
Abstract
Abstract
Background:
Scarless and minimally invasive surgery is becoming popular in the head and neck area. We have developed a new robotic selective neck dissection procedure for head and neck squamous cell carcinoma (HNSCC) to avoid a long visible lateral neck scar. Here we report on the technical feasibility and safety of our procedure.
Subjects and Methods:
We prospectively analyzed 4 patients with early HNSCC who underwent transoral robotic surgery (TORS) and concomitant robotic selective neck dissection via a gasless postauricular facelift approach using the da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA).
Results:
Of these patients, 3 were male, and 1 was female. The mean age was 59.0±8.8 years. All patients had tongue cancer, with a clinically negative neck. Three patients were T1, and 1 patient was T2. All patients underwent partial glossectomy by TORS and elective robotic selective neck dissection including levels I, II, and III. The robotic selective neck dissection procedure was completed successfully in all patients. The mean operative time was 276±48 minutes. The mean number of lymph nodes removed was 19.3±7.3. Postoperative hematoma and transient marginal nerve palsy occurred in 1 patient each. Cosmetic satisfaction was excellent in all patients.
Conclusions:
Preliminary results indicate that robotic selective neck dissection via a gasless postauricular facelift approach is feasible and safe and allows for excellent postoperative cosmesis. Further studies are necessary to determine the oncologic safety and surgical completeness of this procedure compared with conventional neck dissection.
Introduction
We have developed a technique of robotic selective neck dissection via a gasless postauricular facelift approach using the da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) for the management of cervical lymph node metastasis in early head and neck cancer in a way that avoids a long visible scar in the neck. In this study we report on the technical feasibility and safety of this novel procedure based on our early experience.
Subjects and Methods
Patients
This prospective study was carried out on 4 consecutive patients with head and neck squamous cell carcinoma (HNSCC) who underwent transoral robotic surgery (TORS) and robotic selective neck dissection via a gasless postauricular facelift approach using the da Vinci Surgical System from October 2011 to January 2012. The individuals who we classified as eligible for robotic selective neck dissection were early HNSCC patients with imaging results with clinically negative necks, on whom transoral resection of the primary tumor and elective neck dissection were to be performed. We excluded patients with clinically positive cervical lymph nodes, recurrent tumors, or distant metastasis. We also excluded patients with a history of neck surgery or irradiation. Patients who required transcervical incision for removal of the primary tumor were also excluded.
All patients were diagnosed with squamous cell carcinoma of tongue and showed no evidence of cervical lymph node metastasis upon physical examination or in imaging studies such as computed tomography, magnetic resonance imaging, and positron emission tomography/computed tomography. Three patients were male, and 1 was female. The mean age was 59.0±8.8 years (range, 49–69 years). T classification was T1 in 3 patients and T2 in 1 patient. All patients underwent simultaneous transoral partial glossectomy by TORS and elective robotic selective neck dissection.
The patients studied were informed about the operative procedure, its advantages and disadvantages, and the possibility of conversion to open surgery. Written informed consent was obtained from each patient, and the study was approved by the Institutional Review Board of Hanyang University Hospital (Seoul, Korea).
Surgical procedure
In all cases, robotic selective neck dissection was followed by partial glossectomy using TORS. The patient was placed in the supine position under general anesthesia. The neck was extended slightly, and the head was turned to the side opposite the lesion. After the patient had been draped, a postauricular facelift incision was designed (Fig. 1). The skin incision was made in the postauricular sulcus, curved posteriorly at the upper third of the auricle, and continued along the occipital hairline. The skin flap was elevated in the plane of the subplatysmal level over the sternocleidomastoid (SCM) muscle by monopolar cautery dissection under direct vision. Elevation of the skin flap was continued anteriorly to the midline of the neck, inferiorly to the clavicle, superiorly to the lower border of the mandible, and posteriorly to the anterior border of the trapezius muscle (Fig. 2). The external jugular vein was then divided at the posterior border of the SCM muscle, the fascia overlying the SCM muscle was elevated, and the dissection of fibroadipose tissues was continued to expose the internal jugular vein medially and the parotid gland superiorly. The tail portion of the parotid gland was divided, and the posterior belly of the digastrics muscle was exposed. The great auricular nerve was generally preserved. After retraction of the digastrics muscle, the high level IIA lymph nodes were dissected under direct vision, and the spinal accessory nerve was identified where it entered the SCM muscle. After adequate retraction of the SCM muscle and digastrics muscle, level IIB lymph nodes were dissected under direct vision. After completion of the dissection of level IIB and high level IIA lymph nodes, an external retractor was inserted to maintain working space without CO2 gas insufflations, and it was suspended using a lift system. An 8-mm trocar was inserted through a small secondary incision in the lower neck area if necessary. The robotic arms were then docked. Three robotic arms were inserted through the postauricular facelift incision port; a dual-channel 30° endoscope was placed in the center of the port, and Harmonic® (Ethicon Endo-Surgery, Blue Ash, OH) curved shears and Maryland dissectors were placed on either side of the endoscope. A fourth robotic arm with Prograsp forceps (Intuitive Surgical) was inserted through the lower neck trocar if this was used (Fig. 3).

