
Abstract
Abstract
Evolutions in minimally invasive surgical techniques and advances in sentinel node navigation surgery (SNNS) have had considerable impact on current insights into surgical treatment of gastric cancer. Extensive data on this method of surgical application have accumulated but have been principally derived from single-institute studies. Isosulfan blue and patent blue violet have been the most frequently used dye tracers in the past; however, indocyanine green has now is increasingly popular. The double-tracer method, where dye and radioisotope tracers are used together, seems to be more effective than any single tracer. Among newly emerging adjunct techniques and promising alternative in particular are infrared ray electronic endoscopy, florescence imaging, nanoparticles, and near-infrared technology. Hematoxylin and eosin (H&E) staining is still the method of choice for the detection of sentinel lymph node (SLN) metastases. Immunohistochemical staining can be used to support H&E findings, but the equipment costs of ultrarapid processing systems are currently slowing down their worldwide spread. We believe minimally invasive function-preserving resection of the stomach, together with lymphatic basin dissection navigated by SLNs, can represent the ideal approach for SNNS to detect clinically node-negative early gastric cancer, although this remains to be elucidated. Patients with cT3 or more advanced disease should still be treated by means of standard D2 dissection.
Introduction
A significant body of knowledge relating to the use of SLN biopsy in gastrointestinal cancers has accumulated as well, with colorectal and gastric cancers being the most widely investigated kinds of gastrointestinal malignant diseases in the field.2,3 Carcinoma of the stomach remains one of the most prevalent cancers and is the second most frequent cause of cancer-related deaths worldwide, affecting hundreds of thousands of people every year. 4 The relationship between the depth of the primary tumor and the probability of metastasis to regional lymph nodes (LNs) is well recognized; a tumor invasion event confined to the submucosa carries a 10%–20% risk of subsequent LN metastasis. 4 Thus, a vast majority of patients with early gastric cancer undergo standard lymphadenectomy (D1 or D2) despite the absence of any detectable LN metastasis. According to the most current version of the Japanese gastric cancer treatment guidelines (2010), clinically node-negative gastric cancer invading submucosa should be treated with gastrectomy plus D1+ dissection (LN numbers 1–7, 8a, 9, and 11p) 5 ; moreover, SNNS is not included among the potential investigational treatment modalities.
Optimal surgical treatment for gastric cancer may be established once it becomes possible to limit resection to those areas with precise and accurate boundaries of tumoral involvement, achieving an R0 resection. Curative resection of any primary tumor situated on the gastric wall can be adequately ensured by frozen section examination of the resected margins; however, the most effective means by which to manage the related LNs and lymphatic channels draining the tumoral area are yet to be established. The SNNS concept is particularly amenable to such management as it limits the extent of lymphatic dissection, thus preventing unnecessarily increased risk of morbidity caused by the dissection and resection of tumor-free areas.
Initial studies relating to the clinical utility of SLN biopsy for gastrointestinal cancers appeared in the literature in the early 2000s and have led many researchers to focus on improving the feasibility and usefulness of sentinel node mapping in patients with gastric cancer. In fact, more than 50 reports in the English language have selectively investigated gastric cancer; the great majority of these have been published in journals that are indexed in the Medline database. To date, however, no review article has attempted to provide an overview of all aspects of the SNNS concept as reported for the management of gastric cancer. Here, we present such a systematic analysis of SNNS treatment in gastric cancer.
Materials and Methods
