
Abstract
Abstract
Background:
Safe and effective retraction of the liver is essential in providing adequate working space and a proper view of the stomach during laparoscopic bariatric surgery. Conventional liver retractors are expensive, require additional ports, resulting in pain and scarring, and cannot be utilized for single-port surgeries. To overcome these limitations we present a novel technique, using an indigenous “T-suspension tape,” for liver and gallbladder retraction.
Patients and Methods:
A retrospective analysis of the first 12 bariatric procedures using the “T-suspension tape” for liver retraction is presented here. The tape was created using the Teflon® (Dupont, Wilmington, DE) tail of a Jackson–Pratt drain secured to a Prolene™ (Ethicon, Blue Ash, OH) suture on a long straight needle. The liver was retracted by transparenchymal passage of the needle, which was exteriorized and secured to the anterior abdominal wall.
Results:
There were 11 female patients and 1 male patient. The mean age was 30 years (range, 20–42 years), and the mean preoperative body mass index was 37.37 kg/m2 (range, 33.14–48.98 kg/m2). There were six laparoscopic sleeve gastrectomies (including one single-incision procedure), two laparoscopic Roux-en-Y gastric bypasses, four laparoscopic adjustable gastric banded plications, and three concomitant cholecystectomies. Mean time for retraction was 4 minutes 33 seconds (range, 38 seconds to 20 minutes 20 seconds). The liver and also the gallbladder could be effectively retracted, providing excellent working space and visualization of the entire stomach. There were no complications or conversions associated with this technique.
Conclusions:
The “T-tape suspension” technique is simple, safe, and inexpensive and provides efficient retraction of the liver and gallbladder during bariatric surgery.
Introduction
Patients and Methods
This study included the first 12 patients in whom the TST was used for various bariatric procedures, namely, laparoscopic Roux-en-Y gastric bypass, laparoscopic sleeve gastrectomy, and laparoscopic adjustable gastric banded placation, including multiport and single-incision procedures and concomitant cholecystectomies. The study was performed between January 2012 and March 2012, after approval by the Institutional Review Board. Informed consent was obtained from all patients. The inclusion criteria were based on the 2005 Asian Pacific Bariatric Surgery Society guidelines for bariatric surgery 9 (age between 18 and 65 years and body mass index of 32 kg/m2 with obesity-related comorbidities or body mass index of >37 kg/m2 irrespective of comorbidities). The data of these patients were retrospectively reviewed from a prospectively maintained database. The data analyzed included patient demographics, time taken for retraction with each tape, operative time, and complications.
