
Abstract
Abstract
Objective:
This meta-analysis was designed to assess the feasibility and safety of laparoscopic right hemicolectomy for colon cancer.
Research Design:
A systematic search of the MEDLINE, EMBASE, and Cochrane databases identified 12 studies that met the inclusion criteria for data extraction. Publications that compared laparoscopic right hemicolectomy and open right hemicolectomy for treatment of colon cancer in the past 20 years were collected for review. The primary outcomes used for meta-analysis were operating time, blood loss, number of harvested lymph nodes, time to first flatus, postoperative hospital stay, postoperative complications, mortality, and rate of recurrence.
Results:
Twelve studies that included 1057 patients were examined. Of these patients, 475 and 582 had undergone laparoscopic right hemicolectomy and open right hemicolectomy, respectively. There were significant reductions in blood loss, time to first flatus, postoperative hospital stay, and rate of wound but a operating time for laparoscopic right hemicolectomy compared with open right hemicolectomy. Other outcome variables such as number of harvested lymph nodes, postoperative complications except wound infection, mortality, and rate of recurrence were not found to be statistically significant for either group.
Conclusions:
Compared with open right hemicolectomy, laparoscopic right hemicolectomy has the advantages of minimal invasion, faster recovery, and a lower rate of wound infection, and it can achieve the same degree of radicality and short-term prognosis as open right hemicolectomy. The drawback is that the operative time is longer.
Introduction
Several meta-analyses on laparoscopic resection of colorectal cancer have been published and indicated that laparoscopic surgery can benefit patients with colorectal cancer.4–6 However, these meta-analyses covered too many entities, and the heterogeneity of different tumor sites and different surgical procedures may have affected the reliability of the results. LRH is technically complex because it involves laparoscopic mobilization of the colon over a wide area, intracorporeal division of major vessels, extraction of specimens, and bowel anastomosis. 7 The feasibility and safety of LRH in the treatment of colon cancer have yet to be tested. Therefore, to systematically and objectively assess the value of LRH for treatment of colon cancer, we performed a meta-analysis of data from clinical studies that have compared LRH with open right hemicolectomy (ORH) over the past 20 years.
Materials and Methods
For the purpose of this study, LRH was defined as laparoscopic dissection, mobilization, and resection of right hemicolectomy and its corresponding mesentery. The anastomosis may be performed either intra-abdominally or extracorporeally. Mortality was defined as 30-day mortality.
Search strategy
The publications were identified by searching the major medical databases such as MEDLINE, EMBASE, and the Cochrane Library for relevant articles published between January 1991 and April 2012. The search strategy was as follows: “(laparoscopic OR laparoscopic assisted OR laparoscopy assisted) AND right hemicolectomy AND (colon cancer OR colon carcinoma).”
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) clinical studies that compared LRH versus ORH for treatment of colon cancer between 1991 and 2012; (2) patients with primary right-sided colon cancer; and (3) raw data that included most of the following: operation time, blood loss, number of harvested lymph nodes, exhaust time, hospital stay, complications, mortality, and recurrence.
Exclusion criteria were as follows: (1) emergency operation; (2) no ORH as a control; (3) recurrent colon cancer, non-primary colon cancer, or benign colon diseases; and (4) duplicate publication or publication that did not provide sufficient data.
Quality of literature
We used a stars scoring system 8 based on criteria related to study design, comparability of patient groups, and outcome assessment to assess literature quality. The total score was 9 stars, and the quality of each study was graded as level 1 (0–5 stars) or level 2 (6–9 stars).
Data extraction
Three researchers extracted data from each study by using a structured sheet and entered the data into a database. The extracted information comprised the author, year of publication, source journals, sample size, research design, operative time, blood loss, number of harvested lymph nodes, time to first flatus, period of hospital stay, rate of complication, mortality, rate of recurrence, and 5-year survival rate. Other data, such as conversion rate and reason for conversion, were noted. Data from duplicate studies were analyzed once only.
