
Abstract
Abstract
Background:
Apart from the required expertise, a major deterrent to laparoscopic common bile duct (CBD) lithotomy (LCDL) remains the relatively prohibitive cost of the flexible choledochoscope, and it also has a shortcoming of not being effective in removal of large impacted CBD stones.
Subjects and Methods:
All patients presenting with CBD stones were treated, without exclusion, by laparoscopic cholecystectomy plus transdochal LCDL after relevant investigations. LCDL was performed using a rigid nephroscope. The CBD was closed either with running 3-0 polyglactin acid (Vicryl™; Ethicon) sutures without a stent or around a T tube in a few patients. Perioperative parameters were recorded in all patients.
Results:
Transdochal LCDL was performed on 172 consecutive patients. Five patients had a prior open cholecystectomy, 26 patients presented with acute cholecystitis, 5 patients presented with mild acute pancreatitis, and 12 patients presented after failed endoscopic retrograde cholangiopancreatography. Twenty-eight (16.28%) patients had multiple stones, 2 had biliary sludge, and no stone was found in 3 patients. Stone size varied from 4 to 12 mm. The average operative time was 68 minutes (range, 45–127 minutes). Primary repair was performed with 3-0 Vicryl continuous sutures, and the T tube was left in place in 13 (7.56%) patients. Conversion to an open procedure was required in 8 patients (4.65%). Postoperatively, mild acute pancreatitis occurred in 1 patient, and biliary peritonitis occurred in 5 patients.
Conclusions:
Rigid scope transdochal LCDL is feasible, probably easier, better for impacted large CBD stones, and definitely more affordable.
Introduction
Subjects and Methods
All patients with gallbladder stones and CBD stones were treated with LC and laparoscopic CBD exploration or LCDL. All 172 patients underwent transdochal LCDL. None of the patients was referred for ERCP.
Four or five ports (two 10-mm and three 5-mm) were used for transductal LCDL (Fig. 1). A 6° 5-mm rigid nephroscope with a working channel was used. Two cameras were used, with the second camera for the nephroscope. The infraumbilical 10-mm port was for the telescope. The second 10-mm port is a working port and was positioned to the left of the midline midway between the xiphoid and the umbilicus. The positioning was beneficial in two respects. First, the nephroscope entered the proximal CBD and the common hepatic duct in a straight line without causing any traction injury. Second, the needle holder through this port makes the CBD suturing process easy and ergonomic. This port, when positioned at the usual epigastrium site, has both of the above disadvantages, and suturing is very uncomfortable. The first 5-mm port was the usual right subcostal–in-midclavicular line for gallbladder retraction and manipulation. The second 5-mm port high up in the right epigastrium accommodates the nephroscope for visualization of the distal CBD up to the duodenum, again in a straight line, without any traction injury on the CBD. During the suturing process this port accommodates the grasper for retracting the gallbladder as the subcostal port accommodates the suture grasper. The fifth port, when needed, was positioned in the anterior axillary line midway between the costal margin and the transumbilical line.
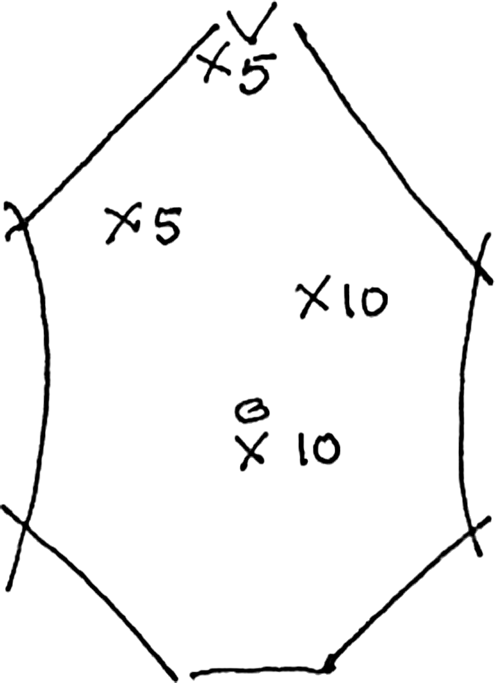
Port placements.