A postauricular facelift incision was made in the postauricular sulcus, curved posteriorly at the upper third of the auricle, and continued along the occipital hairline.

The skin flap was elevated in the plane of the subplatysmal level under direct vision anteriorly to the midline of neck, inferiorly to the clavicle, superiorly to the lower border of the mandible, and posteriorly to the anterior border of the trapezius muscle. An external retractor was used to maintain working space without CO2 gas insufflations, and an 8-mm trocar was used in the lower neck area for insertion of a fourth robotic arm with Prograsp forceps.
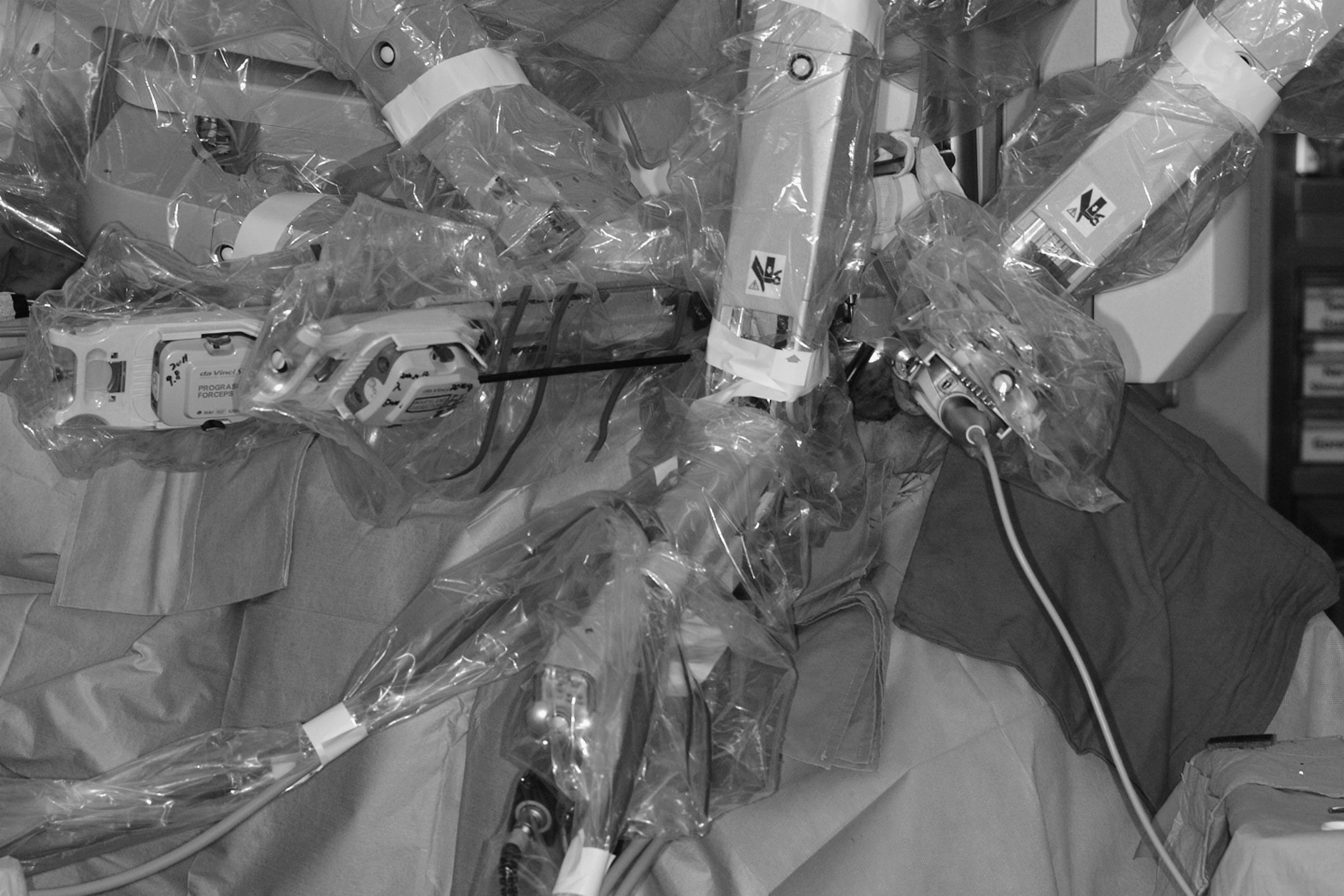
After working space was generated, four robotic arms were docked. Three robotic arms were placed through the postauricular facelift incision port; a dual-channel 30° endoscope was placed in the center of the port, and Harmonic curved shears and Maryland dissectors were placed on either side of the endoscope. A fourth robotic arm with Prograsp forceps was inserted through the lower neck trocar.