Statistical analysis
Statistically, it was not possible to combine the analysis of mean and median, and only data in the form of mean and standard deviation values were included in the meta-analysis. Therefore, continuous variables such as median or range were excluded. In this meta-analysis, weighted mean differences (WMDs) were used for the analysis of continuous variables, and odds ratios (ORs) were used for dichotomous variables. Random-effect models were used to identify heterogeneity between the studies. 9 Heterogeneity was assessed using the chi-squared test. The 95% confidence intervals (CIs) were established. A value of P<.05 was considered to indicate statistical significance. Statistical analyses were performed using Review Manager version 4.2 provided by the Cochrane Collaboration.
Results
According to the search strategy and inclusion criteria, in total, 12 clinical studies that included 1057 right hemicolectomies (475 LRH and 582 ORH) were considered suitable for meta-analysis. The search and exclusion strategy is displayed in Figure 1. The characteristics of the 12 clinical studies (1 randomized controlled trial 13 and 11 retrospective studies10–12,14–21) are shown in Table 1. Quality assessment of the reported studies is shown in Table 2, and each study has a score of more than 6 points.

Combined Dukes' stages A+B.
LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; RCT, randomized controlled trial, RNT, retrospective nonrandomized trial.
Selection for treatment: 1, inclusion criteria reported; 2, representability of patients undergoing laparoscopic right hemicolectomy to population undergoing surgery for right-sided colon cancer; and 3, representability of patients undergoing open right hemicolectomy to population undergoing surgery for right-sided colon cancer. Comparability between groups (if yes to all, two stars; if one of these characteristics was not reported, one star; if the two groups differed, no stars): 4, age, sex, body mass index, and American Society of Anesthesiologists score; and 5, tumor site, tumor size, and tumor stage. Outcome assessment: 6, more than six outcomes of interested clearly recorded: one star; and 7, quality of follow-up (one star if >90 of patients were followed up for 5 years).
Conversion rate
In total, 34 cases were converted to open surgery; in other words, the conversion rate was 7.2%. The conversion rate ranged from 0% to 21.4% in other studies (Table 1). Reasons for conversion to open surgery included tumor invasion to adjacent structures,11,14,18,21 bulky tumors,17,20 extensive adhesions,10,11,14,16–18,20,21 obscure bleeding, 20 cecum injury, 21 and hypercapnia. 21 The most common reasons were extensive adhesions (15 cases) and tumor invasion to adjacent structures (8 cases).
Operative time
Six clinical studies11,15–18,20 showed data on operative time. The heterogeneity test showed heterogeneity in the operative time of the six clinical studies; therefore, the random-effect model was used to combine the data. This model showed a significant difference between LRH and ORH in operative time. In the pooled data, the operative time for LRH was longer than that for ORH (WMD, 33.37; 95% CI, 14.23–52.51; P<.05) (Fig. 2).

Operation time (in minutes). CI, confidence interval; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; SD, standard deviation; WMD, weighted mean difference.
Blood loss
Four studies11,13,15,17 showed data on intraoperative blood loss, and in three studies, estimated intraoperative blood loss was significantly less for LRH than for ORH. The random-effect model was used to combine the data because of evident heterogeneity. In the pooled data, the intraoperative blood loss for LRH was less than that for ORH (WMD, −128.97; 95% CI, −232.01 to −25.94; P<.05) (Fig. 3).
