
Abstract
Abstract
Background:
Efficient retraction of the left lobe of the liver is mandatory for laparoscopic gastric surgery because of the lesser curvature of the stomach, the gastroesophageal junction, and the gastrohepatic ligaments that are covered by the left lobe. We attempted to introduce our simple and safe method for lifting up the liver by suturing the pars condensa and the right diaphragmatic crus at the same time.
Study Design:
Between March 2011 and February 2012, 85 patients (52 men and 33 women) underwent laparoscopic gastrectomy for gastric cancer using our liver retraction method. Our procedure included combined suturing of the pars condensa and the right crus and retrieval of the thread on both sides of the xiphoid process. The end result is a triangle-shaped sling with the left lobe sitting on it.
Results:
There were 65 totally laparoscopic distal gastrectomy, 18 totally laparoscopic total gastrectomy, and two laparoscopy-assisted distal gastrectomy cases. The mean patient age was 58.7 years (range, 28–82 years), and average body mass index was 24.5 kg/m2 (range, 16.7–32.0 kg/m2). In all cases, we acquired adequate exposure of the surgical field without the help of another instrument, and there were no procedure-related complications such as hepatic laceration, bleeding, or bile leakage.
Conclusions:
Our liver retraction method is a simple, safe, and effective procedure for laparoscopy-assisted gastrectomy as well as totally laparoscopic gastrectomy. It can be also useful in other types of laparoscopic gastric surgery.
Introduction
Patients and Methods
We have used this technique for patients undergoing any laparoscopic gastrectomy, including laparoscopy-assisted distal gastrectomy (LADG), totally laparoscopic distal gastrectomy (TLDG), and totally laparoscopic total gastrectomy (TLTG), performed for early gastric cancer at the Asan Medical Center, Seoul, Korea.
Under general anesthesia, the patient is placed in the supine position with the right arm abducted. After the patient has been prepped, a 12-mm infraumbilical camera port is inserted using an open technique, and carbon dioxide pneumoperitoneum is then created. A diagnostic exploration is then performed using a 30° scope to determine how to proceed with the laparoscopic gastrectomy. Four additional trocars are used: one 5-mm trocar on each of the upper quadrants and one 12-mm trocar on each of the lower quadrants of the abdomen for manipulation. An operator is stationed on the right side of the patient.
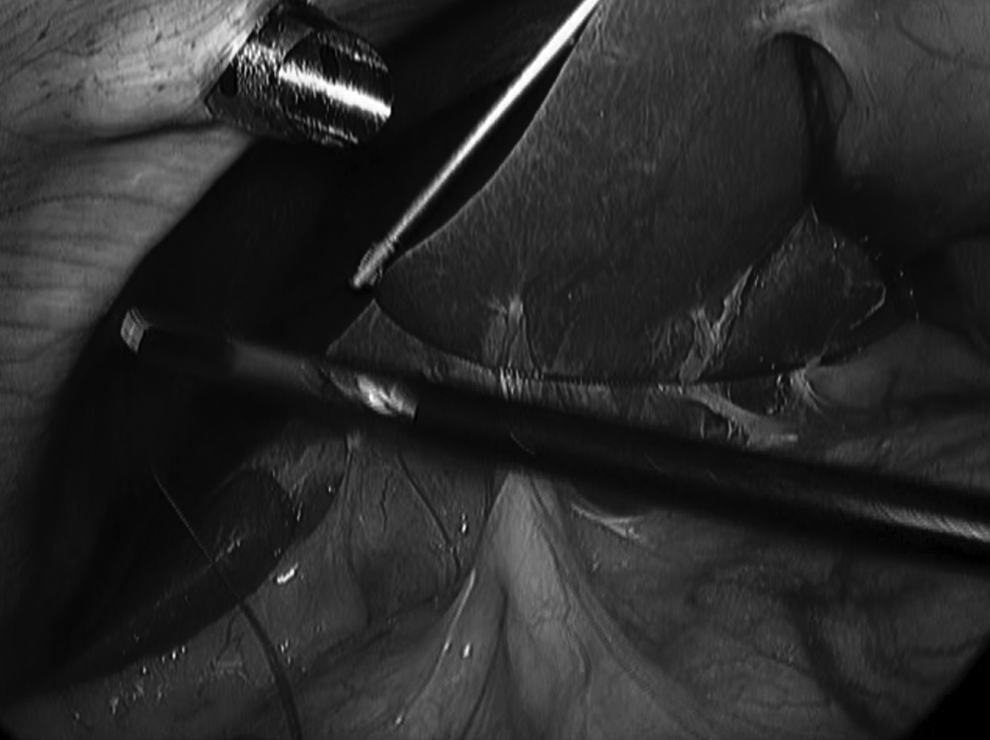
In the reverse Trendelenburg position, surgery commences with division of the gastrohepatic ligament until the gastroesophageal junction and a right diaphragmatic crus are uncovered using a Harmonic® scalpel (Ethicon Endo-Surgery Inc., Cincinnati, OH). The operator then loads a Polysorb™ 1-0 suture (Covidien Inc., Santo Domingo, Dominican Republic) into the peritoneal cavity through the 12-mm right lower quadrant trocar and simultaneously stitches up the right crus and the pars condensa (Fig. 1). The sutured needle and thread are then taken out of the abdominal cavity through the right lower quadrant trocar again, and the needle is removed.

