
Abstract
Abstract
Background:
Management of staghorn renal stones is still challenging. We present our experience with laparoscopic anatrophic nephrolithotomy as an alternative option for management of staghorn renal calculi.
Patients and Methods:
Twenty-four patients with staghorn renal calculi underwent 25 laparoscopic anatrophic nephrolithtomy procedures. Characteristics of patients and stones along with perioperative features such as operation time, transfusion, ischemic time, hospitalization, stone-free rate, and biochemical data were recorded prospectively. We applied the one-layer knotless technique for renorrhaphy repair.
Results:
The mean age of the patients was 55.1±10.9 years (range, 28–74 years). Eleven (44%) operations were done on the right side, and 14 (56%) were done on the left side. Complete and partial staghorn stones existed in 17 (68%) and 8 (32%) renal units, respectively. The mean stone size was 61.5±11.5 mm. Ischemic time was 30.4±7.55 minutes. The stone-free rate was 88% on discharge and 92% after one session of extracorporeal shockwave lithotripsy.
Conclusions:
Although percutaneous nephrolithotomy is the standard of care for treatment of staghorn stone, laparoscopic anatrophic nephrolithotomy seems to be a safe and feasible option in select patients.
Introduction
Laparoscopy has been used to duplicate various techniques of open surgery used for renal and ureteral stone management.5–7 We previously reported our experience with laparoscopic anatrophic nephrolithotomy (LAN) in a preliminary series. 8 Our results showed that the procedure was safe, feasible, and successful. Here, we present our complementary series on LAN to more precisely assess feasibility and safety of the procedure as an alternative for treatment of staghorn renal stones. To our knowledge, this is the largest series on LAN.
Subjects and Methods
Twenty-four patients with a staghorn renal stone who underwent LAN between 2008 and 2010 were included in this prospective study. The ethics committee approved the study, and written consent was obtained from all patients. Patients with large staghorn stones composed of one piece and maximally three or four pieces, without considerable hydronephrosis or an extrarenal pelvis, were selected for LAN. Patients with small stones, multiple stone pieces, pyuria/bacteriuria in urine analysis, or positive urine culture were not selected. Patients with a solitary kidney or history of previous ipsilateral open renal surgery were also excluded. Before surgery, patients underwent a complete radiological evaluation, including abdominopelvic ultrasonography (US) and intravenous urography (IVU). Although computed tomography scan was performed for some of the patients, it was not available for all. All of the patients were admitted on the day before surgery and underwent renal function tests, a complete blood count, urine analysis, and culture. Characteristics of patients and stones were recorded. Stone size was measured as the largest diameter on US or IVU. Stones occupying pelvis and all calyces were considered as a complete staghorn.
LAN was performed according to the technique described previously. 8 A four-port transperitoneal approach was used. After medial mobilization of the colon, the renal pedicle was completely dissected, Gerota's fascia was opened, and the kidney was fully mobilized within the fascia. The renal artery was clamped by a bulldog clamp (Aesculap, Tuttlingen, Germany). Brodel's line and collecting system were sharply incised, and the staghorn stone was removed. Both the collecting system and renal cortex were closed in one layer with one row of running sutures; sutures were buttressed by applying Hem-o-lok clips (Weck® Closure Systems, Teleflex, Inc., Research Triangle Park, NC) instead of tying knots. Intraoperative and postoperative variables such as operation time, transfusion, ischemic time, hospitalization, stone-free rate, and biochemical characteristics were also recorded. Abdominopelvic US and plain films were obtained before discharge. Three months postoperatively, IVU and a repeated US were performed. Patients with no residual stone greater than 4 mm were considered stone free.
Results
Twenty-four patients (7 females and 17 males) underwent 25 laparoscopic operations; 1 patient was operated on bilaterally in two sessions. The mean age of the patients was 55.1±10.9 years (range, 28–74 years). Eleven operations (44%) were done on the right side, and 14 (56%) were done on the left side. Complete and partial staghorn stones existed in 17 (68%) and 8 (32%) renal units, respectively. Table 1 shows intraoperative and perioperative features. A ureteral stent was inserted only in 3 (12%) patients intraoperatively.
DJ, double-J stent; SD, standard deviation.