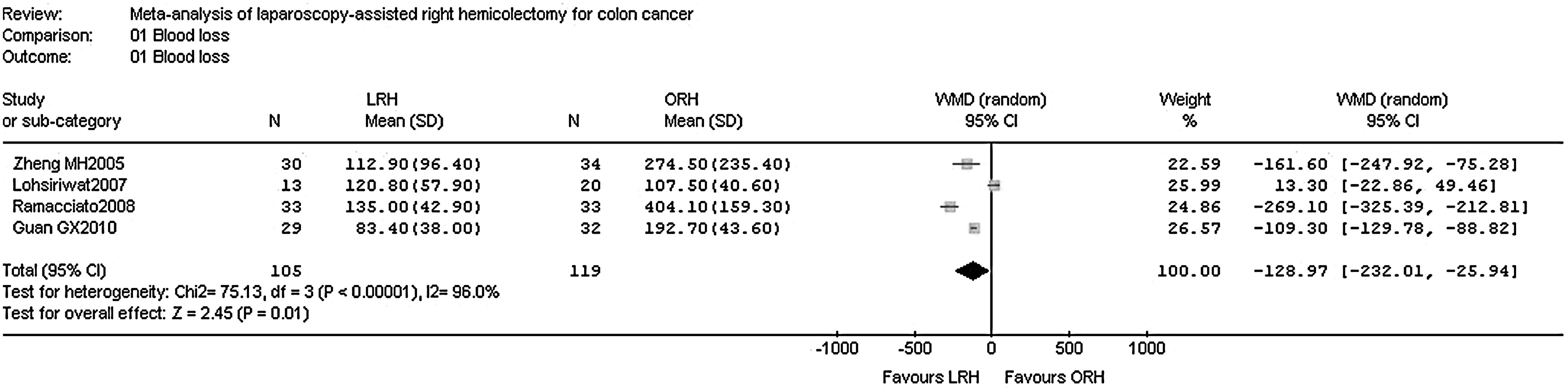
Blood loss (in mL). CI, confidence interval; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; SD, standard deviation; WMD, weighted mean difference.
Number of harvested lymph nodes
Seven clinical studies10,11,13,15–18 had data on the number of harvested lymph nodes and showed no significant difference between LRH and ORH. The random-effect model was used to combine the data because of evident heterogeneity. Analysis of the pooled data revealed no significant difference in the number of harvested lymph nodes between LRH and ORH (WMD, 0.51; 95% CI, −1.96 to 2.97; P=.69) (Fig. 4).

Harvested lymph nodes (number). CI, confidence interval; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; SD, standard deviation; WMD, weighted mean difference.
Postoperative pain
Because the presentation of data was heterogeneous with lack of a standardized protocol for analgesia, a meta-analysis was not appropriate. Of the included studies, five10,15,17,18,20 reported less postoperative pain after LRH than after ORH, and three of them10,17,18 showed that the difference was significant.
Time to first flatus
Four studies11,15–17 demonstrated the time to first flatus, and three of them11,16,17 showed a significantly shorter time in LRH than in ORH. The fixed-effect model was used to combine the data because heterogeneity was not evident. In the pooled data, the time to first flatus in LRH was significantly earlier than in ORH (WMD, −0.96; 95% CI, −1.25 to −0.66; P<.05) (Fig. 5).
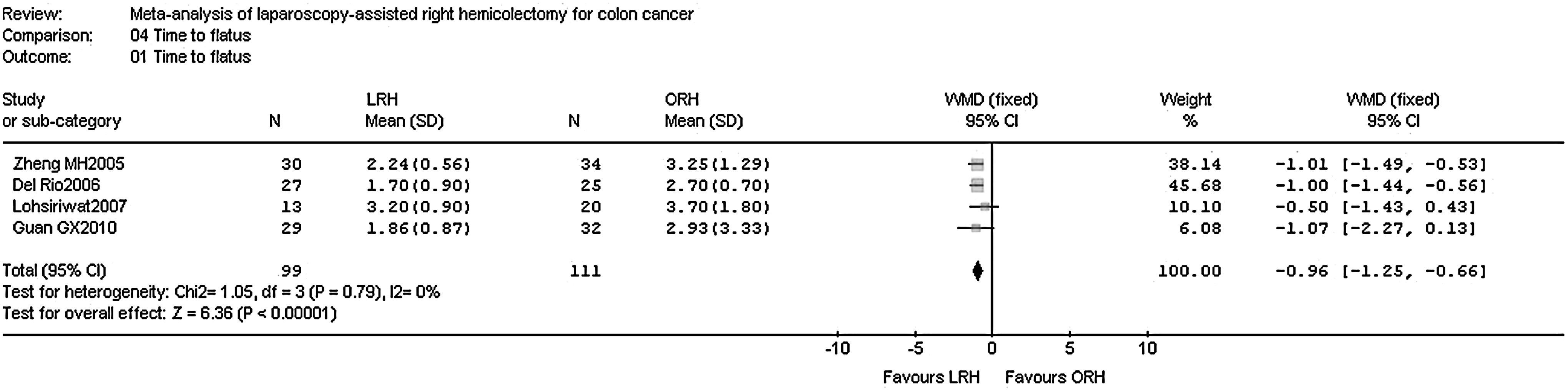
Time to flatus (in days). CI, confidence interval; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; SD, standard deviation; WMD, weighted mean difference.