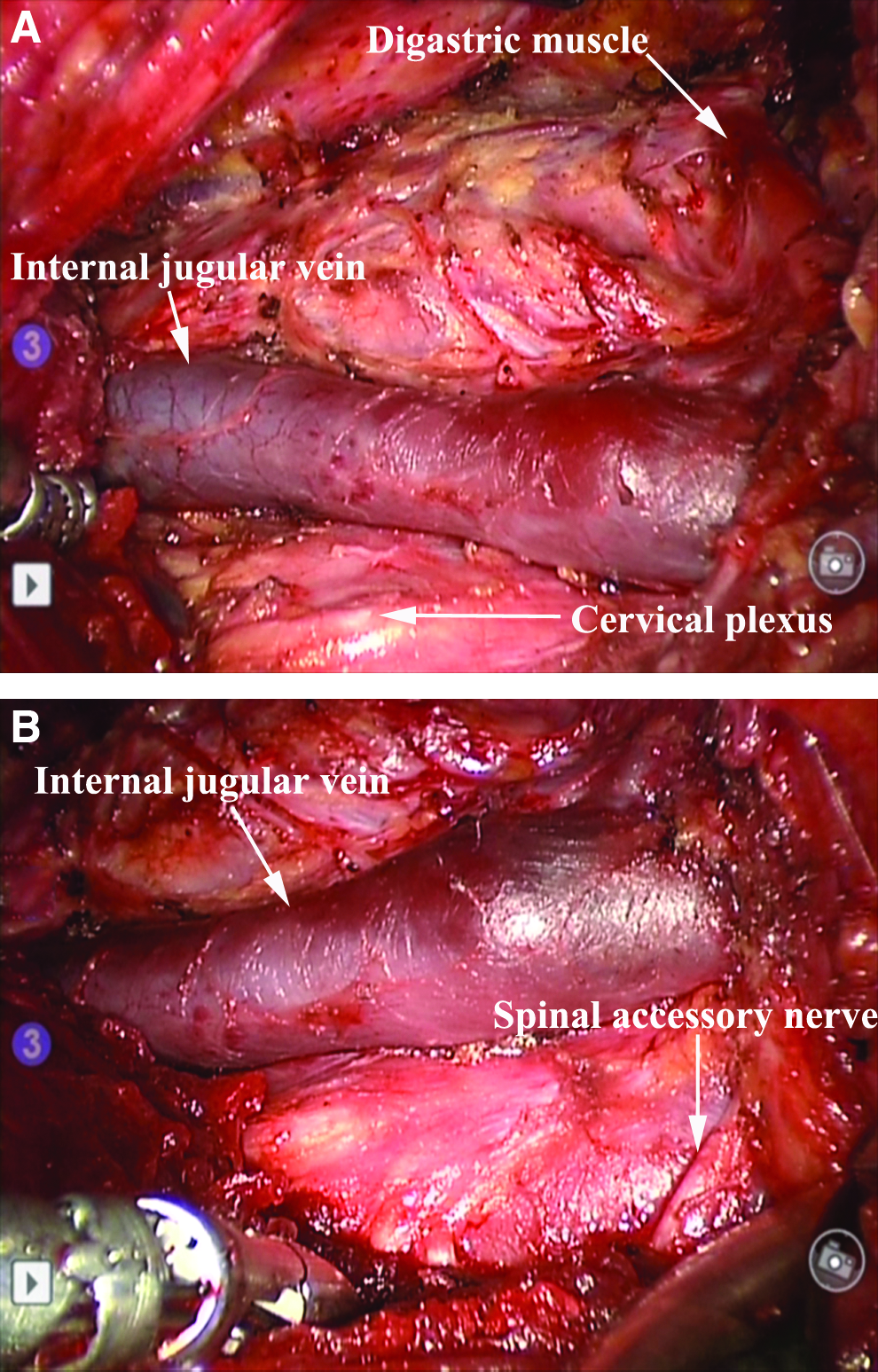
After docking of the robotic arms, robotic dissection using a console was started in level I. The prevascular and retrovascular lymph nodes were dissected, taking care not to injure the marginal branch of the facial nerve (Fig. 4). The facial artery and vein were identified and divided using a Harmonic curved shear. The submandibular gland and surrounding fat and lymph node tissues were dissected while preserving the hypoglossal nerve. The proximal portion of the facial artery was divided using a hemoclip (Fig. 5). After retraction of the mylohyoid muscle using Prograsp forceps, the lingual nerve and its tributary to the submandibular gland were identified and divided. Wharton's duct and accompanying blood vessels were divided using a Harmonic curved shear or hemoclip. The submental fibroadipose tissue and lymph nodes were then removed. After completing dissection of level I, dissection