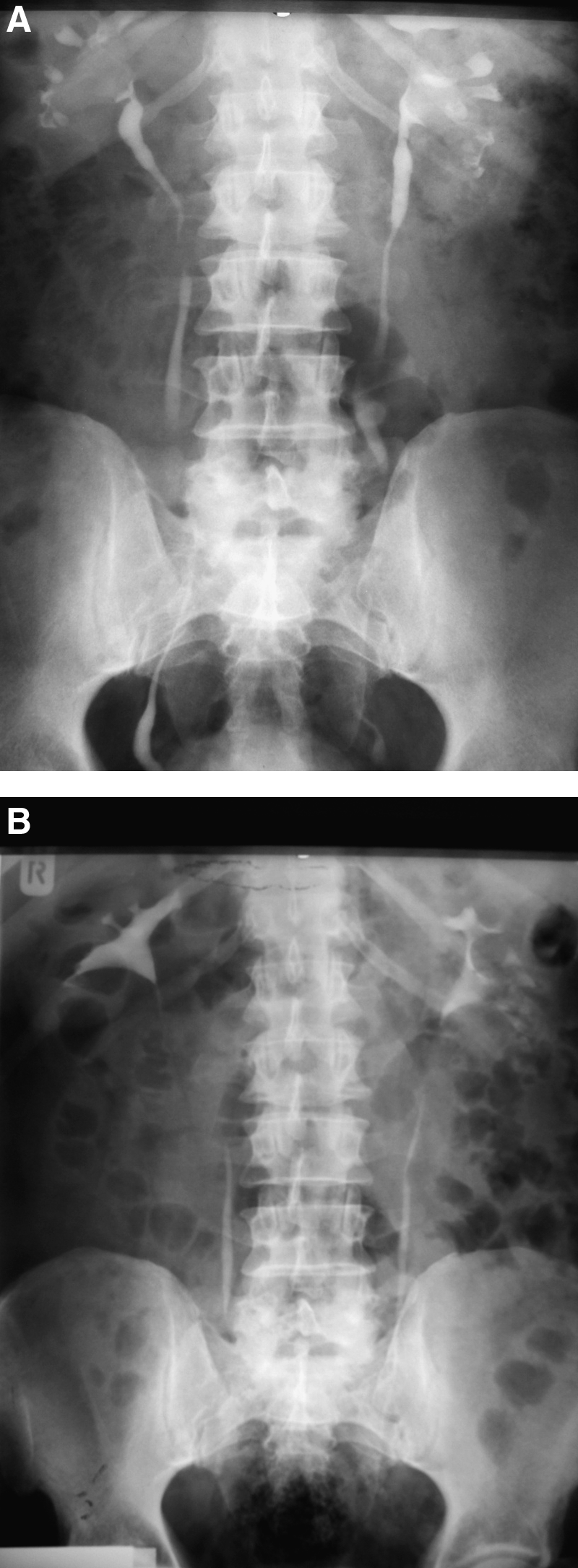
Collection, fever, and urinary leak were encountered in 2 (8%), 3 (12%), and 2 (8%) patients, respectively. According to the Clavien–Dindo classification of surgical complications, 9 3 of 7 patients with collection, fever, and/or urinary leak had Grade II complication (i.e., resolved with medical and antibiotic therapy), and 4 patients had Grade IIIa complication (i.e., resolved with stenting). Nephrectomy (Grade IIIb complication) occurred in 1 patient (4%). The stone-free rate was 88% on discharge and 92% after one session of shock wave lithotripsy. The mean preoperative hemoglobin, hematocrit, and serum creatinine levels were 14.4±1.6 g/dL, 43.1±4.4%, and 1.20±0.36 mg/dL, respectively. Postoperative hemoglobin, hematocrit, and creatinine levels were 12.95±1.74 g/dL, 40.2±5.6%, and 1.31±0.44 mg/dL on discharge day, respectively. Post- and preoperative biochemical values were not different significantly. Figure 1 shows preoperative and postoperative IVU of the patient who underwent LAN on both sides in two sessions.
Discussion
Although laparoscopy is used in several urologic procedures with similar efficacy and less morbidity, its role in renal stone management is not well defined yet.2–4 Laparoscopic duplication of the open stone surgery technique may be a solution to achieve a high stone-free rate of the open surgery and also decrease its morbidities. Using laparoscopy for urolithiasis surgical management was first suggested by Wickham 10 in 1979. Later, in 1985, Eshghi et al. 11 reported on a case of laparoscopic stone removal from a pelvic kidney. Since then several reports on laparoscopic renal stone removal have been reported in various situations. Laparoscopy has been used for stone removal in calyceal diverticulum, ectopic kidney, horseshoe kidney, and several routine indications.5,6,12 Many investigators have reported that laparoscopy is a safe approach for renal stone management with successful results and minimal morbidity.5–8,12 Meria et al. 13 compared laparoscopic pyelolithotomy versus PNL for pelvic stones larger than 20 mm. The stone-free rate was insignificantly better in the laparoscopy group, and complications were almost similar. They described that laparoscopy could be an alternative to PNL for large pelvic stones.