A Medline database search was conducted in June 2010 to identify publications in the English language literature by using the PubMed search engine and combinations of subject-related key words “sentinel” AND “gastric” AND “cancer.” This initial search resulted in the identification of 268 articles (Fig. 1). All of the retrieved articles' abstracts were then manually checked to determine the appropriateness of the topic and study objectives and design; specifically, only those articles investigating any aspect of SNNS for gastric cancer were chosen for more in-depth full-text reading. In addition, the full reference list of each article was investigated to ascertain whether they included any article not indexed by the Medline database. Review articles, editorials, letters, and technical notes were excluded. Also, studies were excluded if they comprised an amalgamated population of patients with several kinds of gastrointestinal malignancies. Finally, in total, 51 articles published between March 2001 and March 2010 were identified that met the inclusion criteria and were included in the final analysis.6–56
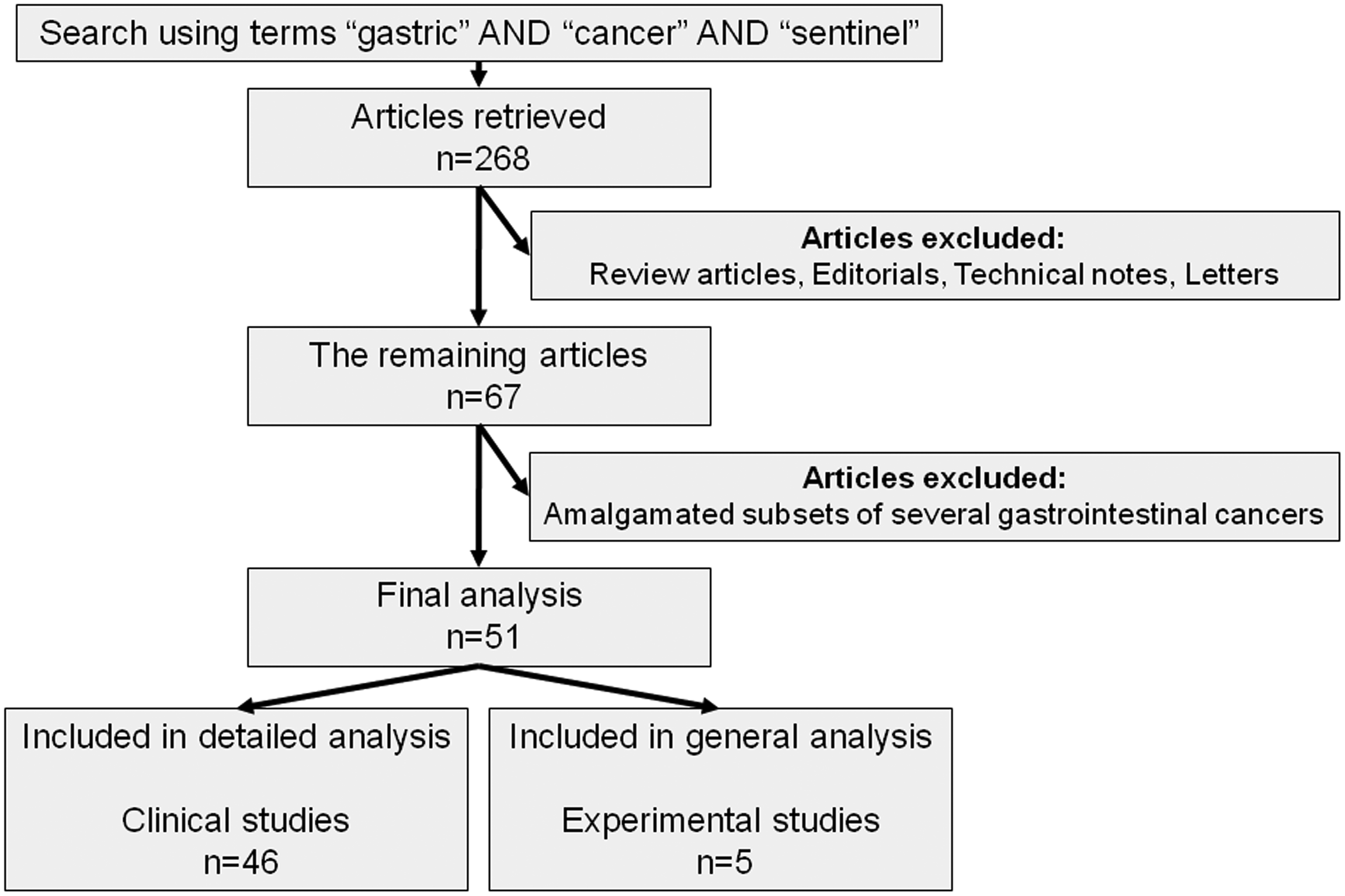
Flowchart of literature search and article retrieval.
Results
General results
Of the 51 articles analyzed, 46 (90%) were for clinical trials, and the remaining were for experimental studies (Table 1).39,41,43,50,56 All the studies were designed as prospective trials. Of these, 37 (80%) were prospective descriptive trials, whereas 9 (20%) intentionally planned to include comparative groups. There were no prospective randomized controlled or retrospective clinical trials. Of the 46 clinical studies, 3 (6.5%)14,20,48 were included in the initial general analysis but are absent from the tables presented herein that provide detailed descriptions of the articles because of trouble accessing their full-text content. Thus, frequency and average calculations were based on the remaining 43 clinical studies, unless otherwise specified. The publication dates of articles had a balanced distribution among the years. It is not surprising that Japan, where adenocarcinoma of the stomach is considered to be endemic and still remains the leading cause cancer-related deaths, 57 was by far the leading country for articles published on this topic, accounting for over two-thirds of studies conducted in this field. Researchers from South Korea followed their Japanese counterparts in terms of publication on this interesting topic, having 8 of the 51 articles published.
Researchers interested in SNNS for gastric cancer have typically been clinicians. This might be due to the fact that tracers and methods required for SNNS in this group of patients had already been extensively studied in experimental malignant melanoma and breast and colon cancer models during the period of infancy of the technique. The total number of patients enrolled in the clinical studies included in this review—irrespective of the method used for the removal of primary tumor—is approximately 2800 (Table 2). These studies have addressed several aspects of the SNNS procedure, including efficacy of novel tracers, implementation issues, injection sites and injection methods, type of surgery, and reliability and feasibility of methods used for the detection of LN metastasis. Despite considerable heterogeneity existing among the trials, parameters used to address the study topic can be categorized into three groups: (1) identification of SLNs, (2) detection of SLN metastasis, and (3) patient selection and surgical management. The review of numerical data of these subcategories is based on the analysis of clinical studies selectively.
Average number of sentinel lymph nodes (SLNs) identified or removed (as applicable).
Could not be accessed.
For combined method only.
For stage cT1 tumors.
In SLN pick-up method, where an isolated removal of SLNs is carried out.
In lymphatic basin dissection, where all related lymphatic structures are removed.
For stage cT2–3 tumors.
FI, fluorescence imaging; IR, infrared imaging videoscope; IREE, infrared ray electronic endoscopy; SR, success rate (refers to the ability of the method to identify SLNs in relation to the whole study population); SM, submucosal injection; SS, subserosal injection; 99mTc ASC, technetium-99m radiolabeled antimony sulfur colloid; 99mTc SC, technetium-99m radiolabeled sulfur colloid; 99mTc tin C, technetium-99m radiolabeled tin colloid.