Making the TST
The TST could be easily constructed in two steps, from commonly available surgical materials as follows.
Materials required
The materials required included:
1. A Jackson–Pratt drain, which has three parts, namely, a fenestrated Teflon® (Dupont, Wilmington, DE) tail, the central tube, and a bulb. 2. 2/0 monofilament polypropylene suture (Prolene™; straight taper point, ST-70, W8400; Ethicon, Blue Ash, OH) with a long straight needle. 3. Surgical scissors and needle holder.
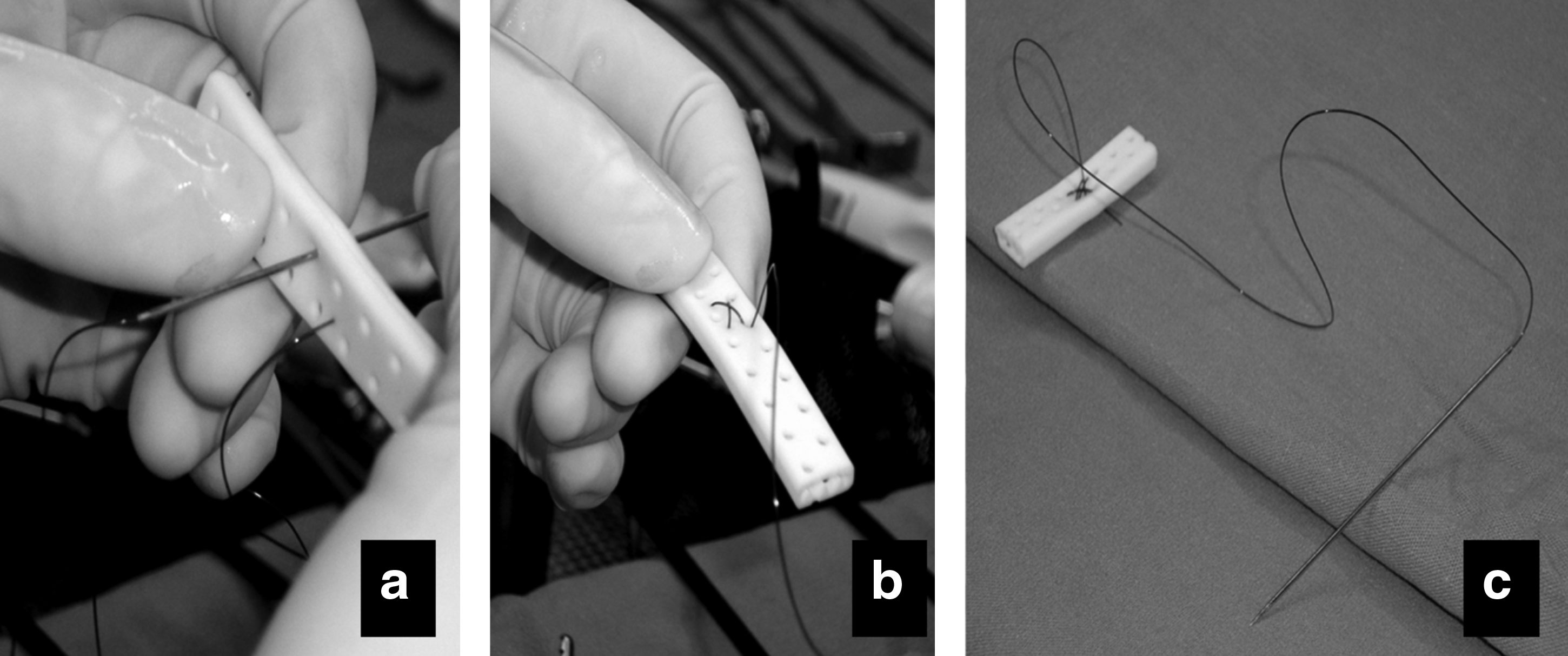
Steps
The TST was constructed in two steps:
1. A 2–5-cm length of the Teflon tail of the Jackson–Pratt drain was cut off. Smaller lengths are used for gallbladder retraction. 2. The Prolene suture was passed to the midportion of the Teflon tube and secured with multiple passes (three or four) at the center, forming a T-shape with the needle still attached at the end of the suture (Fig. 1).
Operative technique
General considerations
All the procedures were performed with the patient under general anesthesia, supine, with the legs together and maintained on anti–deep vein thrombosis stockings. Four trocars were placed for conventional bariatric procedures, and three transumbilical trocars were inserted for single-incision surgery. The operating surgeon stood on the right side throughout the procedure. Pneumoperitoneum was created using a long Veress needle (in the left upper quadrant), after which the patient was placed in a steep reverse Trendelenburg position. The intra-abdominal pressure was maintained at 17 mm Hg.
Technique of retraction: liver, gallbladder, and falciform ligament (Fig. 2)
The newly created TST was grasped on the Teflon limb using the needle holder, introduced into the peritoneal cavity through the largest port (12–15 mm), and directed toward the left upper quadrant. Once inside the abdomen, the needle was grasped with a needle holder using the right hand (dominant hand), while the left lobe of the liver was gently raised (left hand) with a blunt laparoscopic instrument (bowel forceps) so as to have a clear view of the inferior surface. The needle was then passed into the inferior surface of the liver (transparenchymal) so as to exit at the superior surface. The tip of the needle (which had pierced through the superior surface of the liver) was exteriorized by piercing the anterior abdominal, where it was grasped by a hemostat, gently pulled up, and clamped close to the abdominal wall. This maneuver lifted the left lobe of the liver along with it. The liver was thus retracted and maintained in position, supported by the Teflon limb of the Jackson–Pratt drain. The needle was then cut off from the suture, while the hemostat gripped the Prolene to maintain the retraction. The degree of liver retraction could be adjusted by manipulating the tension on the suture with the help of the hemostat.