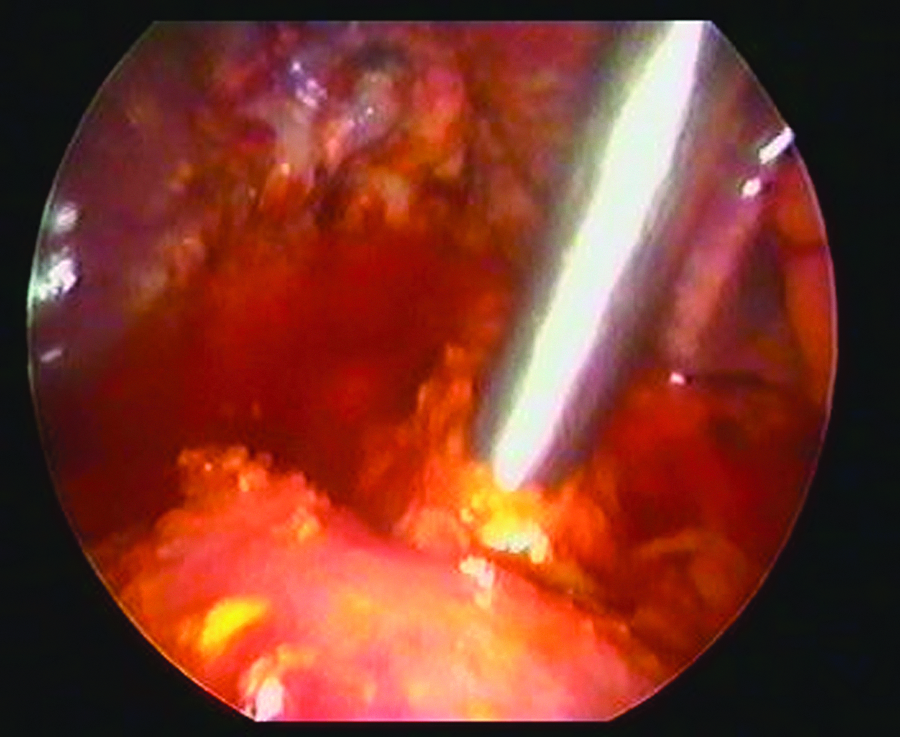
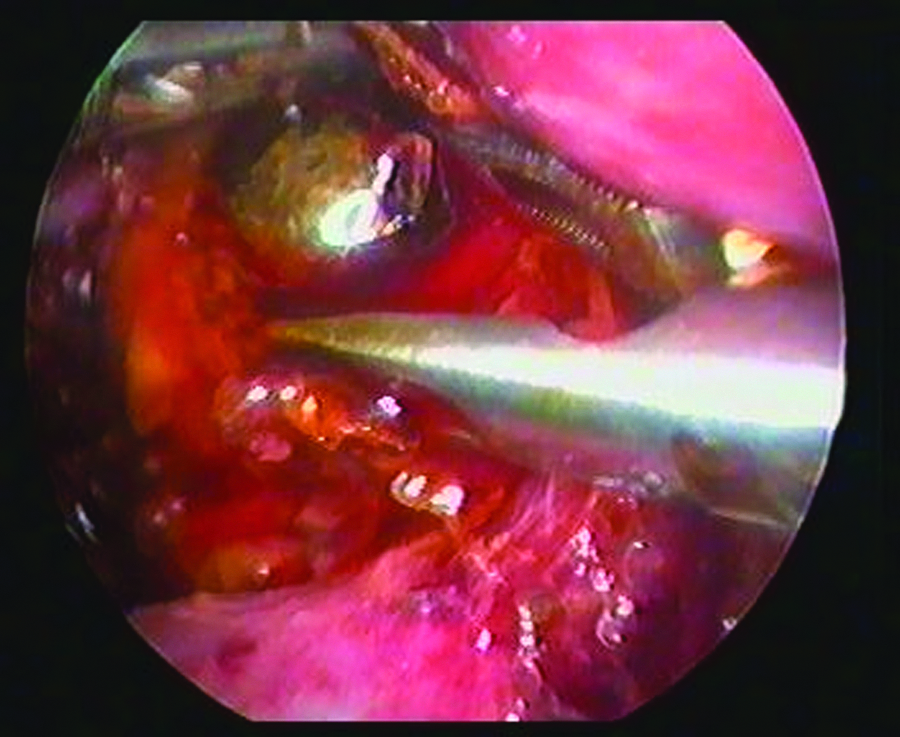
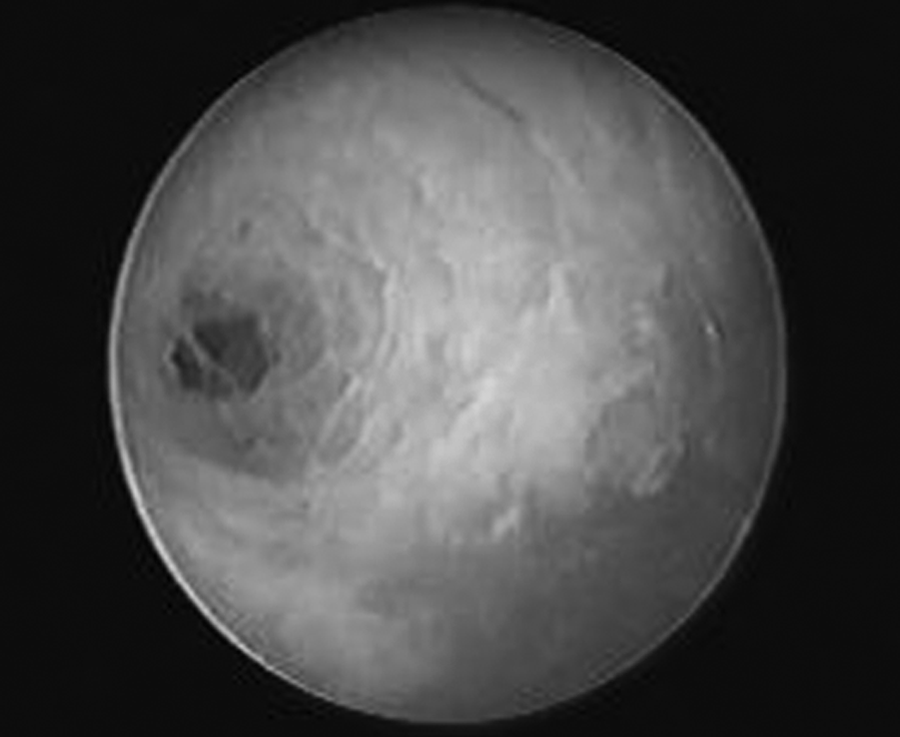
The first step included dissection and ligation of the cystic artery and duct and mobilization of the gallbladder except the terminal most fundal attachment. The anterior surface of the CBD was cleared off the anterior leaf of the visceral peritoneum using either a Harmonic® scalpel (Ethicon Endo-Surgery) or electrocautery. The CBD was opened midway in the supraduodenal part with an endoscopic knife and enlarged with scissors. The proximal and distal segments were thoroughly irrigated with saline at high pressure. The nephroscope was then introduced through the working 10-mm port into the proximal CBD and common hepatic duct, in a straight line (Fig. 2). It was then introduced through the epigastric 5-mm port, again in a straight line, to visualize the distal CBD (Fig. 3). The stone or stones were easily and clearly visualized in the distal CBD (Fig. 4). A 3-mm three-pronged grasper or an atraumatic grasper was used through the working channel of the nephroscope, and the stone or stones were extracted in toto (Figs. 5 and 6) or after crushing. Stones impacted at the terminal CBD may be pushed into the duodenum.

