
Abstract
Abstract
The calcifying fibrous tumor (CFT) is classified as a benign fibrous lesion, and it is a rare pathologic entity. Local excision is the preferred therapeutic approach in treating CFTs. We present the first reported case in the literature of a CFT found in the colon, and this is the first time the way we did the laparoscopic-endoscopic cooperative surgery has been introduced.
Introduction
Case Report
A 22-year-old Chinese man was seen by his primary care physician for a 1-week history of abdominal discomfort. Gastroscopy revealed a 2-×2-cm lesion in the hepatic flexure of the colon. The lesion, as viewed by endoscopy, appeared as well-circumscribed submucosal tumors with normal overlying mucosae. The endoscopic ultrasonographic features of the lesions included a mass in the muscularis propria of the colonic wall and a homogeneous hypoechoic pattern.
We have done endoscopic full-thickness resection without laparoscopic assistance for gastric submucosal tumors originated from the muscularis propria successfully in more than 60 cases. However, for colon leisons, because of the risk of peritoneal infection after colon perforation, we choose LECS as the first choice. Informed consent was obtained from the patient. The patient was kept supine, with the lower limbs spread laterally and his right side elevated, under general anesthesia. A plastic strip was applied at the ileum at a distance of 15 cm from the ileocecal valve toward the oral side, preventing gas from entering into