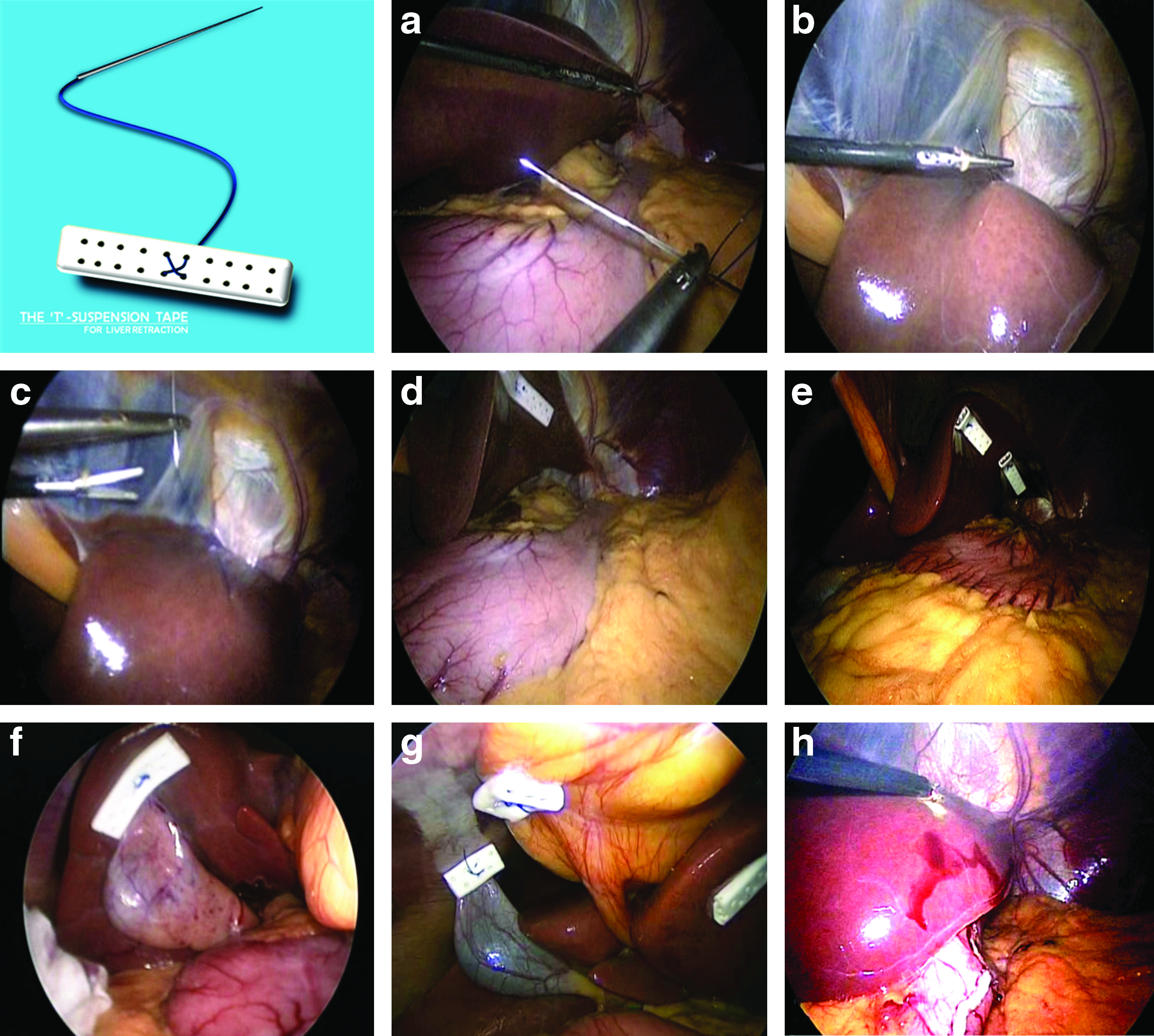
After completion of the procedure the hemostat was released, and the Teflon limb was delivered out through the port. Minimal bleeding at the entry and exit points was secured by one or two touches of the hook cautery.
Concomitant cholecystectomy was done in patients who had preoperative evidence of gallstones. For retracting the gallbladder the needle was passed through the fundus of the gallbladder or, alternatively, into the right lobe of the liver adjacent to the fundus of the gallbladder (Fig. 2g and h). The needle was passed through the falciform ligament in order to retract the ligament.
Results
The TST was used in 12 patients (11 females and 1 male). The mean age was 30 (standard deviation 6.768913) years (range, 20–42) years, and the mean preoperative body mass index was 37.37 (standard deviation 4.89) kg/m2 (range, 33.14–48.98 kg/m2). The bariatric procedures included six laparoscopic sleeve gastrectomies, two laparoscopic Roux-en-Y gastric bypasses, and four laparoscopic adjustable gastric banded plications (Table 1). The mean operating time was 77 minutes 20 seconds. The mean time for accomplishing retraction with the TST was 4 minutes 33 seconds (range, 38 seconds to 20 minutes 20 seconds). Three patients underwent concomitant cholecystectomy. In these patients TST was also used for retracting the gallbladder, and in 1 patient an additional tape was required for retracting the falciform ligament. In the case of larger livers additional tapes were added to attain adequate retraction. The majority of the patients required more than one TST. A shorter amount of time was needed to deploy additional tapes for multiport surgery. The liver could be effectively retracted in all the cases, providing excellent working space and visualization of the gastrohepatic ligament, hepatoduodenal ligament, and esophageal hiatus. There were no conversions to open surgery and no need for deploying conventional liver retractors. There were no complications associated with this technique.
Time values are given as minutes:seconds.
