
Abstract
Abstract
Background:
Cure of disease with the least possible injury is an ideal of surgery. Herein we share our experience with transumbilical single-incision laparoscopic multiple organ procedures using conventional instruments.
Subjects and Methods:
We reviewed data from 20 patients who underwent transumbilical single-incision laparoscopic surgery of multiple organs between May 2009 and March 2012 at Shengjing Hospital. All 20 patients had laparoscopic cholecystectomy, which was combined with appendectomy in 16 patients, resection of hepatic hemangiomas in 2 patients, and partial gastrectomy for gastric mesenchymal tumor in 2 patients. All procedures were successful with conventional laparoscopic instruments placed through a single operating portal of entry created within the umbilicus.
Results:
All the operations were successfully completed without conversion to conventional laparoscopic or open surgery. No intraoperative complications occurred. Patients were satisfied with the therapeutic and cosmetic outcomes.
Conclusions:
Transumbilical single-incision laparoscopic combined procedures appear to be a technically feasible alternative to standard laparoscopic procedures in simultaneous management of two different coexisting pathologies. Larger studies are required to confirm these findings.
Introduction
It is not uncommon for a patient to have coexisting pathologies at different sites. While a surgeon may be confronted with the embarrassment of elongating or even making another incision while performing open surgery in such a case, a simple “trocar-adding” may well solve the problem in laparoscopy. However, surgeons are now seeking to further this advantage by decreasing the number of trocars and avoiding visible scarring.
Single-incision laparoscopic surgery (SILS) has come into being on the basis of this notion. This technique is well described in the literature for appendectomy, nephrectomy, adrenalectomy, cholecystectomy, and colectomy. But, there are only a few reports of transumbilical single-incision laparoscopic combined procedures. Since beginning in May 2009, we have performed over 1000 transumbilical single-incision cholecystectomies, 20 of which were combined with other laparoscopic procedures using conventional instruments. We herein describe detailed operative techniques and challenges encountered during these procedures.
Subjects and Methods
Patients
Between May 2009 and March 2012, 20 patients underwent transumbilical single-incision laparoscopic multiple organ procedures at Shengjing Hospital, including 7 male and 13 female patients ranging in age from 40 to 74 years old and with an average body mass index of 26.6 kg/m2. All patients had a history of chronic calculus cholecystitis, among them coexistent chronic appendicitis in 16, hepatic hemangiomas in 2, and gastric mesenchymal tumor in 2 patients. Computed tomography scan was performed on all 20 patients. The diagnoses of chronic appendicitis were made when the patient had a history of acute appendicitis or repeated right lower quadrant abdominal pain and an enlarged appendix was found on computed tomography scan. The hemangiomas were located in the left lateral lobe with a diameter of less than 6 cm. The diameters of the gastric mesenchymal tumors were 3 and 4 cm, respectively; both of them were situated in the greater curvature and not near to either the cardia or the pylorus. All the diagnoses were confirmed by postoperative pathologic examination. Operative procedures performed together with SILS cholecystectomy included appendectomies, hepatic hemagioma resection, and partial gastrectomy. All procedures were performed laparoscopically using conventional laparoscopic instruments placed via a single operating portal within the umbilicus.
Operative Technique
General anesthesia was used in all cases. Pneumoperitoneum was created with the closed method using a Veress needle, and insufflation pressure was maintained at 13 mm Hg. A 2-cm intra-umbilical incision was made for trocar access, and a 10-mm trocar was inserted at the lower border of the umbilical incision for the camera port. Two 5-mm trocars were added through separate fascial openings superior to the initial trocar—with one on the incision midline and the other right lateral to it. As a result, all three trocars were introduced through the same incision at different fascial sites; entry sites were approximately 10 mm apart in a reverse triangular arrangement. A 30° 10-mm rigid laparoscope (Stryker Endoscopy, San Jose, CA) was used throughout the procedures. The patient was first positioned in a reverse Trendelenburg position with a 15° left tilt.
