
Abstract
Abstract
Background:
Optimal treatment of intrathoracic hydatid diseases in adults involves complete removal of the cyst with parenchyma-preserving surgery. In current practice, thoracotomy remains the standard surgical approach for pulmonary hydatid cysts, so surgical experience is limited, particularly with regard to video-assisted thoracoscopic surgery (VATS).
Subjects and Methods:
Between June 2007 and May 2011, a selected series of 12 adult patients presenting with intrathoracic hydatid cysts underwent VATS. The cysts were completely removed using a three-trocar technique.
Results:
Complete removal of the cysts was successful in all patients. All cysts were diagnosed by computerized tomography, and 6 (50%) patients had a history of hydatid disease in the liver or lung. No serious postoperative complications were observed. Patients with thoracoscopic excision were discharged after a median of 2.9 days (range, 2–6 days). No recurrences or complications were observed during a mean follow-up of 29 months.
Conclusions:
Considering the conversion and complication rates in our series, VATS should be the primary therapeutic choice for adults with thoracic hydatid cysts. Open surgical interventions in patients with large and uncomplicated cysts appear optional.
Introduction
Treatment for thoracic hydatid disease includes complete surgical removal of cysts. 3 The standard surgical approach is open surgery (thoracotomy), which is notorious for involving a painful surgical wound, and it can also lead to respiratory complications and chronic pain syndrome. 4 In our study, a selected series of patients with pulmonary and intrathoracic but extrapulmonary (mediastinal) hydatid cysts who underwent video-assisted thoracoscopic surgery (VATS) were evaluated in terms of reliability of the method and appropriate patient selection.
Subjects and Methods
Patients
From June 2007 to May 2011, 115 patients underwent surgery for treatment of thoracic hydatid disease. Of these, 12 (10%) underwent VATS. Computerized tomography of the thorax was the diagnostic tool used for all patients with hydatid cysts. Additionally, 6 (50%) patients had a history of hydatid disease in the liver or lung; these diagnoses were confirmed histologically in 2 patients with