of level II lymph nodes was performed by continuing the previous dissection of level IIB and high level IIA. The internal jugular vein and carotid artery were unwrapped from surrounding fibroadipose tissue and lymph nodes, while preserving the spinal accessory nerve (Fig. 6). The dissection was progressed from level II to the omohyoid muscle inferiorly (level III). The cervical nerves were identified and preserved by maintaining the dissection lateral to them. As a fascia was incised over the internal jugular vein, the lymph nodes and fatty tissue were rolled anteriorly and removed from this overlying fascia. The selective neck dissection including levels I–III was completed (Fig. 7), and the resected specimen was removed through the incision port (Fig. 8). Negative suction was applied for drainage, and the wound was closed.
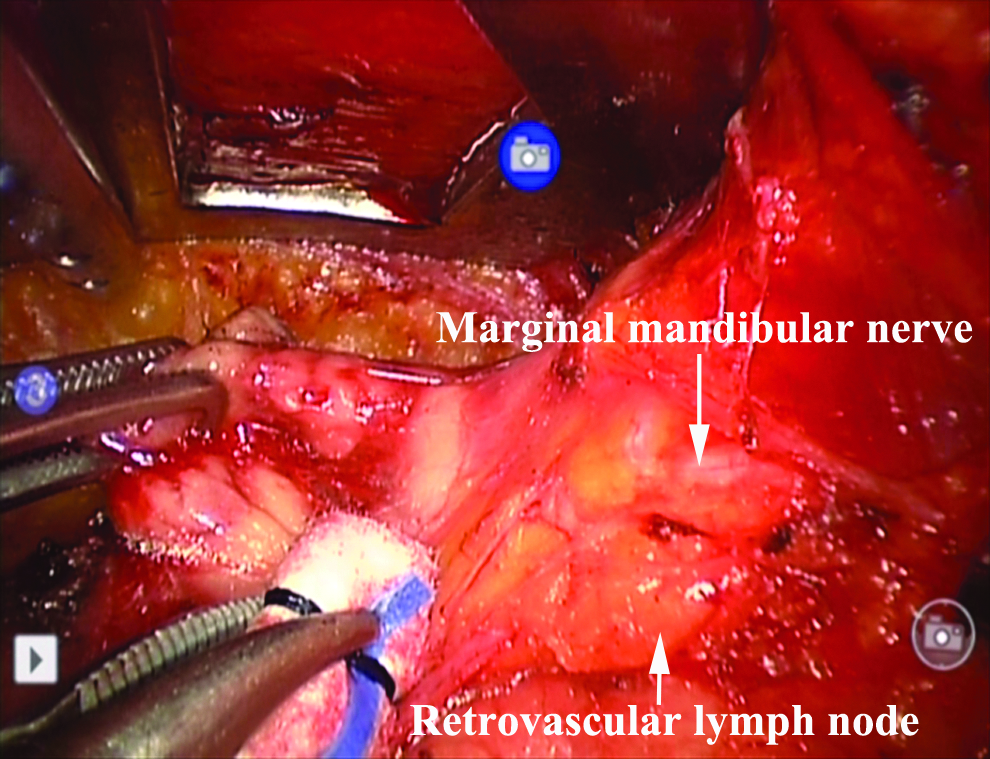
The prevascular and retrovascular lymph nodes were dissected, taking care not to injure the marginal branch of the facial nerve.