The nephroscope is introduced through the 10-mm port to visualize the proximal common bile duct and common hepatic duct and the proximal hepatic duct opening.
The nephroscope is introduced through the 5-mm epigastric port and into the distal common bile duct.
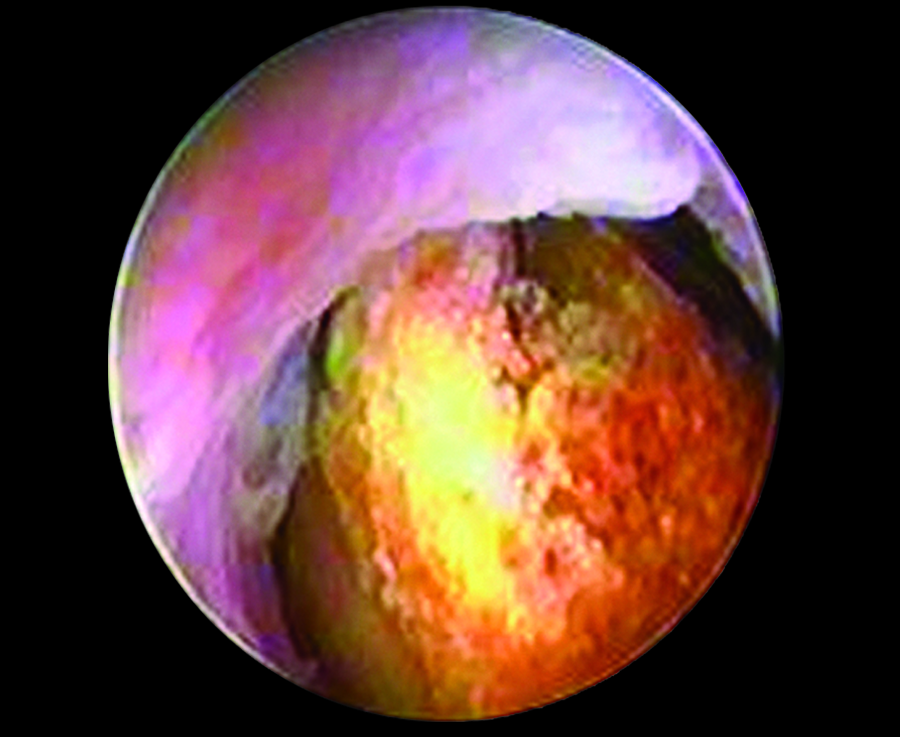
Stone seen in the distal common bile duct.
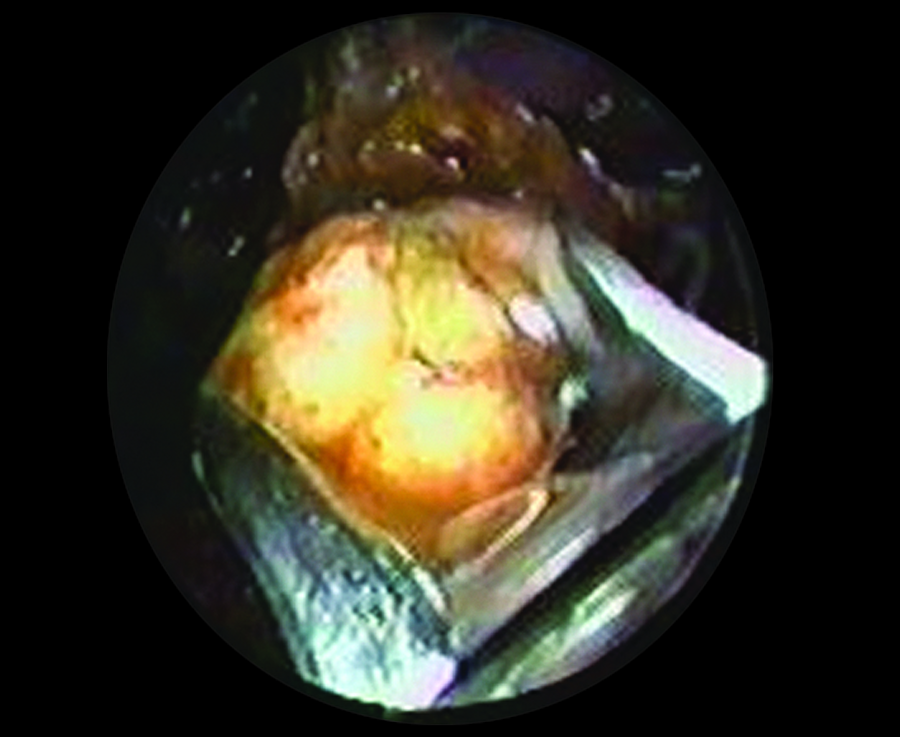
The stone is grasped with the three-pronged 3-mm grasper.