Postoperative period of hospital stay
Five studies11,15–18 showed data on the postoperative period of hospital stay. In two11,17 of the five studies, length of stay was significantly shorter after LRH than after ORH. The random-effect model was used to combine the data because of evident heterogeneity. In the pooled data, the length of hospital stay after LRH was significantly shorter than after ORH (WMD, −1.62; 95% CI, −2.98 to −0.26; P<.05) (Fig. 6).
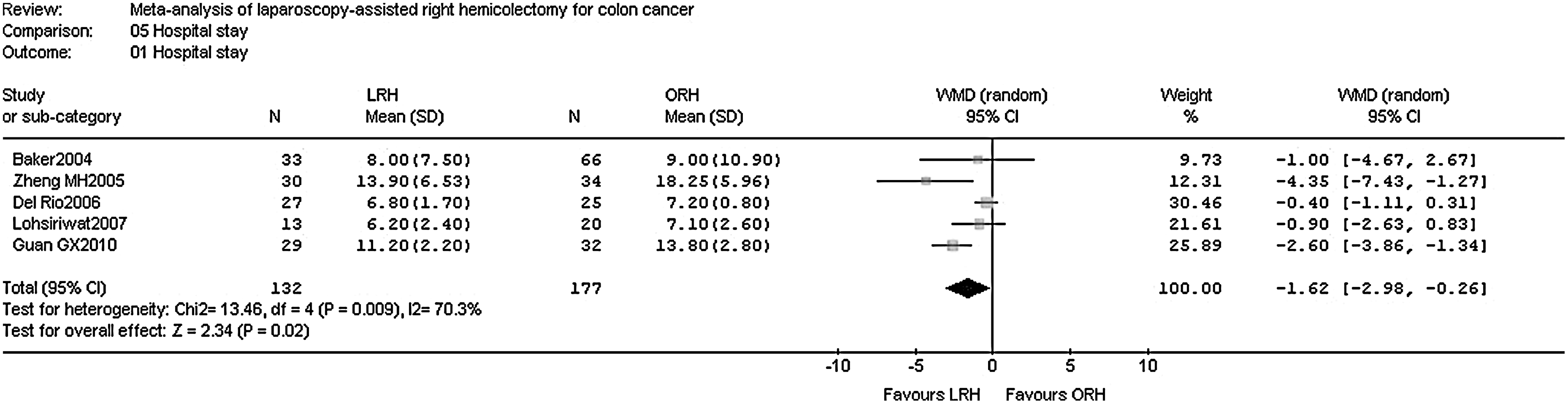
Hospital stay (in days). CI, confidence interval; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; SD, standard deviation; WMD, weighted mean difference.
Number of complications
Data on postoperative complications, including pneumonia, urinary tract infection, wound infection, anastomotic leak, ileus, hemorrhage, and deep vein thrombus, were collected and analyzed. The fixed-effect model was used to combine the data because heterogeneity was not evident. The laparoscopic and open surgery groups had similar incidences of pneumonia (OR, 1.02; 95% CI, 0.50–2.08; P>.05), urinary tract infection (OR, 0.78; 95% CI, 0.25–2.44; P>.05), anastomotic leak (OR, 0.82; 95% CI, 0.33–2.04; P>.05), ileus (OR, 0.63; 95% CI, 0.35–1.14; P>.05), hemorrhage (OR, 0.72; 95% CI, 0.21–2.49; P>.05), and deep vein thrombus (OR, 0.72; 95% CI, 0.18–2.97; P>.05), whereas the rate of wound infection was significantly less in the LRH group than in the ORH group (OR, 0.56; 95% CI, 0.31–1.01; P=.05). A summary of the pooled results for postoperative complications is presented in Table 3.