BMI, body mass index; LAGBP, laparoscopic adjustable banded plication; LC, laparoscopic cholecystectomy; LSG, laparoscopic sleeve gastrectomy; LYRGB, laparoscopic Roux-en-Y gastric bypass; SITU, single-incision transumbilical surgery; T1, time for deploying first tape; T2, time for deploying second tape; T3, time for deploying third tape; T4, time for deploying fourth tape.
Discussion
In bariatric surgery, proper and safe retraction of the liver is essential in providing a good operating field in terms of both working space and vision. In addition to the commercially available retractors, various innovative and cost-effective techniques have been described by enthusiasts. These techniques have their own advantages as well as disadvantages and have been described mainly for procedures like gastrectomy and liver and gallbladder surgeries.
Commercially available mechanical retractors require additional incisions, often produce liver congestion, 10 and cannot be used for single-incision laparoscopic procedures. They are also known to cause iatrogenic liver injuries.11,12
The use of transabdominally placed suture retraction techniques is not new and has been described earlier for various laparoscopic surgeries but has not gained widespread acceptance in bariatric surgery. Lee et al. 13 described a liver puncture technique for liver retraction during laparoscopic gastrectomy for gastric cancer, using a straight needle with Prolene suture that punctured the liver margin and exited the abdomen with the liver lobe supported over the length of the suture with gauze placed in between to prevent cut-through. With this technique they could accomplish adequate liver retraction with good exposure of hepatoduodenal and gastrohepatic ligaments, including the region from the porta hepatis to the esophageal hiatus in all the patients. There were no complications associated with this technique.
Shibao et al. 10 described a disk suspension technique using a combination of the snake retractor, silicone disk, and an elastic tape and found it to be safer than the fixed retractor during laparoscopic gastrectomy for gastric cancer. However, this technique requires special instruments and an additional port for the snake retractor and cannot be used for single-site surgeries. Galvani et al. 14 described a totally intracorporeal retraction technique, using a combination of a lonestar-hook and a bulldog clamp in 7 patients who underwent single-incision laparoscopic sleeve gastrectomy and found it to be safe and effective. Shabbir et al. 15 described a transabdominal suture technique for combined retraction of the falciform ligament and left lobe of the liver during laparoscopic gastrectomy.
Our technique has numerous advantages, which are outlined in Table 2. The retractor is simple and easy to construct. The technique provides good exposure at the esophageal hiatus, hepatoduodenal and gastrohepatic ligaments, and the entire stomach. In the case of larger livers more than one T-tape can be safely used. The time taken for deploying additional tapes is much lesser. The procedure is less invasive as it obviates the need for additional ports/wounds, translating to better cosmesis and reduced wound-related complications. Following the use of fixed retractors we often noticed that the liver gets congested after a certain time, necessitating frequent release or readjustments and thereby interrupting the smooth flow of surgery. This did not happen with the TST technique. We have already published a randomized controlled trial comparing three methods of liver retraction in laparoscopic Roux-en-Y gastric bypass, wherein we demonstrated a significant rise in levels of aspartate aminotransferase and alanine aminotransferase while using fixed retractors compared with liver puncture technique using the liver suspension tape. 16 Another unique feature of the TST is that it can be used to retract the right and left lobes of the liver, the gallbladder, and even the falciform ligament either in isolation or in combination. Moreover, the Teflon tape evenly distributes the pressure and reduces the risk of cutting-through. This technique is much easier to perform and more versatile than the liver suspension tape. The TST is smaller and has only one needle and therefore is more agile, and the process of insertion into the abdomen and the intra-abdominal maneuverability is technically less challenging compared with the liver suspension tape. The potential disadvantage of the technique is that it requires penetrating the liver, and there is a perceived risk of liver injury. We have not experienced any such complications using this technique. Lee et al. 13 also used a liver puncture technique, without complications. The bleeding is minimal, and in some cases there is no bleeding at all, even after the needle puncture, as is obvious from Figure 2b and c. The time taken for retraction is also very much shorter. The technique is also advantageous for single-incision surgery, as seen in this series. Based on this initial experience we believe that the TST liver retraction technique is safe and effective during bariatric surgery; however, more detailed studies based on a larger patient cohort along with analysis of liver function tests and comparisons with other available methods are needed to ascertain the true benefits of this technique.
Conclusions
The TST method is a safe, simple, efficient, cost-effective, and feasible technique for retracting the liver, gallbladder, and falciform ligament in laparoscopic bariatric procedures. Further research is needed to determine the true potential of the technique.
Footnotes
Acknowledgments
The authors would like to thank the entire staff of the bariatric surgery center at E-da Hospital for their help in obtaining the necessary information required for this article and especially thank Miss Ivy Huang, the case manager, for helping with the data retrieval.
Disclosure Statement
No competing financial interests exist.