The stone is maneuvered out of the common bile duct incision.
After thorough flushing and ensuring total clearance of the CBD, by visualizing its ampullary end (Fig. 7), the CBD was closed without a stent, with continuous 3-0 polyglactin acid (Vicryl™; Ethicon) suturing. A T tube (size 12 French) was placed in patients with doubtful clearance or requiring excessive manipulation. LC was then completed, and a tube drain (FG 18) was placed in the Morrison's pouch through the subcostal port in all patients. A perioperative cholangiogram was not performed as a routine procedure but was used in patients with doubtful complete clearance.
Visualization of the cleared common bile duct and its ampullary end.
Results
The study period extended from January 2002 to May 2012. All consecutive 172 patients with CBD stones were treated with transdochal LCDL. Nineteen (11.05%) were males, and the age range varied from 13 to 78 years. Five patients had had a prior open cholecystectomy, 26 patients presented with acute cholecystitis, 5 patients presented with mild acute pancreatitis, and 12 patients presented after a failed ERCP (Table 1). The CBD diameter ranged between 8 and 16 mm. Twenty-eight (16.28%) patients had multiple stones, 2 had biliary sludge, and no stone was found in 3 patients (Table 2). The stones measured 4–12 mm in size. The procedure could be completed with four ports (two 10-mm and two 5-mm) in 149 patients, and 23 patients required an additional 5-mm fifth port. The operative time varied from 45 minutes to 127 minutes (average, 68 minutes). Primary repair was performed with 3-0 Vicryl continuous sutures, and the T tube was left in place in 13 (7.56%) patients. Conversion to an open procedure was required in 8 patients (4.65%) (Table 3). The reason for conversion was because of nonidentifiable CBD in 2 patients and dense adhesions in 4 patients, and in 2 patients the stone could only be removed on open surgery.
ERCP, endoscopic retrograde cholangiopancreatography.
Data are number of patients unless indicated otherwise.
Data are number of patients unless indicated otherwise.
CBD, common bile duct.
The Morrison pouch drain was removed on an average of 3 days (range, 2–14 days) at the time of discharge. Three patients with a drain had an extended drainage time of more than 3 days, and 1 patient had drainage of more than 50 mL/day up to 14 days (Table 4). The time to discharge varied from 3 to 14 days (average, 3.26 days). Postoperative mild acute pancreatitis in 1 patient resolved completely within a week, and biliary peritonitis in 5 patients resolved conservatively.