Identification of SLNs
In early studies of SNNS for gastric cancer, the authors had predominantly chosen to use conventional dye and radioisotope tracers (Table 2).6–13,15–17 The dye agents used included isosulfan blue, patent blue violet, and indocyanine green (ICG). Isosulfan blue was used as a sole agent in 6 (14%) of 43 studies and in combination with technetium-99m radiolabeled tin colloid (99mTc tin C) in 2 (4.6%). It is interesting that use of isosulfan blue as a sole tracer was last reported on in the 2006 study by Saikawa et al. 34 Patent blue violet was used as a single agent and combined with 99mTc tin C in 5 (11.6%) and 6 (14%) of the studies, respectively. ICG was the most frequently used tracer, representing 17 (39.5%) of the clinical trials. ICG together with 99mTc tin C was used in 7 (16.2%) of the studies. Of interest is that analysis of the last 10 articles published since 2008 revealed that the majority of the most recently publishing authors (8 of the 10) chose to administer ICG as the tracer agent (Table 2). The radioguided method was preferred as the sole method to identify SLNs in six (14%) of the reported clinical investigations. Of these, five relied on the use of 99mTc tin C, and only one used technetium-99m radiolabeled sulfur colloid. In addition, 15 (34.9%) authors used the radiolabeled method as an adjunct to a dye-guided method; one of them, in particular, used technetium-99m radiolabeled antimony sulfur colloid as the radiolabeling substance.
Infrared ray electronic endoscopy (IREE), a novel technique that has the capability of improving the visibility of SLNs and lymphatic basins draining the tumor after dye injection, especially on fatty areas surrounding the stomach, has trended in popularity over the past 5 years.18,35,42 Except for one article published in 2004, the four studies that relied on the use of IREE were conducted between 2007 and 2010. IREE was invariably used in combination with the ICG dye-guided method. Two other novel techniques that have recently been introduced in order to improve visibility of SLNs dyed with ICG are infrared imaging videoscopy and florescence imaging. Two articles published in 2008 and 2009 reported on using infrared imaging videoscopy and florescence imaging techniques in SNNS for gastric cancer.
The method by which to administer radioisotope or dye tracer for SNNS has been a topic of debate. Traditionally, the tracer has been applied as a preoperative submucosal administration of radioisotopes or intraoperative submucosal injection of dye tracer around the primary tumor, depending on the adopted mapping method. Either of these methods is usually carried out by endoscopy. To date, two authors have used subserosal injection in their study,8,31 and another one randomly used a submucosal or subserosal injection method. 51 In another two studies, the researchers compared the efficacy of subserosal and submucosal injection of dye tracers. In a study that consisted of 121 patients, Lee et al. 24 used isosulfan blue and found no significant difference between the subserosal and submucosal administration groups, in terms of the proportion of successfully identified SLNs (92% and 94%, respectively) or in the number of SLNs determined per patient (2.5 and 2.9, respectively). Yaguchi et al. 44 administered ICG and concluded that subserosal injection of the tracer under direct vision compares well with the submucosal application by intraoperative endoscopy.
With regard to the two well-recognized outcome parameters—(1) the number of SLNs identified by using a certain type of tracer or method and (2) the proportion of patients for whom SLNs were successfully identified from the whole study population (success rate [SR])—we could not determine clear denominators that would predict the superiority of a given method. The SR ranged between 54.8% and 100%. However, when the study by Lee et al. 47 was excluded, the lowest value for SR increased to 76.3%, likely because of the fact that that study had reported the lowest rate associated with the method of isolated removal of SLNs. Of those articles reporting 100% SR, two relied on the sole use of dye tracers, one on the sole use of 99mTc tin C, and eight on the use of dye tracers combined with a second (a radiolabeled or IREE) technique. In this analysis we noted that some authors preferred reporting the number of identified SLNs, whereas others reported the number of nodes removed, probably considering that both numbers represented the same parameter. The number of SLNs identified/removed per patient ranged from 1.5 to 10.5 (Table 2). In most of the studies, however, this number was between 2 and 5. We recognized that there was no conspicuous factor that impacted the number of SLNs.
Detection of SLN metastasis
It is generally accepted that detection by frozen section of metastasis in a SLN during SNNS should lead the surgeon to proceed with conventional D2 lymph node dissection. In this context, the technique used for the detection of metastatic foci within SLNs and false negativity and accuracy rates remain the most important parameters of the SNNS concept for gastric cancer. In the vast majority of reports, the sole statistical parameter provided was the accuracy rate. In some studies,44,45,49,52 the authors have intended to specifically focus on the method of identifying SLNs and did not give detailed information about the technique used for the histological evaluation of SLNs. The issue of whether hematoxylin and eosin (H&E) staining is adequate for intraoperative detection of LN metastasis remains controversial. Because of this controversy, efforts have been directed toward making use of more reliable histopathological methods.
The perusal of the articles revealed that histological methods used to detect metastasis in LNs included H&E staining, immunohistochemical (IHC) staining and reverse transcription–polymerase chain reaction (RT-PCR) (Table 3). As expected, all of the studies relied principally on H&E as the baseline method for detecting metastasis. The great majority of studies (25 of 38 with accessible knowledge [65.8%]) have also benefited from IHC staining to confirm the status of LNs. However, the proportion of studies in which the IHC method was used during frozen section examination was only 23%. This means that the IHC method has been generally used to confirm the final pathologic staging with regard to LNs and did not drive the operational strategy. In 32 studies, the authors compared the histological examination of SLN biopsy with subsequent standard lymphadenectomy. Our results also indicate that the RT-PCR method has been examined in only three trials (7.9%).11,22,28
Accuracy (AC) was defined as the number of patients with true positive+true negative histology/whole sentinel lymph node–identified population.
Could not be accessed.
In the sentinel lymph node pick-up method, where an isolated removal of sentinel lymph nodes is carried out.
In lymphatic basin (LB) dissection, where all related lymphatic structures are removed.
For stage cT1tumors.
For stage cT2–3 tumors.
Using indocyanine green.
Using infrared ray electronic endoscopy as an adjunct to dye-guided method with indocyanine green.