complicated cysts using fine needle biopsy because of suspected malignancy. Table 1 lists the patients' characteristics. Echinococcal cysts were removed via VATS if (1) no previous thoracotomy had been conducted on the site, (2) the pulmonary cyst was <4 cm in diameter, (3) the cyst was localized peripherally, (4) the patient had a maximum of three cysts, and (5) the cysts were localized in the mediastinum.
F, female; FEV1, forced expiratory volume in 1 second; LLL, left lower lobe; LUL, left upper lobe; M, male; Med, mediastinal; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe.
Surgery
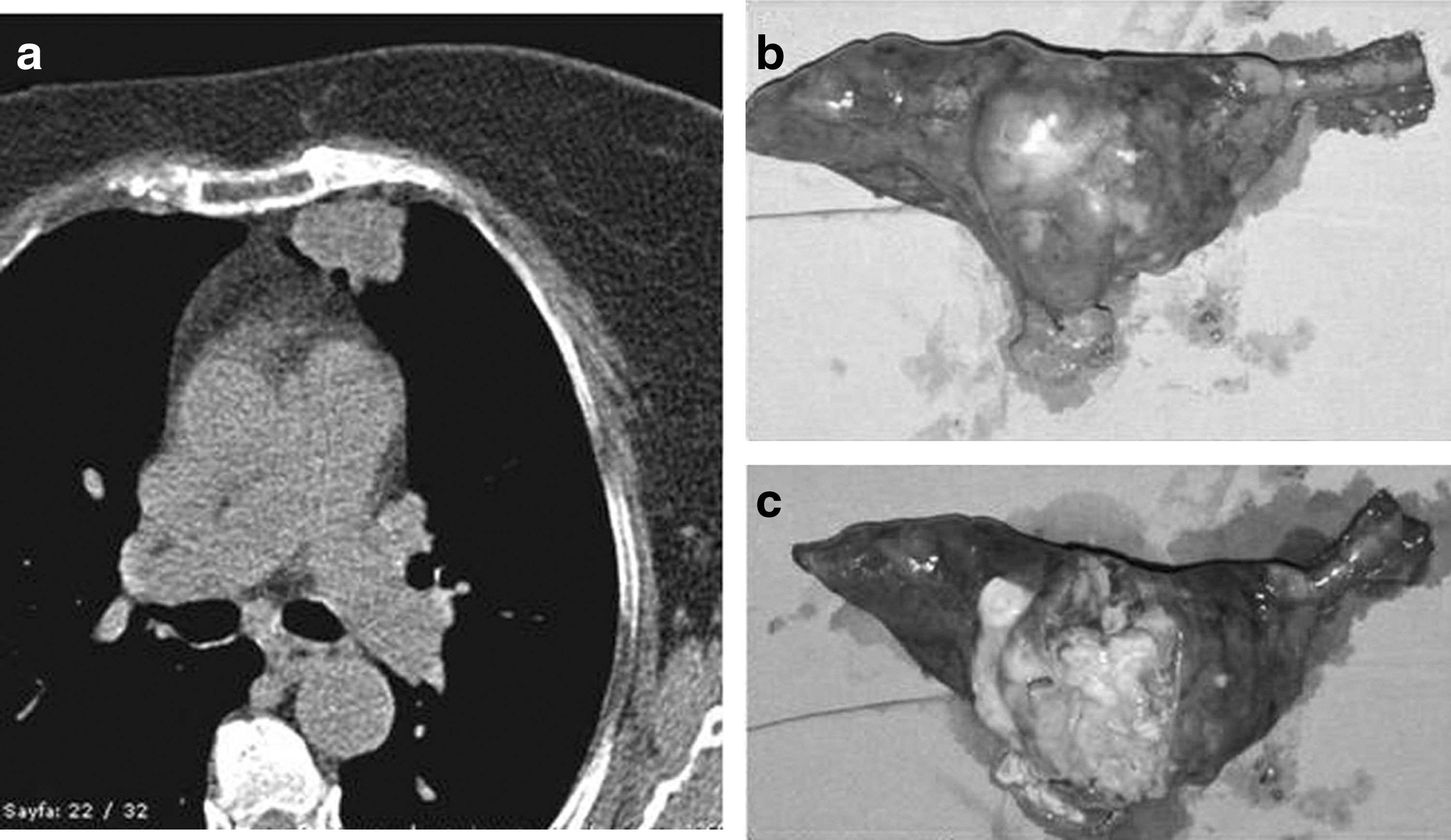
VATS was performed with the patient under general anesthesia with double-lumen intubation. The three-port (11-mm trocars) technique was used with the patient in the lateral decubitus position. Pulmonary echinoccocal cysts were removed through wedge resection (by using a stapler) with safety margins of the parenchyma (Fig. 1). Mediastinal cysts were removed completely with a portion of surrounding fat and pleural tissue. Hydatid fluid was aspirated before any intact and large cysts were excised from the thorax. A large-bore (24–28 French) chest tube was inserted into the camera port in each patient and evacuated in the first 48 hours.
Results
In total, 12 patients underwent 13 operations to treat intrathoracic hydatid cysts. Their mean age was 32.3 years (range, 18–78 years). Of the 12 patients, 8 (67%) patients were female, and 4 (33%) were male. Three patients (25%) presented with intact pulmonary cysts, 5 (42%) with ruptured pulmonary cysts, and 4 (33%) with mediastinal intact cysts. Only 1 patient presented with bilateral cysts. VATS was successful in all patients. Surgeries took 30–100 minutes (mean, 51.5±21.7 minutes), and no patient required conversion to thoracotomy. The mean length of hospital stay was 2.9 days (range, 2–6 days). Histopathology revealed E. granulosus in all patients. No operative or hospital deaths were observed in the series, and no patients had a major complication. Prolonged hospitalization (6 days) because of an air leak was the only minor complication. Patients were followed up for 10–55 months (mean, 29 months). The follow-up period was uneventful, and no recurrences were observed.