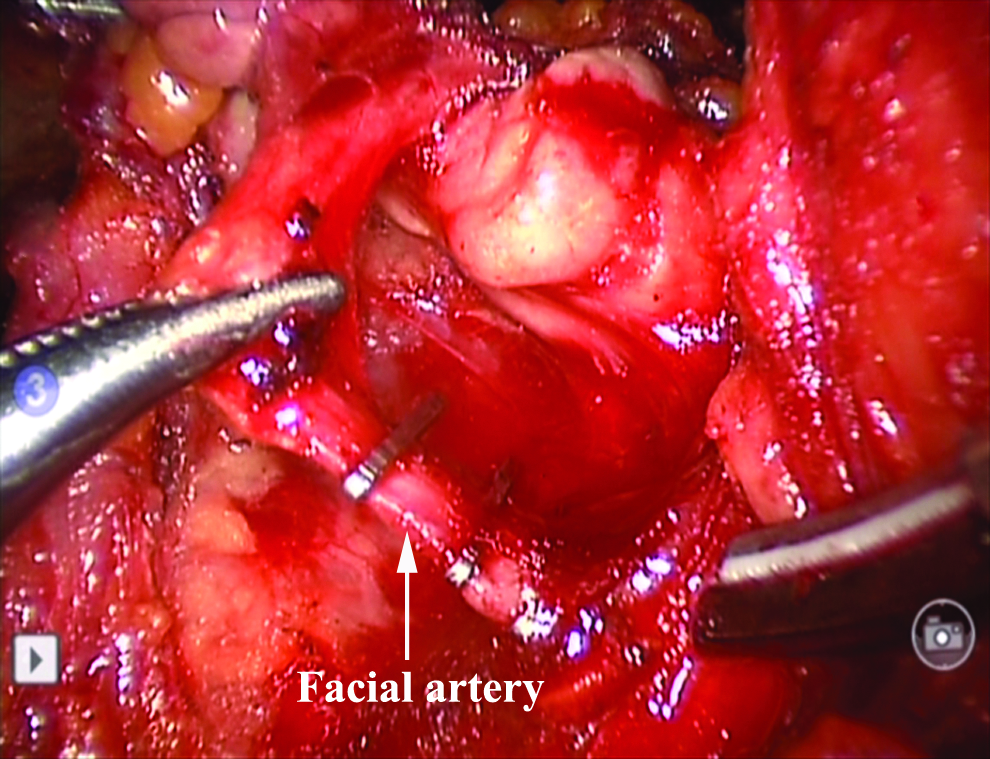
The proximal portion of the facial artery around the submandibular gland was divided using a hemoclip.