H&E, hematoxylin and eosin staining; IHC, immunohistochemical staining; isolated excision, an isolated excision and examination of sentinel lymph nodes with frozen sectioning; RT-PCR, reverse transcription–polymerase chain reaction; SLN-M, method used for sentinel lymph node dissection; SM, submucosal injection; SS, subserosal injection.
It is interesting to consider that authors of such trials have found more sophisticated methods to be useful in the SLN concept, especially in terms of detecting micrometastases. Osaka et al. 22 showed that IHC staining and RT-PCR were able to detect micrometastases in 8 and 21 LNs, respectively, in 10 cases from a series consisting of 57 patients with early gastric cancer. They pointed out that none of those micrometastases could be demonstrated by conventional tissue staining either. Similarly, the series reported by Arigami et al. 28 included 61 patients with clinically node-negative cT1 and cT2 tumors; H&E determined 5 (8.2%) of the patients as having SLN metastasis, whereas IHC examination indicated that 8 (13.1%) patients actually harbored metastatic disease. This rate increased to 36.1%, with 22 patients having LN metastasis, when RT-PCR was used as the diagnostic method. It was noted that micrometastases demonstrated in 14 additional patients were responsible for the discrepant findings between the IHC and RT-PCR methods. Another interesting finding derived from the review is that all studies that compared H&E against other histopathological methods had been published before the year 2006. Reports published over the last 5 years have either relied on the sole use of the H&E method or benefited from IHC as an adjunct to H&E to confirm the diagnosis. There was no association identified between the histological method used and the method of identifying SLNs or the type of the surgical procedure.
The feasibility of SNNS depends largely upon how reliably the status of SLN can reflect the status of non-SLN involvement. The accuracy of a given method used to detect SLN metastasis ranged among studies from 72.2% to 100%. Tajima et al. 49 compared cT1 tumors with cT2–3 tumors and found that the accuracy rate was 72.2% for cT2-3 tumors and 97.2% for cT1 tumors (P<.05). The second lowest rate of accuracy (74%) was reported by Orsenigo et al. 46 Hundley et al. 8 relied on H&E as the frozen section staining method and reached an accuracy rate of 78%. Except for one study 24 in which an accuracy rate of 87.2% was achieved for submucosal injection of dye tracer (versus 89.2% for subserosal injection), all of the remaining studies have reported over 90% accuracy. Eleven articles reported 100% accuracy at predicting the true nodal status of patients by using the SLN concept. Kitagawa et al. 58 reported that accurate intraoperative diagnosis using H&E with a single slice was possible, but only in 74% of the cases. Studies have varied in the number of slices taken from each SLN (from one slice through multiple 2-mm slices), and a considerable proportion of them did not define pathologic procedures in detail. However, it can be concluded that in many of them one or two slices were cut for frozen section examination. No significant difference was detected between articles published in the early and late 2000s in terms of accurate prediction by SLN biopsy of nodal disease status.
Patient selection and surgical management