Discussion
Echinoccocal cysts are a major problem in endemic areas, particularly in developing countries. The liver and lungs are the most common sites for the parasite. 3 Treatment for a pulmonary hydatid cyst involves complete excision with maximal preservation of the lung parenchyma. 5 Cystotomy or cystotomy plus capitonage are preferred surgical methods in both complicated and uncomplicated types of hydatid cysts. 6 Nonanatomic resections such as pericystectomy and wedge resection and anatomic resections such as segmentectomy and lobectomy may be required in cases of complicated thoracic hydatid disease. 7 The surgical principles of cystotomy include avoiding rupture of the cyst and controlling bronchial air leaks in the residual cavity. Extreme care is recommended during enucleation of the cyst to avoid spilling parasitic material into the surgical field. 8 Bronchial air leaks from the cyst cavity may cause serious complications such as empyema and bronchopleural fistula following removal of pulmonary cysts.
As a minimal invasive surgery, VATS has become standard practice for mediastinal and pulmonary cysts. In hepatic echinococcal cysts, minimal invasive surgery (laparoscopy) has proven itself in terms of feasibility and safety.9,10 However, echinoccocal cysts of the thorax are still candidates for open surgery (thoracotomy). Surgical treatment of pulmonary hydatid cysts via VATS, such as parenchyma-preserving surgery, with cystotomy plus capitonage, has some limitations, including difficulties controlling bronchial air leaks and the risk of perforation during enucleation of the membranes. The video-assisted mini-thoracotomy approach may allow enucleation and capitonage of the cysts 11 ; however, this method cannot be considered as completely minimally invasive surgery because of the need for spreading of the ribs and a skin incision of more than 5 cm. In our series, 8 (70%) patients with pulmonary hydatid cysts underwent wedge resection via VATS with the three-port (trocar) technique. Complicated and uncomplicated (intact) types of echinoccocal cysts were completely removed. Postoperative functional capacities of the patients did not deteriorate because only a small amount of healthy lung parenchyma was sacrificed during wedge resection of the cysts.