Transumbilical single-incision laparoscopic cholecystectomy and appendectomy
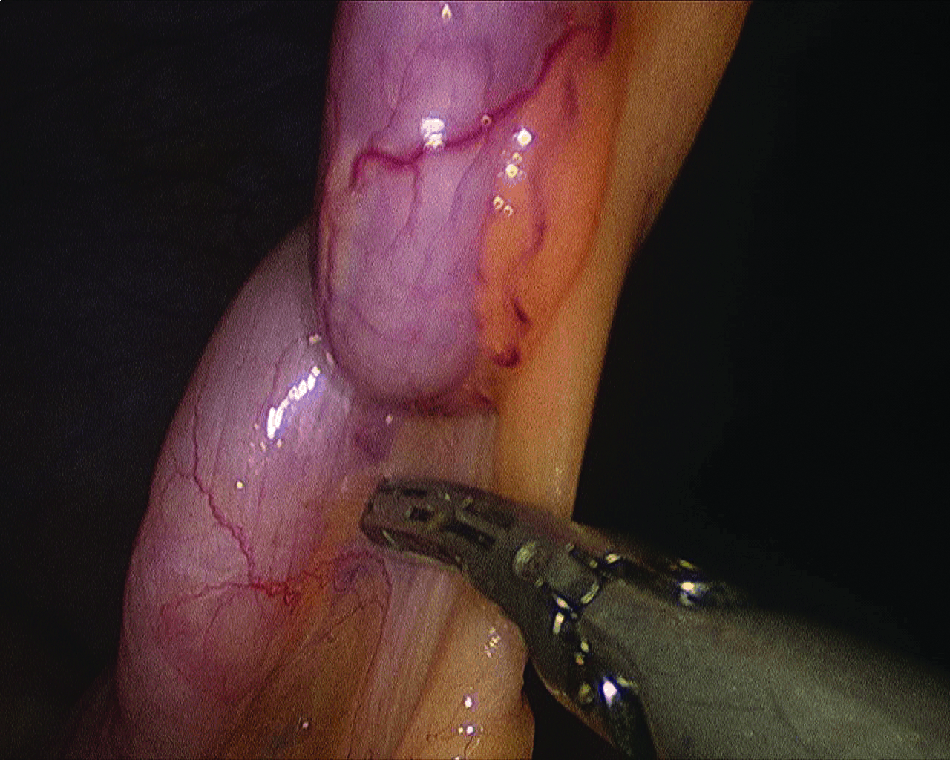
We began our procedure with cholecystectomy in a retrograde fashion as to gain a better visualization and operational convenience (Fig. 1). The gallbladder was dissected to the cystic duct, which was then ligated using two clips. It was then amputated using a Harmonic® scalpel (Ethicon Endo-Surgery, Inc., Blue Ash, OH), leaving the resected specimen in the right hepatorenal recess before removing it. The patient was then repositioned in the Trendelenburg position with a further left tilt to 25°. The appendix was located, and the cecum was adequately mobilized. The mesoappendix was dissected using a Harmonic scalpel to the base of the appendix (Fig. 2). Thereafter the appendix was ligated using clips (if the appendix measured less than 10 mm in diameter) or a silk ligature in the case of a very large appendix. The appendix was then amputated, and the specimen of both appendix and gallbladder was delivered out of the body in a specimen bag.

Retract the gallbladder toward the left axilla by a rigid grasper and use a Harmonic scalpel to dissect the gallbladder along the liver bed.
The mesoappendix and vessels were divided serially with a Harmonic scalpel.
Transumbilical single-incision laparoscopic cholecystectomy combined with laparoscopic hepatic hemangioma resection
Pneumoperitoneum was established, and three trocars were accommodated within a 3-cm intra-umbilical incision in an inverted equilateral triangular configuration at least 1 cm apart as described above. Conventional instruments were used, including 5-mm and 10-mm standard trocars (one each) and an unbladed trocar (Xcel B12LT; Ethicon Endo-Surgery). Cholecystectomy was performed as above, after which the Pringle maneuver was performed to reduce portal blood flow. The hemangioma together with a margin of normal liver parenchyma was dissected with a Harmonic scalpel and Ligasure™ (Covidien, Mansfield, MA) (Fig. 3), and major vessels or bile ducts were ligated with the endoclip. The resected hemangioma specimen was placed in a specimen bag, brought to the abdominal wall, crushed, and extracted using oval clamps via the umbilical incision. The gallbladder was extracted thereafter.
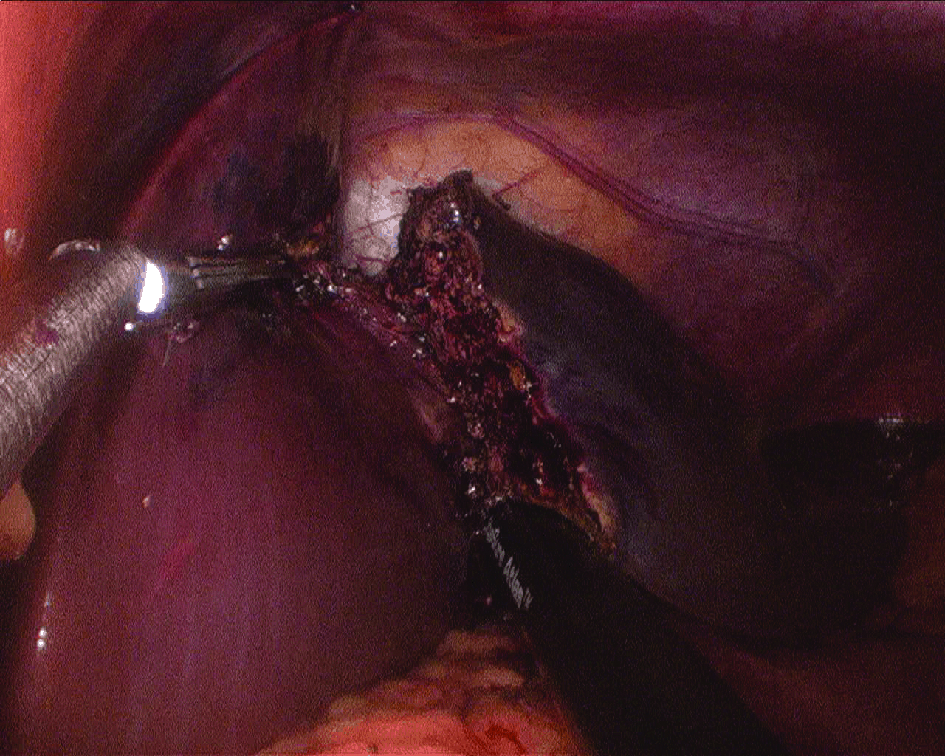
The hemangioma was meticulously dissected with LigaSure along the liver parenchyma.
