
Abstract
Abstract
The Morgagni-type anterior diaphragmatic hernia is a congenital defect that is a very uncommon hernia presenting in an adult. Surgical repair is usually recommended upon diagnosis and often requires synthetic mesh for a durable, tension-free repair. The use of synthetic mesh concurrently with several of bariatric operations is controversial owing to the potential for mesh infection. In this report we describe a laparoscopic repair of a symptomatic Morgagni hernia with synthetic mesh, concurrently with sleeve gastrectomy, in a morbidly obese man. The patient was a 58-year-old man with a body mass index of 48 kg/m2 and associated co-morbid conditions that included obstructive sleep apnea, hypertension, hyperlipidemia, impaired fasting glucose, and osteoarthritis. He was diagnosed with Morgagni hernia with exertional dyspnia. He underwent concurrent laparoscopic Morgagni hernia repair with mesh and sleeve gastrectomy. At 2 months after surgery the patient was doing well and tolerating solid foods, and his percentage excess weight loss was 35%. He was exercising regularly and had no exertional dyspnea. Laparoscopy is an attractive approach to performing multiple intra-abdominal procedures concurrently. The Morgagni hernia repair with mesh can be performed safely and effectively using a laparoscopic approach. This can be performed concurrently with bariatric surgery in the morbidly obese.
Introduction
The use of synthetic mesh in the setting of bariatric surgery is still controversial, owing to the potential risk of mesh infection. However, evidence has emerged to suggest the safety of this practice in patients with abdominal wall hernia repair concurrent with bariatric surgery. 10 In this study we describe a case of a patient undergoing a concurrent laparoscopic repair of a symptomatic Morgagni diaphragmatic hernia with mesh and sleeve gastrectomy for morbid obesity.
Case Report
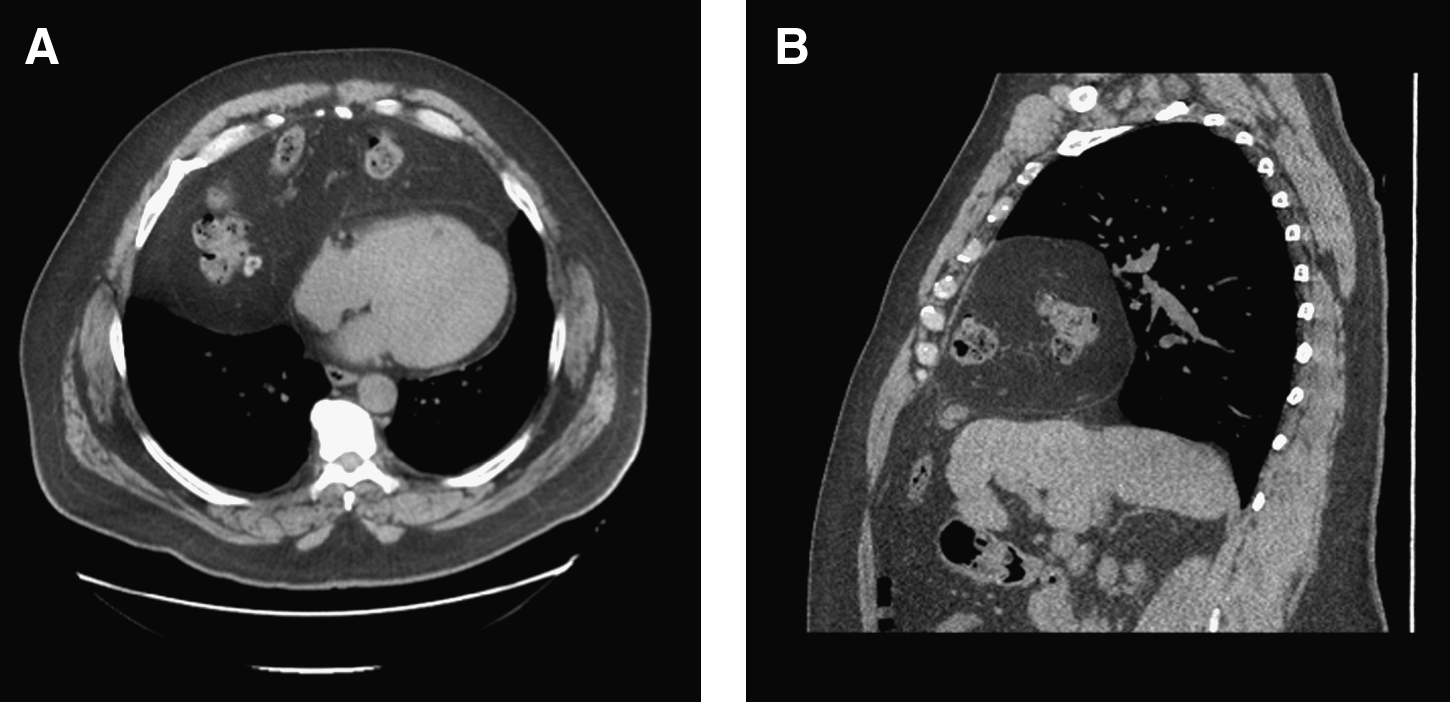
The patient was a 58-year-old man with a body mass index of 48 kg/m2 and associated co-morbid conditions that included obstructive sleep apnea, hypertension, hyperlipidemia, impaired fasting glucose, and osteoarthritis. He underwent an extensive multidisciplinary evaluation for bariatric surgery. He was noted to have a mild dyspnea on exertion or when bending over to tie shoes, and work-up revealed a large anterior diaphragmatic hernia (Morgagni type) with herniated transverse colon and omentum (Fig. 1). He had no associated gastrointestinal symptoms, no chest pain, and no cough, and physical exam was unremarkable. He presented electively for a combined Morgagni hernia repair and sleeve gastrectomy by the laparoscopic approach.