Suture being driven through the right diaphragmatic crus and the pars condensa.
To retrieve the thread in the peritoneal cavity, we use a suture-passer, the Endo Close™ trocar site (Covidien Inc., Norwalk, CT), and puncture wounds are created on both sides of the xiphoid process. First, the surgeon pierces the suture-passer on the left side of the xiphoid process, and one end of the sutured thread is taken back from the peritoneal cavity. In the same manner, the other end is retrieved at the right side without puncturing the falciform ligament (Fig. 2). The distance between the two sites is recommended to be at least 3 cm. Both ends are then tied over the skin in order to lift the left lobe. The end result is a triangle-shaped sling and the left lobe sitting on it (Fig. 3). When finishing the surgery, we cut down the thread using an endo-scissor or Harmonic scalpel near the pars condensa so as to prevent potential laceration of the liver by the thread.
One end of the thread is retrieved from the peritoneal cavity by means of a suture-passer.

Suture retraction of the left lobe of the liver.
Results
Between March 2011 and February 2012, 85 patients (52 men and 33 women) underwent laparoscopic gastrectomy for gastric cancer using our liver retraction method. There were 65 TLDG, 18 TLTG, and 2 LADG cases. The mean patient age was 58.7 years (range, 28–82 years), and the average body mass index was 24.5 kg/m2 (range, 16.7–32.0 kg/m2). In all cases, we acquired adequate exposure of the surgical field without any help of another instrument, and the mean time required to complete the procedure was less than 4 minutes. There were no procedure-related complications such as hepatic laceration, bleeding, or bile leakage.
Discussion
Liver retraction is also essential for other types of laparoscopic gastric surgery such as gastric band placement or fundoplication as well as for laparoscopic gastrectomy. To create an efficient surgical field, several mechanical retractors have been used. Shibao et al. 4 reported a disk suspension method that included a snake retractor and elastic band fixation with a silicon disk. Although these retractors provide effective liver retraction, there are some limitations regarding retractor-associated techniques. They basically require that an assistant holds the retractor in one hand and thus result in the restriction of assistance or the operating space, and the operator will have to use an additional trocar in the upper abdomen.
Therefore, more innovative techniques have been devised in order to overcome these problems. Lee et al. 5 proposed liver elevation using a suture that pierces the edge of the left lateral section of the liver and is fixed to the abdominal wall. Although they reported that their procedure was safe, the study was performed in only 6 patients, and it is possible that bleeding may disturb the procedure. Moreover, despite of invasiveness of the procedure, their surgical field was not superior to ours. Sakaguchi et al. 6 reported a method using a Penrose drain and a J-shaped retractor (Endo Retract Maxi™; United States Surgical Corporation, Norwalk). This method provides a favorable surgical field but requires dissection around the coronary ligament and has a relatively long procedure time of 10 minutes. Moreover, an additional instrument is required.
de la Torre et al. 7 described a suture liver-lifting technique during adjustable gastric band placement in which they anchored a suture across the right diaphragmatic crus. However, in patients with a high body mass index, as the left lobe is relatively large and heavy, a retracting suture or crus may be torn. Moreover, effective retraction of a falciform ligament and the left medial section of the liver is important to dissect lymph node basins around the right gastric artery, the common hepatic artery, and the celiac axis. However, as their method is not effective for lifting up the falciform ligament and left medial section, it may thus be insufficient for successful laparoscopic gastrectomy for gastric cancer.