Management of staghorn renal stones is still a challenging issue in urology. Because of the high recurrence of staghorn renal stones and their high potential for infection, renal function impairment, and even threatening general health, the importance of complete stone clearance cannot be overemphasized. 14 Many investigators reserve open stone surgery as the preferred route for managing large staghorn stones to minimize the need for secondary interventions after complete stone removal.15,16 Deger et al. 17 were the first to report LAN in a patient. We reported our initial experience on LAN in 5 patients with acceptable outcome. 8 Here, we report LAN in 24 patients with a stone-free rate of 88% on discharge and 92% after one session of shock wave lithotripsy.
We applied the one-layer knotless continuous renorrhaphy technique to close the nephrotomy in LAN. We have used this technique both for LAN and for laparoscopic partial nephrectomy (LPN) previously.8,18 Using Hem-o-lok clips instead of knot tying and closing the collecting system and cortex in one layer could simplify the technique and shorten the warm ischemia time. Several authors have reported safety and efficacy of using clips to save time during nephrotomy closure after LPN.19–21 Closing the collecting system and cortex in one layer has been applied by Weight et al. 22 after LPN and shown to be safe and effective. Because the repair technique provided a watertight closure, we used a ureteral stent only in 3 (12%) operations. Nevertheless, urine leakage or collection was encountered in only 4 patients. Collection was diagnosed by postoperative US performed before discharge. This was based on our previous experience with LAN and LPN.8,18 One of our patients underwent nephrectomy 3 weeks after LAN. He had had several episodes of pyelonephritis in his history and showed 30% differential function in the technicium-99m diethylenetriamine pentaacetic acid scan. We think he was not a suitable candidate for LAN. Postoperatively, prolonged fever and collection resistant to conservative treatment necessitated nephrectomy. However, nephrectomy has also been encountered after PNL for staghorn stones.23,24 We did not find a significant change of creatinine level postoperatively; however, using creatinine as an indicator of renal function instead of split renal function assessed by renal scan is a limitation of our study. Transperitoneal exposure to infected urine is a concern in LAN. This event may also happen in other laparoscopic stone surgeries such as laparoscopic ureterolithotomy and pyelolithotomy. We tried to decrease the probability of the exposure of infection by excluding patients with pyuria/bacteriuria in urine analysis or positive urine culture from the study. Moreover, laparoscopy allows irrigation of the exposed space and suction of the possibly infected fluid. This might be why long-term fever, abscess, or peritonitis was not reported in previous reports of laparoscopic stone surgeries.6,7 However, infected urine may be exposed to extrarenal space, but of course not to peritoneal but to retroperitoneal space, during PNL. Warm ischemia time is another concern about LAN and currently considered as a disadvantage compared with PNL. Warm ischemia time longer than 35 minutes happened in only 1 patient in our series. However, the LAN technique is at its primary steps and could be improved gradually. Using new techniques for maintaining cold ischemia such as intrarenal and perirenal irrigation with cold saline or using an ice slurry in perirenal space could solve this problem in the future. 25
Table 2 shows findings of some studies on PNL for staghorn renal stones along with the current study.26–29 Hospitalization time in our study is almost similar to PNL studies. It is because several patients in our series came from faraway cities and could not return easily for early follow-up; hence, we had to hospitalize them for a longer period. Some complications such as angioembolization and hydro-/hemothorax are exclusively encountered in PNL but not in LAN. The transfusion rate in our study has been more than in some PNL studies and less than in the study of Singla et al. 28 It is noticeable that we applied transfusion for patients with a 2 g/dL decrease of hemoglobin level and did not delay it until hypotension occurred. That is, some of the transfused patients could be managed without transfusion. It is obvious from the study by Desai et al. 27 that increased experience with PNL for staghorn stone improves the outcome of the procedure; this could also be expected to occur in LAN. Renal function status may be a concern following LAN and open stone surgery, as it is also in PNL. Comparing renal function after PNL and open stone surgery, Al-Kohlany et al. 30 reported that function is preserved or improved in 86.7% and 91% of patients in open surgery and PNL, respectively. Hence, it could be expected that LAN might not negatively affect renal function more than other minimally invasive approaches do.
Both rows are related to one study; the first row shows later cases, and the second row shows earlier ones.
NA, not applicable.
Although PNL is the standard of care for treatment of a staghorn stone, laparoscopy could be an acceptable alternative option for renal stone management in select patients with an acceptable stone-free rate and complications. In brief, patients with one-piece large staghorn stones, particularly when they are not appropriate candidates for PNL, could be considered for LAN. It should be noted that LAN is an advanced laparoscopic procedure and should be performed by expert laparoscopists. However, more comparative studies are needed to define laparoscopy role more precisely.
Footnotes
Disclosure Statement
No competing financial interests exist.