the small intestinal tract during endoscopic treatment. The adhesions were sharply dissected by using an ultrasonically activated sealing device (Harmonic® ACE™ scalpel; Ethicon, Cupertino, CA), and the hepatic flexure of the colon was exposed. Several marker dots were made approximately along the margin of the lesion with argon plasma coagulation for location of the tumor under intraluminal endoscopy. After injection of several milliliters of submucosal injection solution into the submucosal layer, the mucosa was incised outside the marker dots with a hook knife (model KD-620LR; Olympus, Tokyo, Japan). The submucosal tissue was then gradually dissected to expose the tumor in the muscularis propria. The hook knife was used to carefully dissect the lesion along the margin of tumor and resect the whole tumor along with the serosa. Endoscopic submucosal dissection was performed under intraluminal colonoscopy to ensure complete removal of the tumor, regardless of defects in the colon wall. When the endoscopic submucosal dissection was complete, the colon wound was sutured with a laparoscopic hand-suturing technique, and a soft tube for drainage was placed near the wound (Fig. 1). Histopathologic evaluations for CFT were performed by pathologists (Fig. 2).
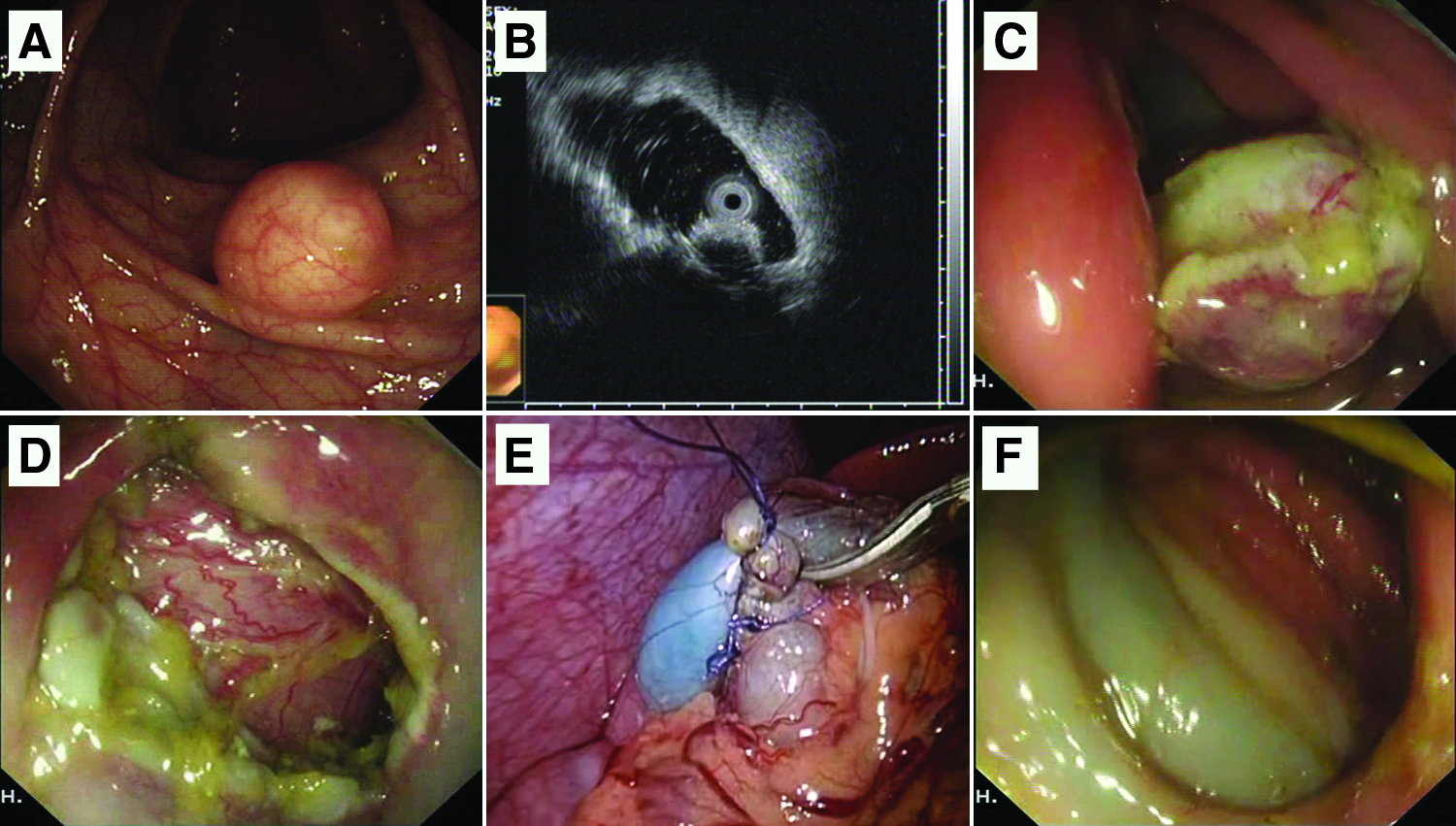
Laparoscopic-endoscopic cooperative surgery to treat calcifying fibrous tumors.
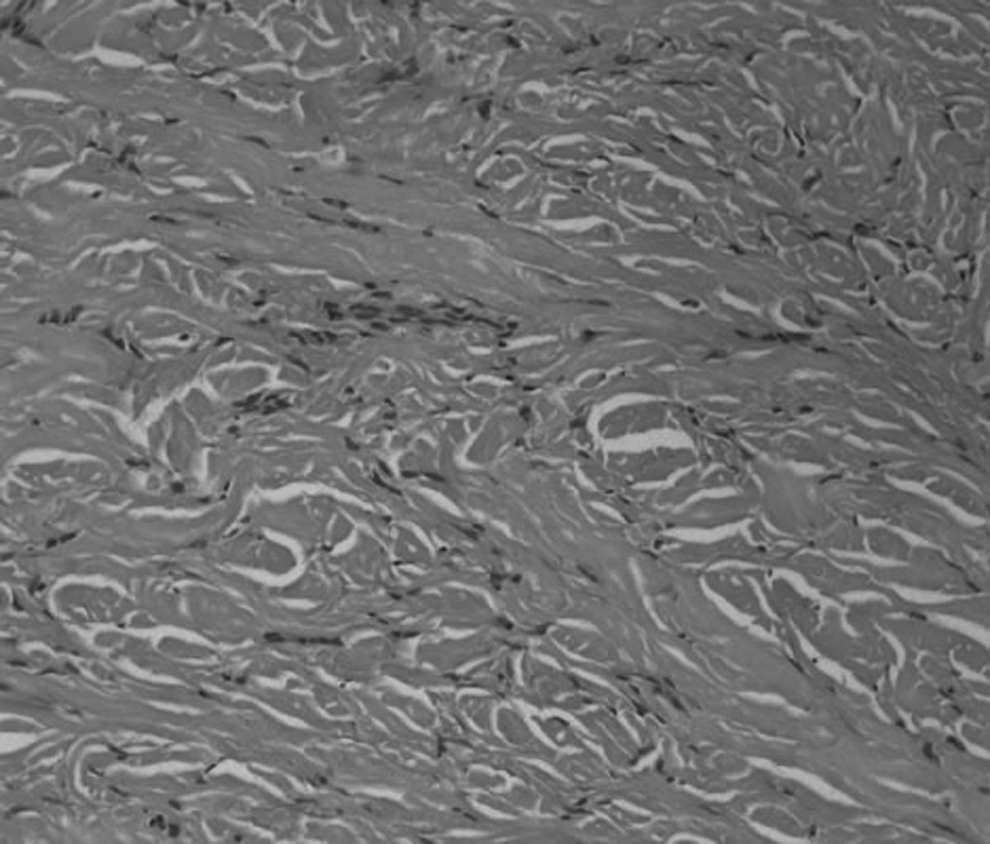
Pathologic evaluation. Hematoxylin and eosin stain. Original magnification×100.