χ2, chi-squared; CI, confidence interval; df, degrees of freedom; I2, i-squared test of heterogeneity; LRH, laparoscopic right hemicolectomy; OR, odds ratio; ORH, open right hemicolectomy.
Mortality rate
Six studies10,14,18–21 had data on mortality rate and showed no significant difference between LRH and ORH. The fixed-effect model was used to combine the data because heterogeneity was not evident. In the pooled data, there were no significant differences in the mortality rate between LRH and ORH (OR, 1.00; 95% CI, 0.38–2.58; P=.99) (Table 3).
Recurrence rate
Five studies14,17–20 had data on recurrence rate. In two18,20 of these five studies, the recurrence rate was significantly less after LRH than after ORH. The fixed-effect model was used to combine the data because heterogeneity was not evident. In the pooled data, there were no significant differences in recurrence rate between LRH and ORH (OR, 0.83, 95% CI, 0.51–1.34; P=.45) (Fig. 7). Details of recurrence sites are shown in Table 4.
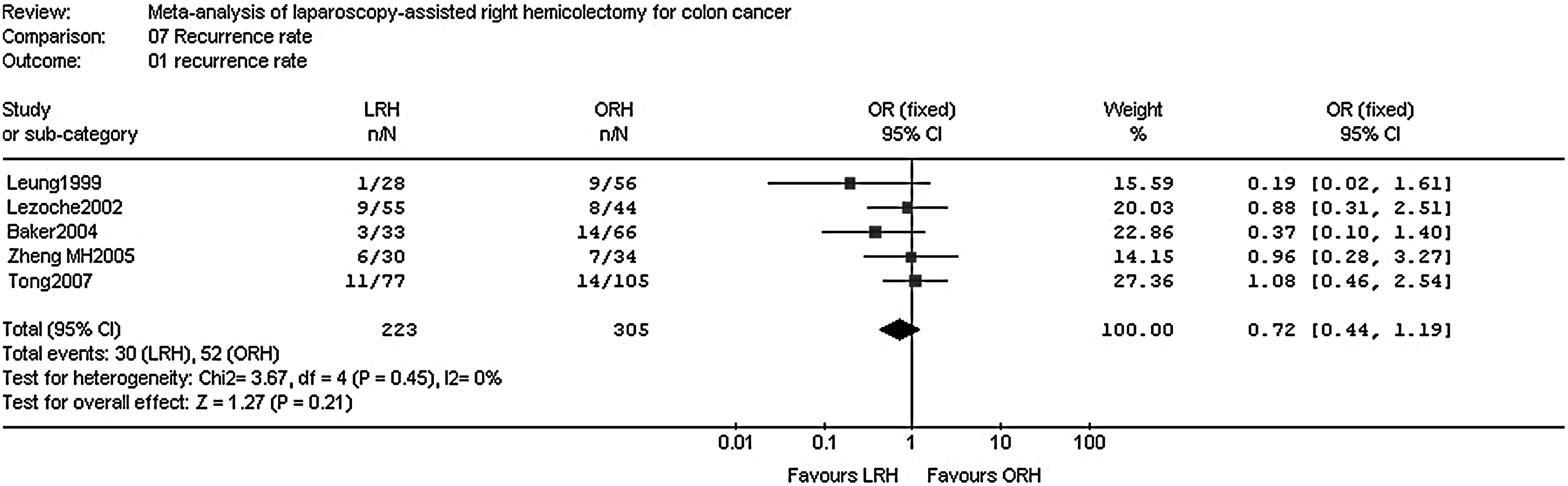
Recurrence rate. CI, confidence interval; LRH, laparoscopic right hemicolectomy; OR, odds ratio; ORH, open right hemicolectomy; SD, standard deviation.