Selected
Laparoscopic Morgagni hernia repair
The operation was performed with the patient in the supine position and the table in the reversed-Trendelenburg position. The abdomen was accessed using Veress needle entry in the left upper quadrant, and the abdomen was insufflated to 15 mm Hg with CO2. Five ports were introduced using our standard approach to bariatric surgical procedures, including a right abdominal port for retraction of the left lateral segment of the liver and a left midabdominal port for introduction of a 30° 5-mm laparoscope that was used throughout the operation.
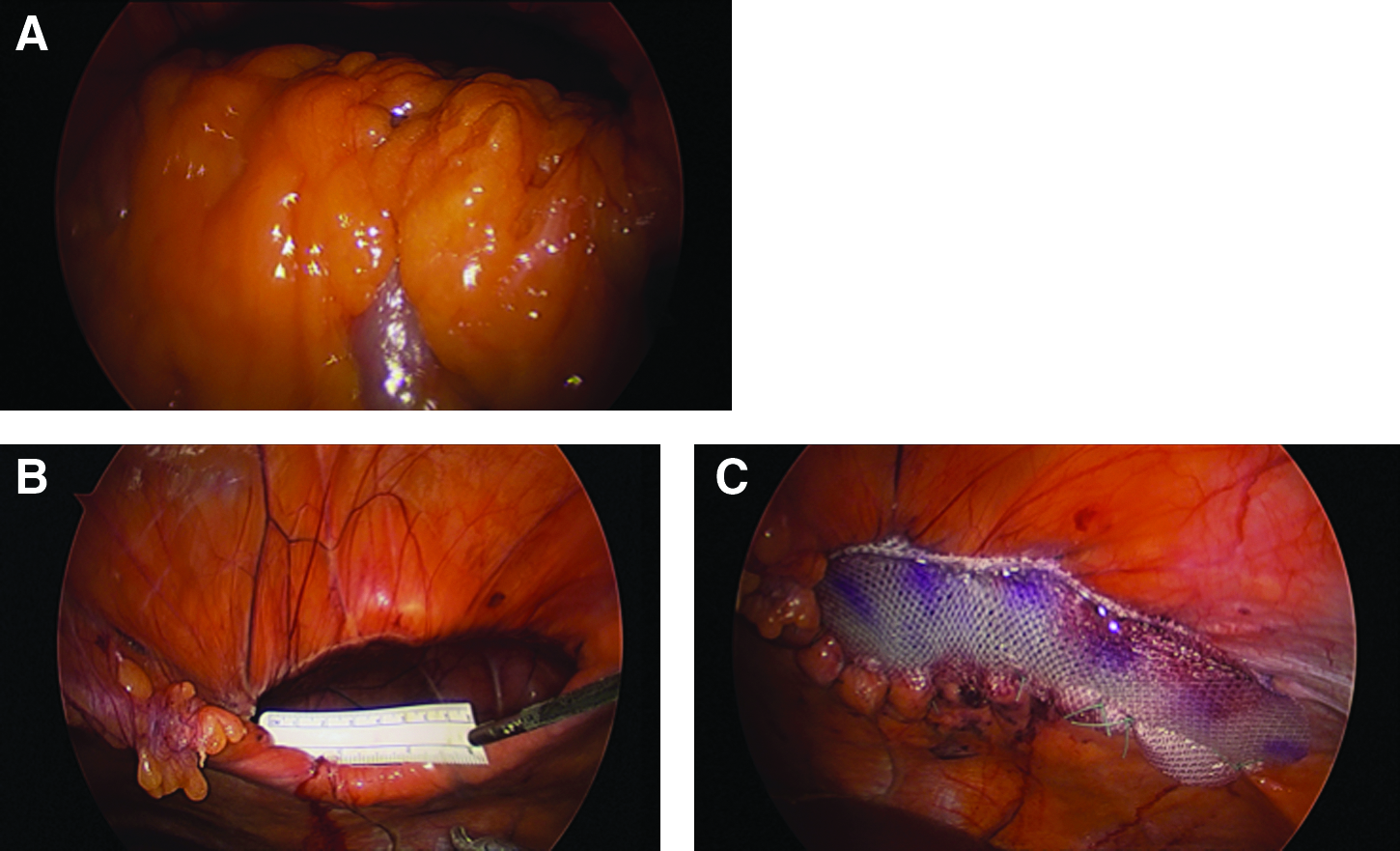
We first reduced the herniated transverse colon and omentum, to allow us later access to the stomach for sleeve gastrectomy. After the contents were reduced, we approached the repair of the diaphragmatic defect. It measured 6 cm across, had an absence of the anterior diaphragmatic rim, and was deemed to be too large for primary repair. A 14-×8-cm Parietex™ composite mesh (Covidien, Mansfield, MA) was introduced into the abdomen for repair. Multiple interrupted 2-0 polyglactin 910 (Vicryl™; Ethicon, Blue Ash, OH) sutures, spaced 1 cm apart, were used to secure the posterior portion of the mesh to the diaphragm. A suture-passer was used to deliver multiple transfacial 2-0 Vicryl sutures in the anterior portion of the mesh, which were then secured to the anterior abdominal wall (Fig. 2).
Laparoscopic view of
Sleeve gastrectomy
The operation was started with mobilization of the greater curvature of the stomach using a LigaSure™ device (Valleylab, North Haven, CT). The gastric sleeve was created using the Echelon stapler (Johnson & Johnson, New Brunswick, NJ) buttressed with SeamGuard® (Gore, Flagstaff, AZ). It was initiated approximately 6 cm proximal to the pylorus and completed approximately 1 cm to the left of the angle of His. A 36 French endoluminal endoscope was used to size the lumen and perform a leak test intraoperatively, and a Jackson Pratt drain was placed along the staple line at the conclusion of the operation. The duration of the entire operation was 200 minutes.
The postoperative course was uncomplicated, and the patient was discharged to home on postoperative Day 2 tolerating a liquid diet. At 2 weeks after surgery a chest radiograph demonstrated interval repair of the anterior diaphragmatic hernia with a small amount of residual mediastinal fluid (Fig. 3). At 2 months after surgery the patient was doing well and tolerating solid foods, and his percentage excess weight loss was 35%. He was exercising regularly, had no exertional dyspnea, and noted a general improvement in symptoms.