The success of SNNS in breast cancer originates principally from the fact that lymphatic flow from any quadrant of the breast to the LNs follows a relatively predictable pattern. However, lymphatic flow around the stomach has a considerably different pattern (Fig. 2). The drainage of lymphatic fluid from the stomach to regional LNs is multidirectional, rather than following a single course; this increases the chance for metastatic cells coming from the primary tumor to move into multiple SLNs. Both the number and the location of SLNs may vary. Lymphatic fluid containing tumor cells may flow toward SLNs situated anywhere along the lesser curvature (LN numbers 1, 3, and 5, according to classification by the Japanese Gastric Cancer Association 4 ) or the greater curvature (LN numbers 2, 4, and 6), depending mostly upon the location of the primary lesion. However, one should keep in mind that multiple SLNs could also exist concurrently in the lesser and greater curvatures. 55 It is also possible that the second echelon (LN numbers 7, 8, 9, and 11) accommodates whole or portions of SLNs.8,58 This complicated drainage structure has historically been considered an obstacle that has restricted, at least in part, the translation of the concept of SNNS to the surgical management of gastric cancer patients.
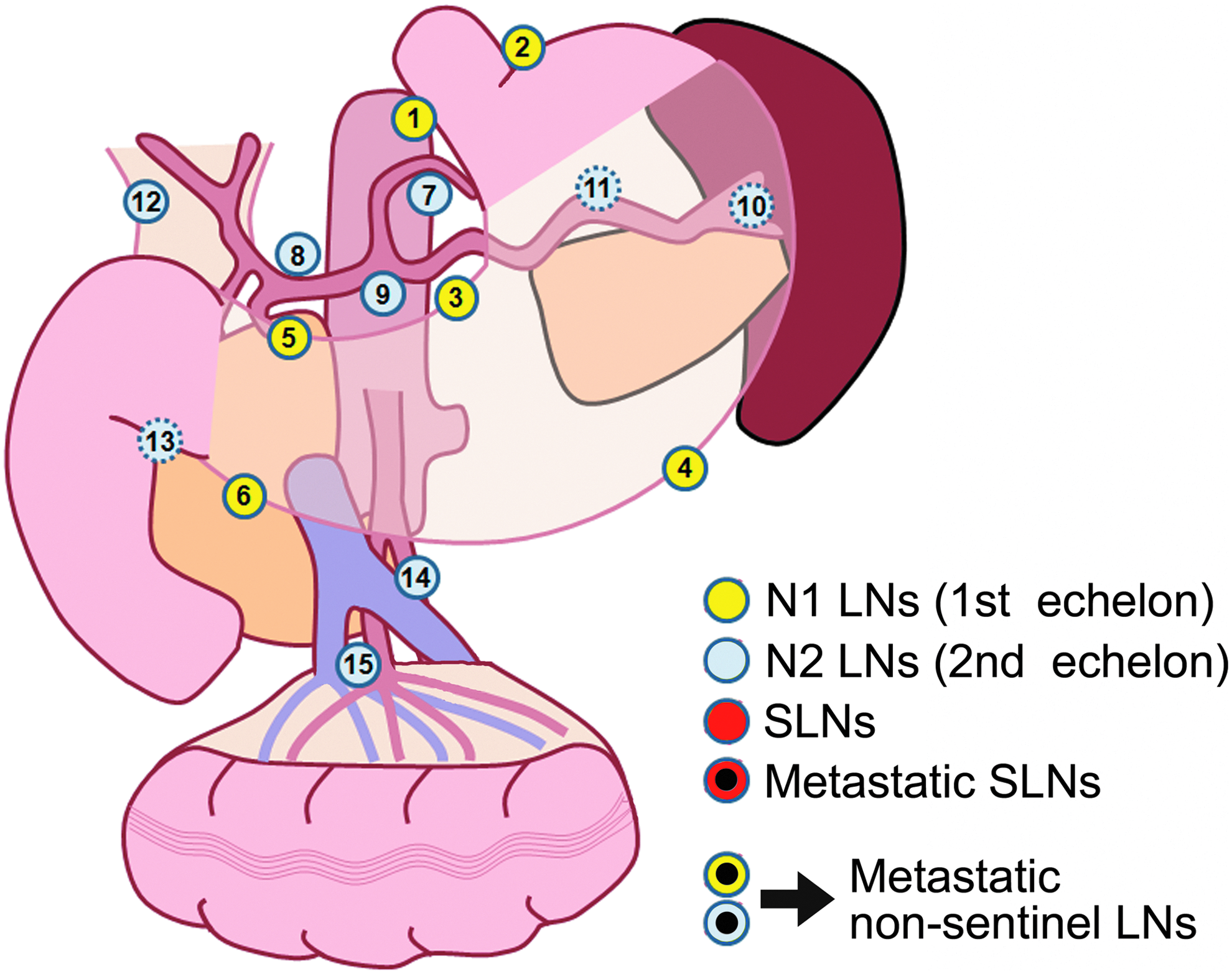
Schematic representation of lypmh nodes (LNs) relevant to the stomach according to the Japanese Classification of Gastric Carcinoma. 5 SLNs, sentinel lymph nodes.
Unlike other components of SNNS, patient selection has largely been standardized by the country where the procedure is performed. Authors of studies conducted in Japan and South Korea have recruited those patients with clinically and radiologically node-negative cT1 and cT2 (confined to the submucosa and muscular layer) disease.7,10,11,18,19,22,24,44,53,55 However, studies conducted in countries in Western regions have tended to include cT3 (infiltrating the serosa) tumors as well.8,25,27,54 This inclusion pattern demonstrates that only a certain subset of patients can be treated using the SNNS concept, ranging from as low as 3% to as high as 50% of the entire population of gastric cancer patients.2,54,57,59 The probability of LN involvement increases from roughly 10%–15% to 40% when the T stage increases from cT2 to cT3. 60 In addition to this, lymphatic skip metastasis has been associated with obstruction of lymphatic flow by tumor cells, which results in drainage through alternative lymphatic pathways. For these reasons, implementation of SNNS in the management of patients with cT3 tumors who are at increased risk of non-SLN involvement remains controversial.46,47,54 Furthermore, it has been reported that cT1 gastric cancer seemed to be a better candidate for SNNS than cT2 disease.31,49,53,58 Consideration for SNNS of cT3 tumors in Western countries appears to be linked to two facts: relatively low incidence of gastric cancer and low incidence of patients with an early T stage (5%–10% of the entire patient population), which would lead to slow patient accrual. Thus, in our opinion, only patients with clinically node-negative cT1–2 tumors should be considered as candidates for SNNS at present.
In this review study, we also recorded the surgical procedure adopted by the authors (open, laparoscopic, or both) and the technique used for LN removal (isolated excision [pick-up method] or lymphatic basin dissection) (Table 3 and Figs. 3–5). Pick-up method refers to the isolated removal of each SLN, which leaves perinodal structures in the abdomen. Lymphatic basin dissection refers to the en bloc removal of SLNs, as well as neighboring non-SLNs and lymphatic channels that drain the primary tumor site. The key objective underlying the SNNS is to protect the patient from unnecessary morbidity, which could be caused by extended lymphatic dissection. Use of SNNS can also shorten the operation time, decrease intraoperative blood loss, and hasten recovery. As these features largely overlap with the idea of minimally invasive surgery, the optimal procedure of SNNS would integrate the use of laparoscopic or other minimally invasive approaches.