HM, hepatic metastases; LM, lung metastases; LRH, laparoscopic right hemicolectomy; ORH, open right hemicolectomy; PM, peritoneal metastases; SLNM, supraclavicular lymph node metastases; UN, unspecified.
Assessment of publication bias
The funnel plot of standard of error by effect size for the measurements of wound infection and ileus showed an equal distribution of studies around the middle line, indicating that publication bias was not evident (Fig. 8).
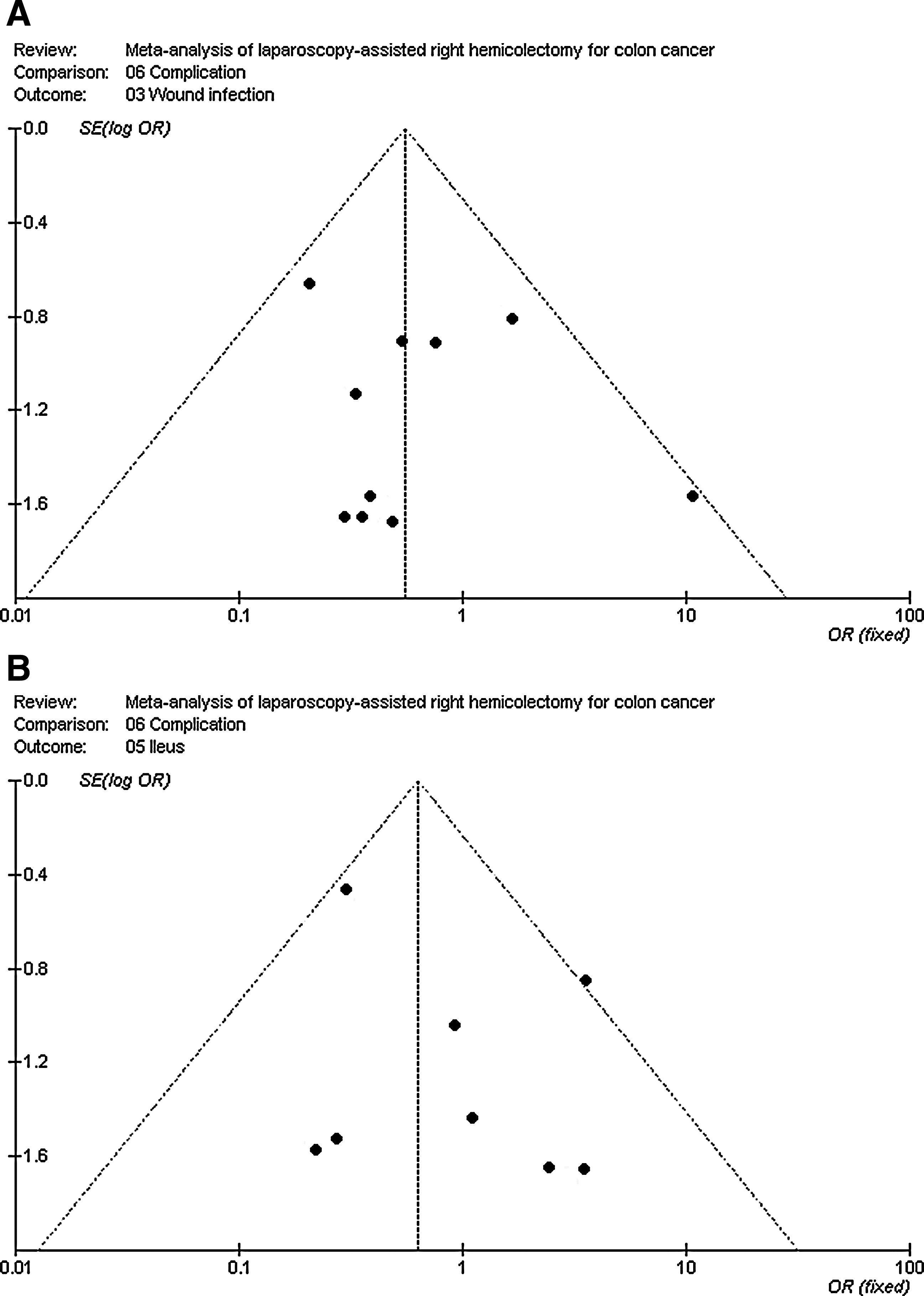
Funnel plot for the results from all studies comparing
Sensitivity analysis
Sensitivity analyses address robustness of the outcomes obtained from meta-analysis. The sensitivity analysis included the following: (1) studies published after 2006 and (2) studies with ≥25 cases per group. Outcomes that could not be analyzed because of insufficient data (fewer than two studies) were excluded from analysis. Six outcomes were selected for sensitivity analysis, and the results are listed in Table 5. Through sensitivity analysis, the OR or WMD and the level of significance for the six outcomes, including operative time, number of harvested lymph nodes, time to first flatus, pneumonia, wound infection, and anastomotic leakage, were not evidently changed.