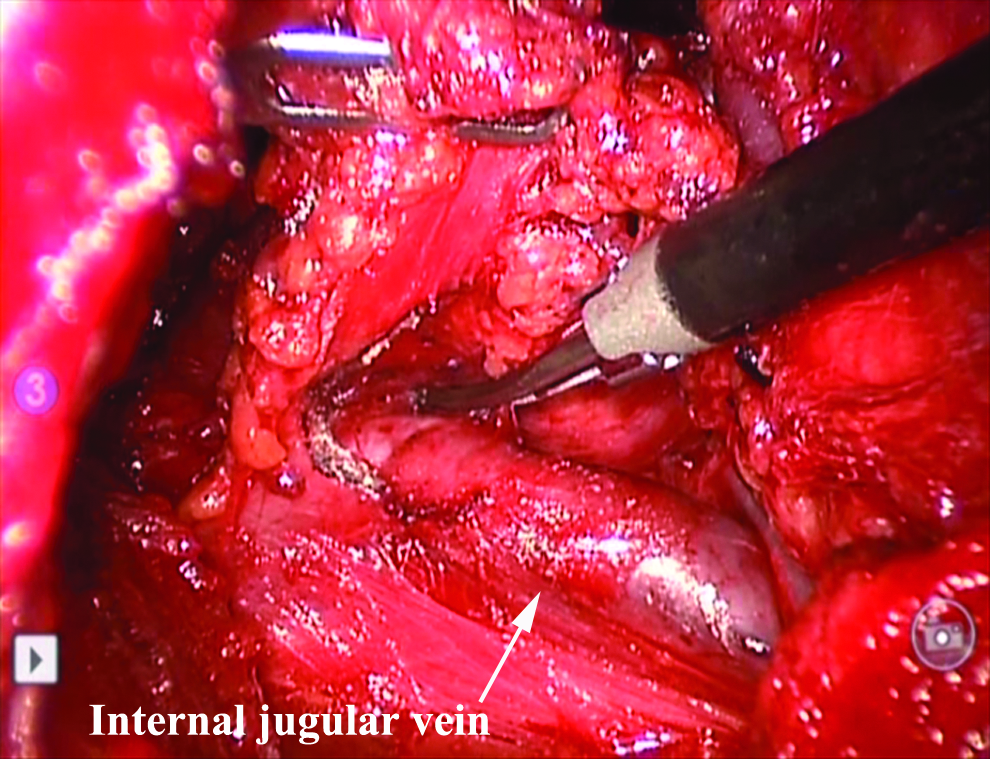
The internal jugular vein and carotid artery were unwrapped from surrounding fibroadipose tissue, and lymph nodes and fatty tissue were rolled anteriorly and freed from the overlying fascia.
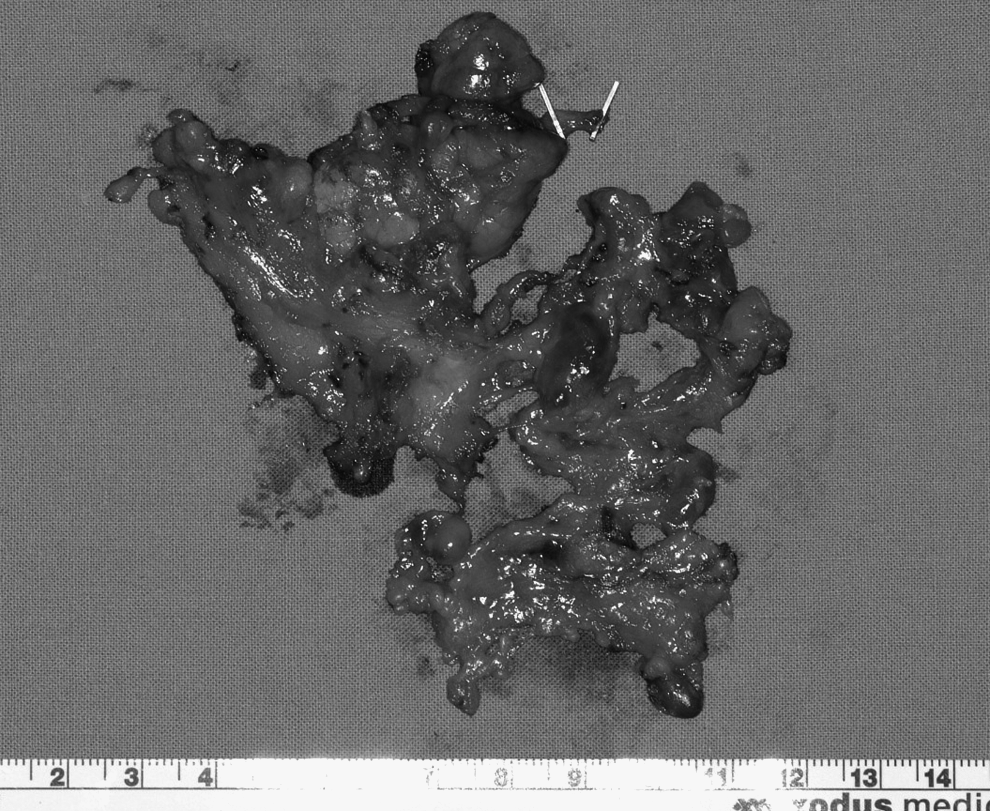
Surgical specimen from robotic selective neck dissection including levels I–III.