Discussion
CFTs present as painless, benign, soft tissue or subserosal lesions with wide anatomical distribution, commonly in children, adolescents, and young adults, with no obvious sex bias. 4 With no special symptoms and no specific endoscopic/endoscopic ultrasonographic findings, it is difficult to differentiate CFTs of the gastrointestinal tract from other gastrointestinal submucosal tumors, such as gastrointestinal stromal tumors, heterotopic pancreas, carcinoid tumors, lipomas, inflammatory myofibroblastic tumors, and reactive nodular fibrous tumors. Histologically, CFTs are characterized by a proliferation of bland (myo)fibroblastic spindle cells embedded in a dense, hyalinized stroma, showing variable degrees of mineralization and inflammation.4,5 Immunohistochemical studies demonstrate that the lesional cells are immunoreactive for vimentin and variably immunoreactive for muscle-specific actin, smooth muscle actin, desmin, and CD34. However, the stain for anaplastic lymphoma kinase is negative. 2
CFT recurrence following excision has been reported, and this recurrence had the same morphology as the primary lesion. 6 However, recurrence occurs primarily when the initial resection is incomplete, and malignant transformation has not been reported, so simple, local excision is still the preferred therapeutic approach in treating CFTs. Although convenient, when using conventional surgery or laparoscopic surgery, it is sometimes difficult to identify a precise resection area without the assistance of a gastroscope. Furthermore, when excising larger areas, operative complications, such as indigestion, obstruction, and adhesion, can easily occur.
Endoscopic submucosal dissection was initially developed in Japan for the resection of early gastric cancer. Recently, with improvements in technology, it has been used not only for mucous layer tumors, but also for muscularis propria tumors of the digestive tract, which has produced good therapeutic effects.7,8 The CFT lesion in this study originated from the muscularis propria and was extraluminal-growing. Perforation is likely to occur during endoscopic resection of this kind of lesion. For gastric lesions, we could repair the perforation using metallic clips and endoloops. But for colon lesions, because of the risk of peritoneal infection after colon perforation, we choose LECS as the first choice. We can resect the lesion by endoscopic submucosal dissection, reducing the normal tissue resection and repairing the colon wall defection by laparoscopy. As well, we could wash the operation area and put a soft tube for drainage, which can reduce the infection risk.
In conclusion, CFTs are difficult to diagnose when relying only on features derived from gastroscopy and endoscopic ultrasonography. LECS appears to be a feasible and safe procedure for not only diagnosis but also treatment. However, more experiences are needed to confirm our results.
Footnotes
Acknowledgments
This work was supported by grants from the Science and Technology Commission of Shanghai Municipality (numbers 09DZ1950102, 09411967100, and 10411969600) and from the National Nature Science Foundation of China (numbers 81101566 and 11071046).
Disclosure Statement
No competing financial interests exist. Y.-S.Z. and M.-D.X. designed the research. L.-Q.Y. and Q.S. analyzed and interpreted the data. Q.S. and H.-F.W. drafted the article. P.-H.Z. and M.-D.X. undertook a critical revision of the article for important intellectual content. L.-Q.Y. and Y.-S.Z. provided final approval for the article. All the authors read and approved the final manuscript.