Shabbir et al. 8 suggested a suture retraction technique similar to ours in that the suturing is performed through the pars condensa and exteriorized by means of a suture-passer. However, our methods have several advantages over theirs. First, we place two puncture wounds on both sides of the xiphoid process and not in the subxiphoid space. As these authors indicated, their technique is limited to patients undergoing TLTG and is not indicated for those receiving LADG or laparoscopic-assisted total gastrectomy because a puncture wound is located on the mini-laparotomy line. However, our puncture sites are not affected by mini-laparotomy, and liver retraction can be maintained after opening the abdominal wound (Fig. 4). Therefore, our technique can be useful in LADG or laparoscopic-assisted total gastrectomy as well as in TLDG and TLTG without any help of another instrument. Second, by suturing together the pars condensa and the right diaphragmatic crus, the suture can bear the left lobe regardless of its size or weight. It is also easier to dissect the esophagus or hiatus because an anchoring suture may widen the plane between the esophagus and the right crus. Third, as we do not directly pierce the falciform ligament or liver, our procedure can be safely performed in patients with liver cirrhosis having prominent varices.
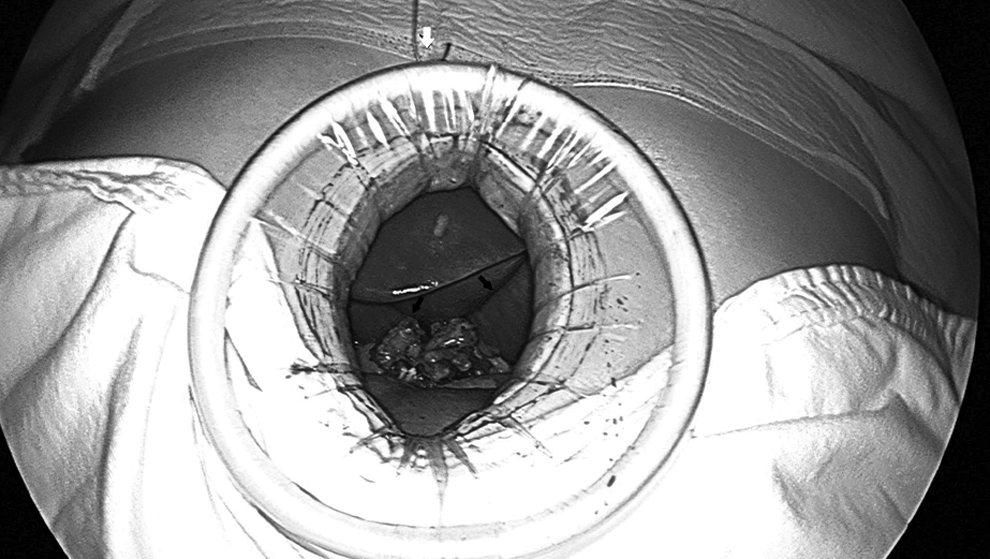
Suture retraction of the liver is maintained after incision of the mini-laparotomy in laparoscopy-assisted distal gastrectomy. Black arrows indicate a sutured thread retracting the liver in the peritoneal cavity; the white arrow indicates a thread tied over the skin.
In conclusion, our liver retraction method is a simple, safe, and effective method for acquiring an adequate surgical field around the gastrohepatic ligament, the hepaticoduodenal ligament, and the gastroesophageal junction. Best of all, our technique is unprecedented as it can be used for all types of laparoscopic gastric surgery.
Footnotes
Acknowledgments
We thank Mr. Chang-Geun Heo and Chun-Myoung Ji for help with this article.
Disclosure Statement
No competing financial interests exist.