CI, confidence interval; OR, odds ratio; WMD, weighted mean difference.
Discussion
LRH has aroused interest among many surgeons since its inception, and it has gradually become one of the most widely used surgical procedures in the treatment of colon cancer.3,22 However, compared with open surgery, it is not clear whether laparoscopic surgery is able to achieve adequate lymphadenectomy, whether it increases the number of complications, and whether it can achieve a good prognosis. This meta-analysis collected 12 clinical studies that compared LRH versus ORH for the first time to investigate the value and safety of LRH in the treatment of colon cancer. The heterogeneity of different tumor sites and different surgical procedures was overcome to better combine the data. Meanwhile, seven common complications, rather than only a few complications or the overall complication rate, were selected for analysis in this meta-analysis for a better evaluation of the safety of LRH.
In total, 12 studies involved 34 cases of conversion to open surgery; the conversion rate was 7.2% and ranged from 0% to 21.4% in other studies. The most common reasons were extensive adhesions (15 cases) and tumor invasion to adjacent structures (8 cases). The total conversion rate in this review was slightly higher than that reported by Abraham et al. 5 in 2004 [5], but lower than that reported by Abraham et al. 23 in 2007. The authors believed that a difference in proficiency with laparoscopic technique and a difference in the patient's condition led to the wide range of conversion rate. Bokey et al. 21 reported a high conversion rate and long hospital stay in their laparoscopic patients, and Tong and Law 14 reported a high rate of wound infection and ileus. Conversion of a laparoscopic procedure is associated with increased morbidity rates compared with planned open procedures. Careful preoperative patient selection is therefore of utmost importance. 24
This meta-analysis of six clinical studies revealed that the operative time for LRH was longer than that for ORH. There is a steep learning curve to achieve advanced laparoscopic skills, and specialized equipment is required, 7 which requires an accumulation of cases, the surgeon's familiarity with the endoscopic instruments, and cooperation of the whole therapeutic team. With increased experience, the mean operative time for LRH would decrease significantly. Lezoche et al. 19 reported that the mean operative time for the last 20 patients was shortened by about 70 minutes compared with the first 30 patients.
Our meta-analysis revealed significantly less blood loss during LRH than during ORH. No selected studies explained reasons for the low blood loss, whereas in a meta-analysis of laparoscopic-assisted distal gastrectomy, Ohtani et al. 25 considered that this was attributed to the enlarged laparoscopic surgical field, which could better expose and allow for identification of the vessels. We believe that the use of special equipment, including the ultrasonic scalpel, and LigaSure™ (Covidien, Mansfield, MA), also contributed to this outcome. The incidence of recurrence was significantly higher in patients who received transfusions during surgery 26 with the exception of autologous transfusion. 27 Therefore, a reduction in the amount of bleeding in patients with colon cancer is desirable because it can reduce the likelihood or amount of transfusion.
