and analyses were conducted using STATA statistical software (version 8.0; STATA Corp., College Station, TX).
Results
Patient characteristics and perioperative data are presented in Table 1. Forty-five patients (94%) had homozygous disease, 18 patients (38%) had hepatitis C virus infection with no preoperative evidence of cirrhosis or hepatic malignancy, and 81% underwent HALS. There was one perioperative death (mortality 2%). This patient underwent cardiac arrest in POD 1 due to cardiac tachyarrhythmia and succumbed in the intensive care unit 20 days later.
HALS, hand-assisted laparoscopic splenectomy; HCV, hepatitis C virus; IQR, interquartile range; LS, laparoscopic splenectomy; SD, standard deviation.
Four of 48 (8.3%; 95% CI 0.2%–16.4%)) patients developed PVT after surgery, including 1 patient who had concomitant splenic vein thrombosis. Details of diagnosis and outcome are presented in Table 2. No other thrombotic events (peripheral or central) or any other complications during the period of PVT occurred in the patients described.
F, female; HALS, hand-assisted laparoscopic splenectomy; LS, laparoscopic splenectomy; M, male; POD, postoperative day; PV, portal vein; SMV, superior mesenteric vein.
No significant differences were found in terms of age, gender, type of surgery, operating time, conversion, complications, duration of hospital stay, spleen length, preoperative hemoglobin, and positivity for hepatitis C virus between patients who developed PVT and those who did not (Table 3).
By Fisher's exact test.
By Mann–Whitney test.
HALS, hand-assisted laparoscopic splenectomy; HCV, hepatitis C virus; IQR, interquartile range; LS, laparoscopic splenectomy; PVT, portal vein thrombosis.
The median operating time for LS was 250 minutes (IQR, 150–200 minutes) and was significantly greater compared with the median operating time of HALS, which was 180 minutes (IQR, 130–210 minutes) (P=.024).
The weight of the resected spleen was significantly greater in patients with PVT than in those without (P=.014). Table 4 shows the association of patient's parameters with the presence of PVT. Significantly greater values of activated partial thromboplastin time (lupus anticoagulant-diluted [LA-AM]) were found for patients with PVT. When multiple logistic regression analysis was conducted in a stepwise method, it was found that spleen weight was the only independent factor associated with the presence of PVT. The odds ratio of spleen weight (100 g increase) was 1.46 (95% CI 1.10–1.94, P=.010), indicating about 50% greater likelihood for PVT for every 100 unit increase in spleen weight. Receiver operator characteristic curve analysis (Fig. 1) demonstrated an area under the curve equal to 0.86 (95% CI 0.64–1.00) and showed that the optimal cutoff of spleen weight to the prediction of PVT was 1543 g with a sensitivity of 75%, specificity of 92.3%, positive predictive value of 50%, and negative predictive value of 97.3%.