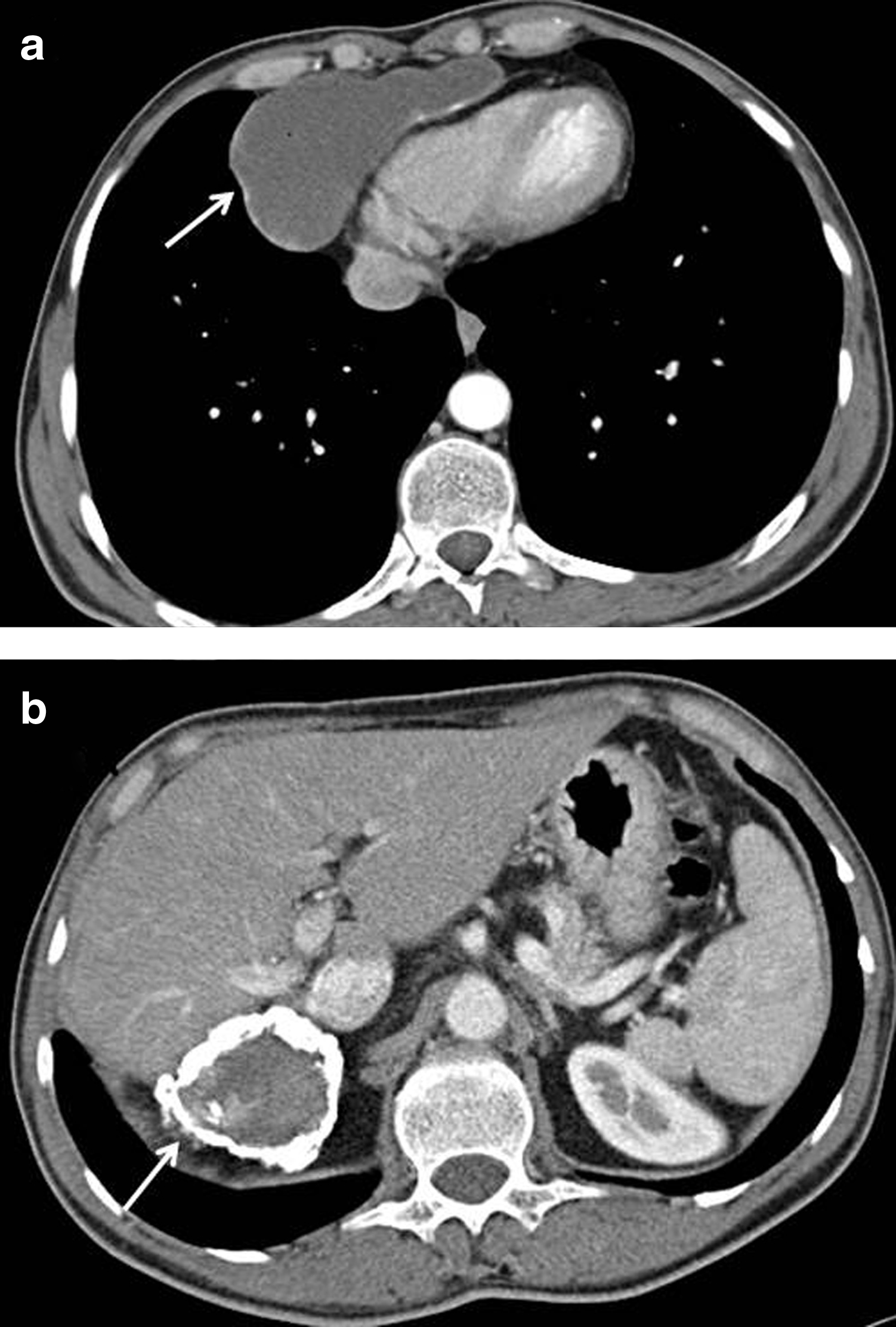
Mediastinal echinoccocal cysts are rare and represent only 0.1%–4% of all hydatidosis cases. Most mediastinal echinococcosis involves secondary cysts that occur as a result of ruptured paramediastinal cysts or penetration and migration of a subdiaphragmatic cyst. 12 Primary mediastinal hydatid cysts are very rare and make up only 0.1% of hydatid diseases. 13 Eroğlu et al. 14 reported a series of 427 operated intrathoracic hydatid cysts, of which only 11 (2.6%) were mediastinal cysts. Differential diagnosis of a mediastinal hydatid cyst is very difficult because imaging findings and clinical symptoms may not provide a clear distinction between congenital and infectious cysts. In our series, all mediastinal cysts were secondary cysts and constituted 3.4% of the series. Patients with mediastinal cysts presented with a history of liver hydatid disease (Fig. 2). Unlike pulmonary hydatid cysts, mediastinal cysts were removed regardless of size and location. These cysts were enucleated and aspirated before being removed from the thorax.
Thoracotomy incisions provide a wide range of exposure, so all thoracic surgical procedures can be applied. However, major disadvantages such as postoperative early and chronic pain, diminished shoulder and respiratory function, and cosmetically unappealing scar tissue directed us to less invasive surgery. 4 The known advantages of VATS, including less pain, shorter hospital stay, and better cosmetic and functional results, were applicable here as well. In our series, cosmetic results were as important as pain and duration of hospitalization because most of the patients were young. VATS was also a safe method not only for early but also late outcomes. No recurrences were observed during the 29-month mean follow-up.
In conclusion, this study demonstrated that VATS resection of intrathoracic hydatid cysts is feasible and safe for selected patients. Although only small and peripheral pulmonary echinoccocal cysts may appear to be suitable for VATS, central and large cysts are also candidates for this less invasive surgical technique. Mediastinal hydatid cysts are also eligible for VATS, but the surgeon should be very careful to prevent rupture.
Footnotes
Disclosure Statement
No competing financial interests exist.