Results
The clinical characteristics of patients and operations are summarized in Table 1. The extent of neck dissection was from level I to level III in all patients. The entire surgical procedure of robotic selective neck dissection was completed successfully in the 4 patients, and the working space and surgical view were sufficient to dissect levels I–III. In no patients was the procedure converted to open neck dissection. The mean number of removed lymph nodes was 19.3±7.3 (5±2.8, 8.8±3.5, and 5.5±1.7 in levels I–III, respectively). The mean total operative time of robotic selective neck dissection was 276±48 minutes; the time for flap elevation was 133±47 minutes, docking time was 9.5±3.3 minutes, and console time was 115±21 minutes. The postoperative pathology N classification was N0 in all cases. The mean total amount of postoperative drainage was 290±49 mL. The mean length of the postoperative hospital stay was 10.3±2.5 days. Postoperative hematoma and transient marginal nerve palsy occurred in 1 patient each. Postoperative hematoma was easily controlled using local anesthetic, and transient marginal nerve palsy resolved within 2 months. There were no other serious postoperative complications. Cosmetic satisfaction was excellent in all patients (Fig. 9).

Postoperative photograph at 2 months after robotic selective neck dissection using a postauricular facelift approach showing excellent cosmesis.
SCC, squamous cell carcinoma; TORS, transoral robotic surgery.
Discussion
A trend toward minimally invasive or scarless surgery has developed over the past three decades in all fields of surgery, including curative-intent cancer surgery of the head and neck. The high rate of toxicity associated with chemoradiotherapy and the high rate of surgical morbidity associated with radical surgeries have led clinicians to consider alternative minimally invasive approaches for the management of HNSCC. Minimally invasive approaches for primary tumors of head and neck include transoral CO2 laser microsurgery and TORS. TORS using the da Vinci Surgical System can be a safe, feasible, and minimally invasive alternative to classic open surgery for patients with early head and neck cancer. The main advantage of using the da Vinci robot in transoral surgery is that its three-dimensional visualization overcomes the limitations imposed by the line-of-sight visualization associated with traditional endoscopic procedures or transoral CO2 laser microsurgery.
Besides minimally invasive surgery for the primary sites of head and neck cancer, there are few trials of scarless surgery or minimally invasive approaches for neck dissection. Management of cervical lymph node metastasis remains the keystone of the treatment of head and neck cancer. The presence of metastatic cervical lymph nodes in head and neck cancer can reduce survival rates by half and is a very important prognostic factor. Hence, appropriate treatment of cervical metastasis should be considered, and neck dissection can be a suitable option. The patterns of nodal spread in HNSCC are relatively predictable, so selective neck dissection is an effective procedure in patients with clinical N0 necks for staging or treatment of occult lymph node metastasis. The extent of selective neck dissection is dependent on the primary site and the extent of primary tumors. Selective neck dissection including levels I–III is an appropriate procedure for oral cancer, and selective neck dissection including levels II–IV is appropriate for oropharyngeal, laryngeal, and hypopharyngeal cancer. Modified radical neck dissection preserving the spinal accessory nerve, internal jugular vein, and SCM muscle is as effective as radical neck dissection for management of cervical lymph node metastasis. Radical neck dissection should probably be reserved for extensive neck disease, such as that involving large or multiple nodes and fixed nodes.