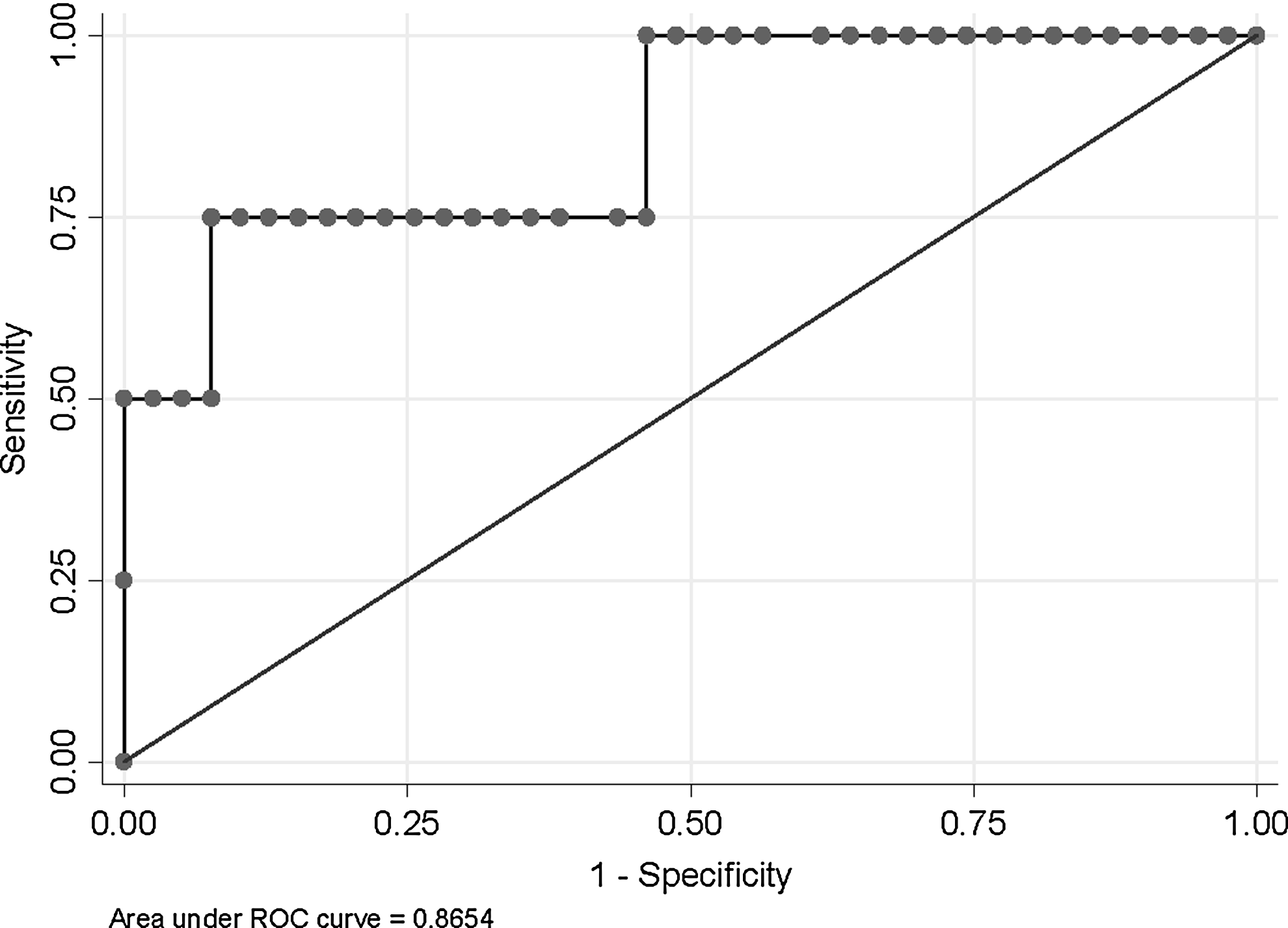
Receiver operator characteristic (ROC) curve for the prediction of portal vein thrombosis PVT from spleen weight.
By Mann–Whitney test.
Fisher's exact test.
APPT (LA), activated partial thromboplasin time (lupus anticoagulant); APPT (LA-AM), activated partial thromboplastin time (lupus anticoagulant-diluted); ATIII, antithrombin III; PTT, partial thromboplastin time; INR, international normalized ratio; PT, prothrombin time; AXAGPL, anti-factor Xa in GPL (U/ml); ACAMPL, anti-cardiolipin antibodies in MPL (U/ml); APC-R, resistance to activated protein C; dRVVT, dilute Russell's viper venom time; KCT, kaolin clotting time; WAG, von Willebrand factor antigen.
Discussion
The present study found that the incidence of PVT in a group of high-risk patients with β-thalassemia was 8.3%. Portal/splenic vein thrombosis occurs after splenectomy, and the incidence in a cumulative review was 8.3% in 395 patients studied prospectively. 1 The reported incidence of portal/splenic vein thrombosis after LS varies widely between 9.8% and 52.5% in prospective studies (total incidence of 23% in 148 patients) and 0.35% and 5.6% in retrospective studies (total incidence of 2.2% in 491 patients).1,7 Furthermore, the incidence of portal/splenic vein thrombosis after splenectomy for hereditary hemolytic anemias was 12.3%. Thus the incidence in the present series—although high—is within the reported range. There is a paucity of well-designed controlled trials but there is no difference in the incidence of PVT between open surgery and LS. 1
The main risk factor for PVT is spleen size and not the method of splenectomy. Patients with splenomegaly and increased spleen weight are at higher risk of PVT after LS.8–10 The median spleen weight of all patients in the present study was 871 g but was 1781 g in patients who developed PVT. Spleen weight was the only risk factor in the logistic regression analysis, and this is in accordance with the findings of a Japanese study. 10
Platelet count of more than 650×103/μL and D-dimer level of >500 μg/mL were associated with the development of PVT in previous studies,2,11 but these were not confirmed for the patient population described here (P=.815 and P=.809, respectively; Table 4).