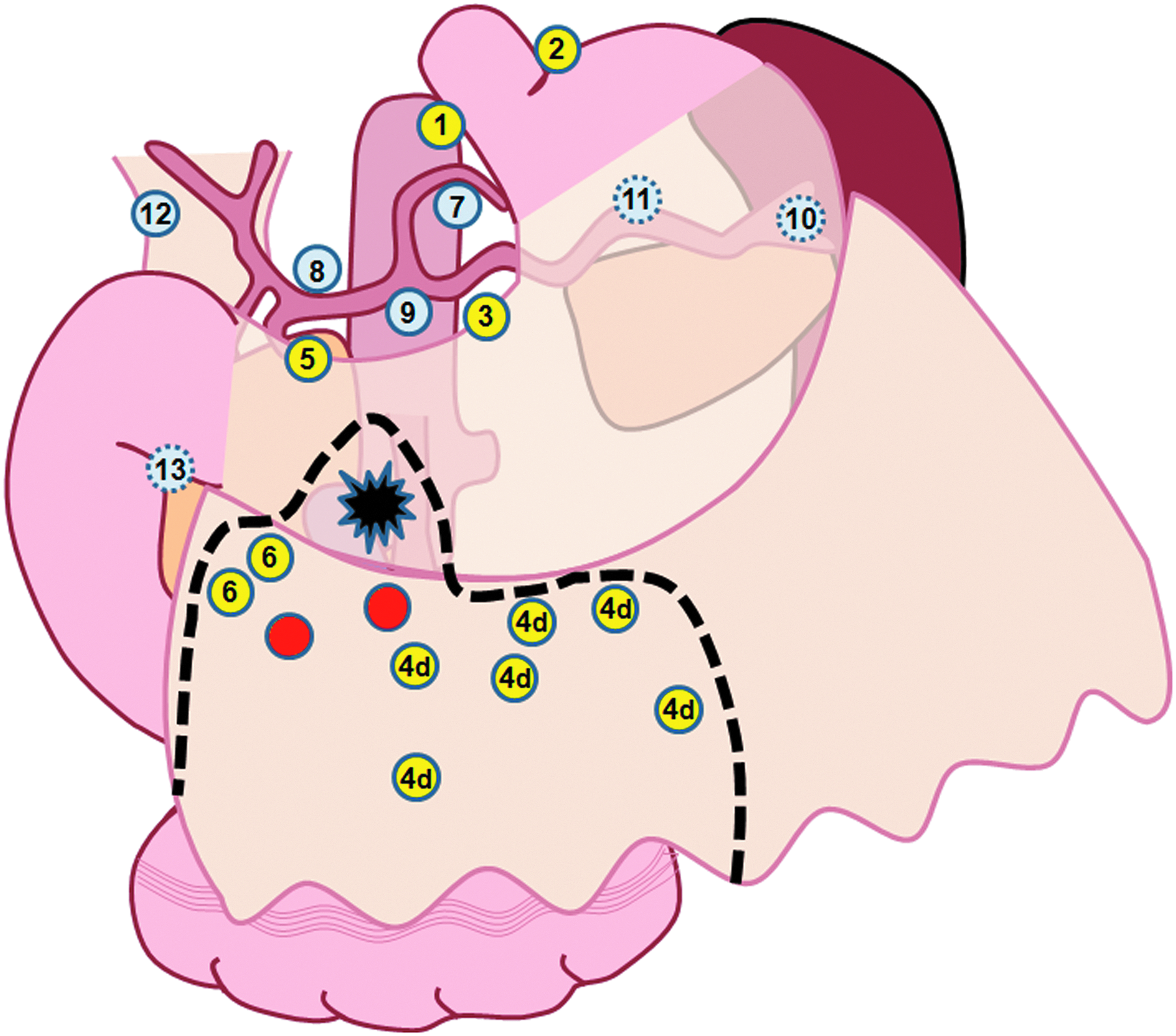
Illustration of lymphatic basin dissection. For example, for a cT1 tumor situated on the antrum, the whole lymphatic basin associated with stained/radiolabeled sentinel lymph nodes (numbers 4d and 6) is removed. The dotted line shows the excision borders.
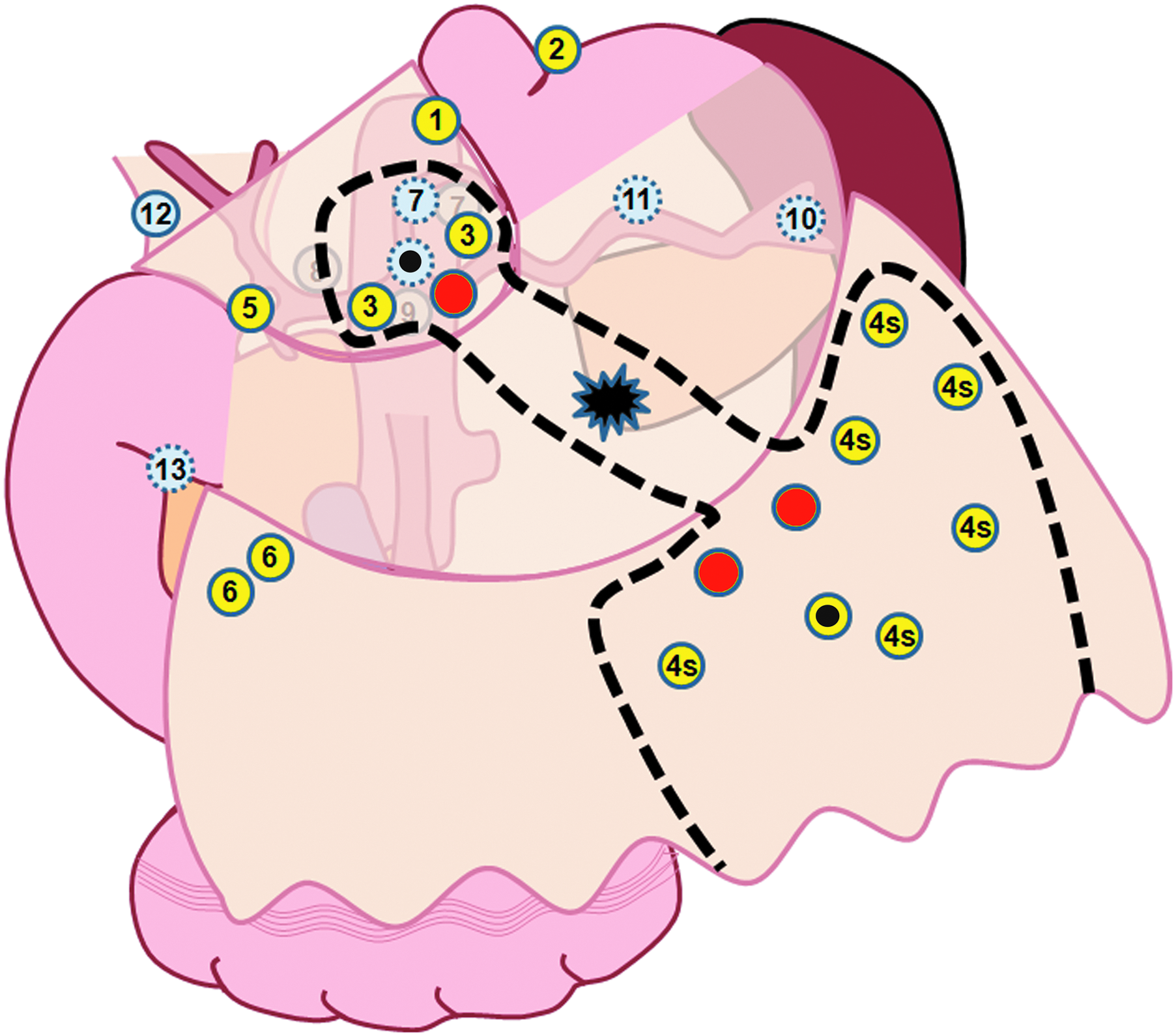
Illustration of multidirectional pattern of gastric lymphatic flow. This may result in skip metastases beyond the sentinel lymph nodes. It is also probable that the second echelon accommodates whole or portions of sentinel nodes. The dotted line indicates resection borders for lymphatic basin dissection.