Discussion
The debate between LC with LCDL at the same surgical session or ERCP followed by LC as being a better modality for managing CBD stones is still unsettled, with marginal benefit in favor of the former by virtue of the fact of it being a single-session intervention.4,5 There have been suggestions of specific indications for LCDL, but we prefer LCDL as the procedure of choice for all our patients with CBD stones. Transcystic LCDL has the main limitation of being possible only if the stone size is less than 5 mm or 8 mm in some studies.4,5 Transdochal LCDL has no such limitation but in turn has a relative contraindication of not being possible in patients with a CBD diameter of less than 6 mm.6,7
The primary impediment to LCDL is the high cost of the fiber optic flexible choledochoscope, Thus it has still not found a regular place in the armamentarium of the general laparoscopic surgeon. The use of the rigid nephroscope reduces this cost by a factor of almost 10–12. The preferred scope for CBD exploration is of course the fiber optic choledoscope, but use of an infant bronchoscope has also been mentioned, 8 as has use of a ureteroscope. 8 In contrast, rigid scopes, especially the nephroscope with a working channel, has also been used by several laparoscopists and with matching results.6,7,9
We use a rigid 5-mm 6° nephroscope for all our patients. Several studies have pointed out numerous problems and drawbacks with use of the rigid scope in the CBD. These include tear of the dochotomy incision, leading to inadvertent enlargement in the incision, for which end sutures had been advised, 6 inability to visualize the proximal CBD and common hepatic duct, 6 and difficulty in visualizing the terminal end of the CBD without duodenal kocherization. 6 We do not agree with these shortcomings and have never encountered them in any of our patients. The nephroscope when introduced through the second 10-mm port can visualize as proximal as the hepatic ducts, and when the nephroscope is introduced through the 5-mm epigastric port it can be used to visualize as distal as the duodenum through the ampulla of Vater, even without any kocherization of the duodenum. The whole idea of alternating the nephroscope port is to ensure its smooth passage along the long axis of the CBD without causing any damage to the CBD.
The procedure could be managed with only four ports in 149 (86.6%) patients. The minimal diameter of the CBD where intervention was attempted was 8 mm. Multiple stones were found in 16.28% of patients, compared with 30%–90% in other studies.6,7,9–11 The stone size varied from 4 to 18 mm.
No external energy source was required, and the stones either were teased out by milking or with a grasper or were crushed with a mechanical lithotripter and washed out or pushed into the duodenum, in that order. We had a 95.35% stone clearance with LCDL compared with 75.95%–100% as noted in other studies.1,2,9,11–13 A lithotripter with an external energy source has been mentioned in many studies.7,9 Conversion to open surgery was required in 8 (4.65%) patients: because of no identifiable CBD in 2 patients and dense adhesions in 4 patients, and in 2 the stone could only be removed on open surgery.
The operating time was 45–126 minutes (average, 68 minutes), which compared favorably with other reports for laparoscopic CBD exploration of 40–480 minutes.1,6,7,9,11
CBD closure was done with a T tube in place in 13 (7.56%) patients. Most of these patients were treated in the early part of the study, when the T tube imparted a false sense of security. In the later part of the study it was used only in patients with doubtful total clearance of the CBD or where optimal CBD closure was in doubt. T tube usage has been reported in 10%–67% of CBD closures after laparoscopic CBD exploration.2,11
Postoperative complications have been reported in 4.75%–20% of cases,1,10–13 compared with 5.2% in our present series. None of the complications was irreversible, and all responded to conservative treatment.
It must be mentioned that there was no patient selection and that patients with CBD stones with associated acute cholecystitis or acute cholangitis as well as those with associated mild acute pancreatitis were all included. These associated pathologies did not in any way alter the procedure except that dissection was more difficult in some of these patients. There are several studies in which LCDL/laparoscopic CBD exploration was carried out in patients with similar associated pathological events.2,10,14
Conclusions
The cost of the fiber optic choledochoscope should not be a limitation for the laparoscopic surgeon in performing LCDL. LCDL can be performed as easily and with equally good results with the rigid nephroscope. And, in large impacted stones LCDL with the rigid scope is easier and gives better results than the operation with the fiber optic choledochoscope.
Footnotes
Disclosure Statement
No competing financial interests exist.