Patients with β-thalassemia have a high prevalence of thromboembolic events due to a hypercoagulable state.4,12 This is a result of a combination of various abnormalities: activated platelets, alteration in red blood cells with the formation of reactive O2 species and expression of negatively charged phospholipids, expression of endothelial adhesion molecules on endothelial cells, decreased levels of antithrombin III, protein C, and protein S, and dysregulation of nitric oxide homeostasis. 4 There were no significant differences in any of the laboratory parameters presented in Table 4. It should be noted that PVT happened despite the routine use of perioperative prophylaxis with low-molecular-weight heparin in the described patient population, and this can be attributed to the combination of splenomegaly and hypercoagulability. Although it has been shown that thromboembolic events occurred 4.38 times more frequently in thalassemia intermedia compared with thalassemia major, 13 there was no difference in the occurrence of PVT between these groups in the present study.
A Japanese study found that splenic vein diameter >8 mm is a risk factor for PVT. 7 In the present study the diameter of the portal vein was measured in 10 patients and was found to be an insignificant factor in the multivariate analysis (11 mm versus 18 mm).
The median time of PVT occurrence after splenectomy is reported between 5 and 12 days (average, 1 week), 1 but it can occur as long as 99 days after the operation. This is the reason the programmed screening in this study was done on POD 7 and 30. In a recent study from Canada, 7 of 9 patients with PVT were diagnosed by 1 week. 14 The median time of PVT diagnosis in the present series was a little longer, at 14.5 days.
There was one perioperative death in this series due to postoperative cardiac arrhythmias. Cardiac disease related to transfusional iron overload is the leading cause of death in patients with β-thalassaemia major. 15 Early myocardial iron deposition predates decreased left ventricular dysfunction. The risk ratio of cardiac death was 2.2 in the age group of 20–30 years and 3.3 at the age of 30–40 years, and the annual risk of cardiac death was 0.67% and 0.56%, respectively, according to a recent study. 15 The age of the deceased patient was 37 years.
Morbidity after HALS has been reported in the range of 16%–35%16–18 and in cases with significant splenomegaly reaches 56%. 19 Forty-four percent of patients in this series had postoperative complications, although the majority were minor (lung atelectasis). This is mainly because β-thalassemia patients have pulmonary dysfunction, which includes restrictive lung disease, impaired diffusing capacity of lung for carbon monoxide, small-airway disease, and obstructive airway disease. 20
Although the impact of thrombocytosis on the incidence of PVT is not yet clear, long-term antiplatelet therapy for high-risk patients has been recommended.8,21 However, the level of evidence for this is low (Level of Evidence 4). 6 The authors are following the recommendations of the European Association for Endoscopic Surgery consensus, which state that perioperative anticoagulant prophylaxis with subcutaneous heparin should be applied for all patients (Grade of Recommendation C). 6 Patients at high risk for portal and/or splenic vein thrombosis should receive anticoagulant prophylaxis for 4 weeks (Grade of Recommendation C). 6
There are limitations in our exploratory study. There were only four outcomes of interest in a series of 48 patients. Concerning the basic hypothesis, which is the difference in spleen weight between patients with thrombosis and patients without thrombosis, it was estimated that with the current sample size the study had 85% power to detect an effect size of 1.5 or more for the difference (α=0.05). Larger studies are needed to confirm the findings of this series.
In summary, β-thalassemia patients who undergo laparoscopic-assisted splenectomy require aggressive coagulation prophylaxis and close follow-up for the development of PVT.
Footnotes
Disclosure Statement
No competing financial interests exist.