Schematic representation of the pick-up method for sentinel node navigation surgery. Only stained/radiolabeled lymph nodes are removed. The dotted line demonstrates resection borders for the pick-up method.
In 14 studies, function-preserving resection was used for primary tumor removal, whereas the remainders included either standard total/distal subtotal/proximal gastrectomies or amalgamated patient groups in which both function-preserving and standard gastrectomy operations were performed. In the majority of the studies (70%) SNNS was performed via laparotomy. In 9 (21%) of those 43 studies, the authors adopted laparoscopic or laparoscopic-assisted procedures.16,21,23,34,37,42,46,47,53 The remaining four (9%) studies were constructed with amalgamated patient subsets of open and laparoscopic treatment.18,35,49,55 It is unsurprising that reports from the early 2000s show that attempts of SNNS at that time were undertaken during open surgery. However, half of the studies published since 2007 used laparoscopic resection, although some authors reported on amalgamated subsets of patients operated on using either the open or laparoscopic method. It is interesting that none of the studies compared the feasibility of SNNS between open and laparoscopic procedures. In a recent report based on an experimental study, Cahill et al. 50 claimed that SNNS could also be performed during natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and the Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]), but this has yet to be validated by other studies.
There is an obvious difference in the technique used for LN removal between the early and late 2000s. Lymphatic basin dissection was preferred in only 3 (12.5%) of 24 studies containing relevant information published before the year 2006 (inclusive)11,23,29; this ratio increased to 60% (9 of 15) when considering publications since the year 2007. One study compared the effectiveness of isolated excision and lymphatic basin dissection during laparoscopic surgery 47 and concluded that basin dissection followed by the isolated removal of SLNs on the back table helped to overcome some shortcomings of the procedure. In the remaining trials SLN biopsy was carried out via the pick-up method. The two most important advantages of lymphatic basin dissection are recognized as (1) lowering the likelihood of the “shine-through phenomenon,” where radioisotope-injected tissues neighboring the primary tumor are mistaken for SLNs by the laparoscopic probe, and (2) facilitating harvesting of non-SLNs belonging to the same lymphatic basin. This will help eliminate overlooking of a skip LN metastasis, which is generally encountered in non-SLNs located within the same lymphatic basin as the SLN. Therefore, removal of entire LNs and lymphatic ducts related to the same basin, rather than selective excision of identified SLNs, seems to be the most reliable procedure.12,46,52,58 To date, no report has stated that lymphatic basin dissection increased the risk of surgical morbidity.
Discussion and Future Perspective
Analysis of the body of literature encompassing studies of SNNS concept treatment for gastric cancer reveals that two major changes have occurred over the last 5 years in the approaches to identify SLNs. First, the general preference to visualize SLNs has shifted toward a double-tracer (dye plus isotope) method.32–34,36,40,44,47,52 Many researchers have reported substantial improvement by the combined use of both techniques in the rate of identification of SLNs,32–34,47,53,58 although some authors did not agree with that idea. 40 Hayashi et al. 10 stated that a reduction in the SR would result if either the dye-guided or radioguided method was used solely. Every method tested and reported in the article achieved only 90% success in identifying SLNs and 4%–7% of skip metastasis in the non-SLNs. The second change over the last 5 years was increased use of ICG as the dye tracer; in the previous 5-year period, isosulfan blue and patent blue violet were the two substances preferred for SNNS.29,31,35,36,49,52,55 Identification of real SLNs in a timely manner during the operative procedure is critical to achieving an acceptable SR for detecting metastasis to SLN in gastric cancer. An ideal tracer for surgical use to identify SLN would be nontoxic, cost-effective, and readily available; moreover, this substance would accumulate in the SLN within minutes and be retained for hours, without passing beyond the sentinel nodes. An ideal tracer is also expected to be easily recognized by the surgeon, without requiring any sophisticated equipment. It must also be amenable to both open and minimally invasive surgery procedures. Unfortunately, none of the commercially available tracers on the market today meets all of the aforementioned criteria. Fluorescence imaging of the lymphatic structures stained by ICG, however, can be used to visualize the dye within thin lymphatic vessels and the SLNs situated deep inside tissues that might otherwise be overlooked.45,49 IREE has emerged as a promising procedure that enhances visualization of ICG-stained tissues. Moreover, many of the novel state-of-the-art technology products show promise. For example, a combined procedure of quantum dots tracers, a well-studied group of nanoparticles, and near-infrared fluorescence technology has been shown in a porcine model to facilitate visualization of both natural anatomical structures and SLNs during surgery as overlapping images in real time.58,59,61,62 Furthermore, it has been show that quantum dots can map lymphatic channels rapidly by accumulating into the SLNs within 1–3 minutes and do not flow toward non-sentinel nodes over the next 4 hours. 62 Most recently, next-generation bimodal nanoparticles that possess features of both radioactive and dye tracers and that provide simultaneous acoustic and visual guidance have been developed. 63 ATX-S10Na(II), a novel lysosomal photosensitizer that sustains its concentration for a long period of time and is recognized as a bright red color in the lymphatic tissue, has also been investigated in animal studies for its potential as a tracer.41,43 It seems likely that in the near future these novel and next-generation nanotechnology-based tracers will replace conventional dye-guided and radioisotope-based methods for SNNS, once the issue of toxic side effects attributed to these agents is overcome.