Transumbilical single-incision laparoscopic cholecystectomy and partial gastrectomy for gastric mesenchymal tumor
The single-incision access and reverse triangular trocar arrangement were made as described for the resection of hepatic hemangioma (Fig. 4). The patient was positioned in a modified lithotomy position, 15–20° head-up tilt, with the surgeon standing between the legs of the patient. Cholecystectomy was performed in a retrograde fashion. The gastric tumor was identified on the greater gastric curvature by preoperative endoscopic injection of methylthioninium chloride on its base. The gastrocolic ligament was divided using the Harmonic scalpel. A laparoscopic intracorporeal linear stapler-cutting device was used to resect the lesion parallel with the long axis of the stomach, in effect performing a limited sleeve gastrectomy and avoiding the need for anastomosis (Fig. 5). The gastric specimen was placed in a specimen bag and removed though an enlarged 2–3-cm incision made between two fascial openings. The gallbladder was extracted thereafter.

The reverse triangular trocar arrangement.
Pull on the suture and transect the stomach using a 45-mm endoscopic linear stapler.
Results
All the procedures were successfully completed without conversion to conventional laparoscopic or open surgery. The operations lasted from 30 to 160 minutes, with blood loss of 5–800 mL. No intraoperative complications occurred. All the patients regained normal bowel function on postoperative Day 2 or 3. The abdominal cavity drainage was removed on postoperative Day 2–4. Patients were satisfied with the therapeutic and cosmetic outcomes. The follow-up period for all the patients was 3–30 months; to date, no significant complication has been reported (Table 1).
Discussion
Laparoscopic surgery has dramatically changed the philosophy of surgery over the past 20 years. As technology and instrumentation continue to improve, current efforts of minimally invasive surgery are aimed at reducing the number and size of trocars or eventually at obtaining “no scar” surgery. To this end, two recent innovations are being developed: natural orifice translumenal endoscopic surgery (NOTES) and transumbilical SILS. Although NOTES still remains in its infancy at present, SILS, which was inspired by the idea of totally incision-less surgery, has made its initial forays into clinical minimally invasive surgery.2,3
SILS has the advantage of a lower complexity for clinical application and the allowance of using conventional laparoscopic instruments, which promotes its current widespread use. It has been described in the literature for the treatment of various conditions.4–9 Since the beginning of application of SILS at our institution in May 2009, we have performed over 1000 transumbilical single-incision laparoscopic cholecystectomies. During this period, some patients had both cholecystitis and concomitant appendicitis, hepatic hemangioma, or gastric mesenchymal tumor, coexisting diseased that should and could be treated at the same time. In this regard, we made an attempt to perform transumbilical single-incision laparoscopic combined procedures.
The results of this study have shown that laparoscopic combined procedures can be done using commercially available instruments through a single umbilical incision. It appears to provide outcomes similar to those of standard laparoscopic surgery with fewer incisions and a well-concealed scar. Other potential benefits over conventional laparoscopy include less incision pain with lower postoperative narcotic requirements, shorter hospital stays, faster return to work and normal presurgery lifestyle, improved cosmesis, and ultimately higher patient satisfaction. What is more, SILS may use conventional laparoscopic instrumentation, which makes technical adaptation and mainstream acceptance more likely.
Of course, SILS is not entirely without its flaws. The major drawback to such a surgical approach is that the concept of “triangulation” to which laparoscopic surgeons have grown accustomed in terms of both the instruments and scope is compromised. All instruments are closely packed together, and clashing between them is common, which poses a major handicap to operating and exposure. It is technically more challenging and time consuming than conventional laparoscopic surgery, especially when the procedure is complex. As shown in Table 1, the operative time of single-incision laparoscopic cholecystectomy and appendectomy is comparable to that of conventional laparoscopic surgery (data not shown), with a trend of reduction in time. But, when it comes to resections of hepatic hemangioma and partial gastrectomy, the time is significantly longer.
In conclusion, transumbilical single-incision laparoscopic combined procedures appear to be a technically feasible and can be performed with conventional laparoscopic instruments. However, increased operative time and technical difficulty are the main concern with this technique. Our study enrolled a limited number of patients, and larger studies are required to confirm these findings and determine the true benefits of SILS combined procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.