Modified radical neck dissection or selective neck dissection is usually done through a large cervical incision such as a modified Schobinger incision, Conley incision, L-shaped incision, or transverse incision. To minimize long cervical scars in lateral neck dissection, some authors described the feasibility of a minimally invasive video-assisted lateral neck dissection using a small cervical incision for papillary thyroid carcinoma (PTC).11,12 Lateral neck dissection using endoscopy or robots through a remote incision was initially considered challenging because of difficulties with visualization and access. The first endoscopic lateral neck dissection was performed on a cadaveric model using three different incisions in the neck. 13 Most endoscopic or robotic lateral neck dissection has been performed for the treatment of PTC. Kang et al. 9 performed robot-assisted selective neck dissection including levels II–V via a transaxillary approach with a small anterior chest port in PTC patients with lateral compartment lymph node metastasis, and the preliminary result of lateral neck dissection including levels III and IV in PTC patients via an endoscopic breast approach was also reported. 10
In this study, we performed robotic selective neck dissection in early HNSCC patients with clinically negative necks. Because the oncologic safety of robotic lateral neck dissection is not determined, we excluded HNSCC patients with clinically positive necks, who require comprehensive therapeutic neck dissection. We found that selective neck dissection including levels I–IV is possible via a postauricular facelift incision after gaining experience of parotidectomy or benign neck mass excision using a modified or postauricular facelift incision. 14 In addition, several authors have reported the use of a retroauricular incision for robotic facelift thyroidectomies or benign neck mass excision with or without endoscopy.6,15,16 In this study we used a postauricular facelift incision for selective neck dissection including levels I–III and found this allowed a clear and sufficient surgical view of levels I–III. Complete dissection of level IIB and high level IIA was also possible under direct vision without the da Vinci robot. In a postauricular facelift incision approach, level V dissection is relatively difficult because of the poor working space and inadequate surgical access. However, level V is usually not involved in HNSCC cases with a clinically negative neck, so dissection of this level can be omitted in elective neck dissection for early HNSCC patients.
In neck dissection using a robotic postauricular facelift approach, we used one endoscope and two (for the first 2 patients) or three (for the last 2 patients) robotic instruments. In the last 2 patients, we inserted a fourth robotic arm with Prograsp forceps through a small additional trocar in the lower neck area. When using three robotic instruments, surgeons can manipulate two instruments to dissect tissues while using countertraction with the third instrument. This results in improved surgeon ergonomics, which lead to substantial improvements in operating efficiency. The small lower neck incisions for the fourth robotic arm healed well and resulted in acceptable scars.
In this study, robotic selective neck dissection via a postauricular facelift approach was completed successfully in all patients. There was no conversion to open surgery in any of the operations. Complications and numbers of removed lymph nodes were comparable to those in conventional open neck dissection. The operative time was relatively long; however, it will decline after more experience. These preliminary results suggest that this procedure is technically feasible and safe. However, further studies with larger numbers of patients are necessary to determine the oncologic safety and surgical completeness of the procedure compared with conventional neck dissection. After determining the oncologic safety of the procedure and gaining more experience with it, the indication of robotic selective neck dissection might be extended to therapeutic neck dissection for small cervical lymph node metastasis.
There are some limitations of the robotic selective neck dissection in this study. The main purpose of robotic selective neck dissection using a postauricular facelift approach is to avoid a visible long cervical scar. Hence this procedure is not suitable in patients who require a transcervical incision for removal of the primary tumor, and visible cervical scarring might not be a major concern to elderly head and neck cancer patients. However, scarless selective neck dissection via a postauricular facelift incision can be a good option, particularly in the subset of patients who want scarless surgery to improve postoperative cosmesis, especially young women. Another limitation of robotic lateral neck dissection is its high cost. Robotic surgery is not covered by the national health insurance system in Korea, so patients have to pay a substantial amount. However, the disadvantages must be weighed against surgical outcomes, cosmetic benefits, and surgical ergonomics.
In conclusion, our preliminary results indicate that robotic selective neck dissection via a gasless postauricular facelift approach is feasible and safe and allows for excellent postoperative cosmesis. Further studies with larger numbers of patients are needed to determine the oncologic safety and surgical completeness of the procedure compared with conventional neck dissection.
Footnotes
Acknowledgments
This work was supported by the research fund of Hanyang University (grant HY-2011-MC).
Disclosure Statement
No competing financial interests exist.