Discussion
The use of prosthetic mesh hernia repair in the setting of a clean-contaminated operation is slowly gaining acceptance, although it is still avoided when possible for fear of mesh infection. There have been multiple reports supporting the use of prosthetic mesh in the setting of ventral hernia repair and simultaneous gastric bypass surgery.11–13 These studies have demonstrated that infection and recurrence rates do not increase in these combined operations. It is common practice to delay ventral hernia repair until after bariatric surgery that requires violation of the gastrointestinal tract. However, deferred management of the hernia in these obese patients undergoing rapid weight loss in the postoperative period may be associated with increased morbidity. Bonnati et al. 14 demonstrated that as many as 37.5% of gastric bypass patients who were deferred treatment of ventral hernias presented with small bowel obstruction in the postoperative period, necessitating urgent surgical intervention.
Concomitant use of mesh has not only been studied in the context of gastric bypass operations, but other clean-contaminated operations as well. These studies have shown the safety of prosthetic repair of fascial defects in settings such as colon and gallbladder surgery.15–19 To date, this study uniquely describes the use of synthetic mesh to repair an anterior diaphragmatic hernia, concurrently with sleeve gastrectomy for morbid obesity.
Anterior diaphragmatic hernias of Morgagni are rare entities in adults, typically warranting repair, especially when symptomatic. When small, these can be repaired primarily. However, they are often identified when large (>20–30 cm2) and require mesh for a tension-free repair.1,20,21 Synthetic mesh is preferred over biologic mesh for its durability. However, biologic mesh had often been used in the setting of concurrent gastrointestinal surgery. We performed a sleeve gastrectomy for morbid obesity and chose to repair the diaphragmatic hernia with a synthetic mesh to ensure durability of the repair. There were no short-term complications or adverse events related to mesh choice.
Footnotes
Disclosure Statement
No competing financial interests exist.