In summary, although no clear consensus exists as to the nature of tracer or method of choice to be selected for SNNS in gastric cancer, some considerations can be drawn. The dual-mapping procedure is becoming increasingly popular. Endoscopic submucosal administration of the tracers (radioisotope, 3 hours to 1 day before surgery; dye, intraoperative) remains the procedure of choice, and ICG with fluorescent imaging is gaining its own proponents rapidly.
What should be noted specifically is that metastasis to SLN cannot be detected if a suitable method of histological examination is not used; this is regardless of how successful any particular surgeon is at identifying SLNs. The overview of the literature suggests that molecular methods, such as RT-PCR technology, give a better chance of detecting metastasis relative to conventional staining, especially in terms of micrometastases. RT-PCR technology relies on the amplification of certain mRNA primers derived from malignant cells and allows staining by monoclonal antibodies that react with several human cytokeratins. However, this method has two major drawbacks. First, many hospitals that are normally able to perform SNNS by H&E staining lack the technical equipment needed to perform this sophisticated testing. Second, obtaining results in a timely manner has been a serious challenge. It is clear that rationality of a technique for SNNS is correlated with the extent to which it does aid in intraoperative decision making. Nevertheless, evolving tools appear to help us to do what is necessary, and it has recently been possible to shorten the time (to 30 minutes) required to obtain a result from ultrarapid IHC test and from one-step nucleic acid amplification, a novel method in the family of RT-PCR.28,64 However, at present, H&E staining of multiple slices still appears to be the best available option for the majority of surgeons carrying out SNNS in their daily practice. If possible, supplementing the H&E procedure with ultrarapid IHC staining will certainly contribute to the reliability of the results. Some authors favor removal of the entire lymphatic basin corresponding to the stained and/or radiolabeled SLNs, regardless of the presence or absence of metastasis in SLNs.
Not every patient with gastric cancer is eligible for SNNS. There seems to be an obvious agreement among most authors that the current approach mandates that only tumors limited to gastric submucosa should be considered unequivocal targets of SNNS. In that same regard, lesions confined to the muscularis propria (cT2) may also be considered. However, some patients whose tumors correspond to cT2 disease by imaging will actually have cT3 disease, which may impair the reliability of the application. Although some researchers from Western countries have included patients with cT3 disease, the high likelihood of skip metastasis as a result of lymphatic blockage by tumor cells should be taken into consideration.
Laparoscopic treatment is rapidly evolving into a key strategy of the armamentarium of gastric cancer surgery, owing to recently developed novel state-of-the-art devices that facilitate both radical and partial resection of the stomach. However, the latest version of gastric cancer treatment guidelines has recommended that the laparoscopic approach should still be considered as a primarily investigational form of intervention. 5 Nonetheless, the promising revolutions in instrumentation and the ever-growing body of knowledge of these technologies and the biological processes underlying metastasis have promoted the value of laparoscopy. In our opinion, the final target of SNNS should be minimally invasive (laparoscopic or robotic) lymphatic basin dissection plus function-preserving (partial or wedge) resection of the primary tumor, providing that it is smaller than 4 cm in diameter. The issue of whether patients with primary lesion confined to the mucosa might also be viable candidates for endoscopic mucosal resection with SLN biopsy is currently under investigation, and preliminary reports have shown encouraging outcomes.65,66 It seems feasible, then, to suggest performing partial or total gastrectomy with standard LN dissection in more advanced disease, depending on the lesion location.
In conclusion, recent developments in minimally invasive interventions and SNNS have notably affected the current approaches to gastric cancer surgery. Cumulative data on the utility and outcomes of this approach have been generally derived from single-institute experiences. Although conventional dye tracers, such as patent blue violet and isosulfan blue, are still in use, ICG has attracted more attention over the last years. The combined use of dye and radioisotope tracers (double-tracer method) appears to be a superior approach for identifying true sentinel nodes. Infrared ray electronic endoscopy, florescence imaging, near-infrared light, and nanoparticles seem to dominate the future SNNS concept. Histological detection of metastasis across the world is still mainly accomplished by H&E staining; however, IHC staining and RT-PCR have potential for routine use in clinical practice but remain limited by the affiliated ultrarapid processing systems that have yet to become available in many countries. We believe that minimally invasive function-preserving resection of the stomach with lymphatic basin dissection navigated by SLN identification would represent the current dominant choice of SNNS for early gastric cancer. Patients with cT3 or more advanced disease are still advised to receive standard D2 dissection, as it yields satisfactory survival rates.
Footnotes
Disclosure Statement
No competing financial interests exist.