Oncological clearance of laparoscopic surgery has always been a controversial issue. Our meta-analysis revealed no evident difference in the number of lymph nodes dissected between LRH and ORH, which is in accordance with previous meta-analyses.4–6 Therefore, LRH could achieve the same level of successful lymphadenectomy as with ORH; suspicion of the effectiveness of lymph node dissection by LRH was unfounded. We noted that two studies from the United Kingdom showed that the number of harvested lymph nodes was significantly increased in the late than in the earlier stages,10,18 which might relate to the surgeon's improvement of laparoscopic technique.
Our meta-analysis revealed that the time to first flatus and postoperative period of hospital stay were both shorter for LRH than for ORH. Time to oral intake as a measure of recovery of gastrointestinal function is prone to bias because surgeons with an interest in laparoscopic surgery are likely to feed their patients earlier than those who perform open surgery. 28 Although time to flatus is an objective indicator, it indicated that LRH was more conducive to recovery of gastrointestinal function. Kang et al. 29 considered that recovery was faster because the laparoscopic procedure allowed for a more subtle operative technique and reduced the level of invasion. In addition to this, Braga et al. 30 found that gut oxygen tension was significantly higher in the laparoscopic group than in the open group during the entire surgical procedure. Many factors could explain this, such as the less traumatic abdominal incision, less traction on the mesentery, and the relatively low-pressure pneumoperitoneum that was used. It can be speculated that the higher oxygen tension during laparoscopic surgery plays an important role in improving the systemic host response and early recovery of gut function. Five studies reported less postoperative pain after LRH than after ORH, which might have been secondary to the decreased invasiveness of laparoscopic surgery.
To fully assess the safety of LRH, seven frequent complications were selected and analyzed in this meta-analysis. The rate of wound infection was significantly less in LRH than in ORH, whereas differences in other complications, including pneumonia, urinary tract infection, anastomotic leak, ileus, hemorrhage and deep vein thrombus, were not evident. In total, eight studies reported a lower wound infection rate in LRH than in ORH. Nakamura et al. 12 reported that the wound infection rate in LRH was 3%, far below that of 13% in ORH. Our meta-analysis revealed no significant difference in mortality; thus, we can conclude that LRH is safe and feasible and even has the advantage of reducing the incidence of wound infection. Perhaps the faster recovery of gastrointestinal function and the lower number of postoperative complications led to the shorter period of hospitalization.
Our meta-analysis revealed that there was no significant difference in recurrence rate between the two groups. In other words, LRH achieved a short-term prognosis equivalent to that of ORH. The long-term prognosis could not be evaluated because the 5-year survival rate was provided in only one 20 of the studies analyzed.
We have identified some limitations of this meta-analysis. First, the included studies covered both right and extended right hemicolectomy, which may have caused heterogeneity in the results. Second, although the surgical technique was described in all included studies, there were no data to detail the minimally invasive surgical experience of the surgeons, which may affect the outcomes in which we were interested. Third, due to the inclusion of nonrandomized studies, there is an inherent selection bias in the two groups. Finally, there is the limitation of non-publication and selective reporting bias, which cannot be accounted for.
In conclusion, LRH is a safe technical alternative to ORH for patients with colon cancer. It involves minimal invasion, faster postoperative recovery, and a lower rate of wound infection, and it can achieve the same degree of radicality and short-term prognosis as ORH. The drawback is that the operative time is slightly longer, which requires improved technical ability of the surgeon and further improvement of laparoscopic instruments. Most of the studies included in our meta-analysis were retrospective studies, which could have led to some selection bias. Therefore, more well-designed, multicenter, prospective randomized controlled trials are expected to be published to allow for a more convincing evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist. J.D. and Y.X. acquired, analyzed, and interpreted data and drafted the article. G.-Q.L. selected the topic and study design and gave final approval of the version to be published. Z.-M.Z. and S.L. acquired, analyzed, and interpreted data. Z.-S.Y. revised the article.