
Abstract
Abstract
Background:
Pancreatic anastomotic leakage is a common problem after pancreaticoduodenectomy and is a leading cause of postoperative morbidity and mortality. It is important to establish a safe and simple technique of pancreatic–enteric anastomosis to minimize pancreatic leakage.
Patients and Methods:
From July 2009 to February 2012, a new method of mesh-reinforced pancreaticogastrostomy was performed in 13 patients after completion of the pancreaticoduodenal resection. Patient demographic data, pathology of lesions, operative parameters, and postoperative outcomes were analyzed.
Results:
The mean operative time was 6.9 hours (range, 5–11 hours), and the mean time for pancreaticogastrostomy was 25 minutes (range, 22–35 minutes). Intraoperative tests showed all pancreatic anastomoses were watertight. There was no postoperative death. No patient developed clinically significant pancreatic leakage (grade B or C) after operation; 1 patient (7.7%) was recognized to have a grade A pancreatic leakage. No significant complication (hemorrhage, intra-abdominal abscess, or cholangitis) was observed. The mean postoperative hospital stay was 20 days (range, 11–30 days). After discharge, all patients recovered well in the 4-week follow-up period without emergency room visit or re-admission.
Conclusions:
The mesh-reinforced pancreaticogastrostomy provides a new way to perform pancreatic–enteric drainage after pancreaticoduodenectomy and has the advantages of simplicity, ease of handling, and applicability to all types of pancreatic remnants.
Introduction
Previously, we introduced a technique of polypropylene mesh-reinforced end-to-end pancreaticojejunostomy that is safe as well as simple and is particularly preferred for patients who have soft pancreatic parenchyma. 4 Nevertheless, the mesh-reinforced pancreaticojejunostomy has potential disadvantages. When the jejunum is not wide enough to accommodate the pancreatic neck, end-to-end anastomosis is not the optimal choice. In addition, postoperative hemorrhage from the pancreatic stump might occur, and this is extremely difficult to deal with after pancreaticojejunostomy. In the interest of solving these hindrances, we designed a new pattern of pancreaticogastrostomy using a mesh-reinforcement technique—by which the pancreatic remnant wrapped in a mesh strip is embedded into the stomach and bound to its posterior wall by a single layer of continuous sutures.
Patients and Methods
Patient characteristics
From July 2009 to February 2012, mesh-reinforced pancreaticogastrostomy was performed in 13 patients after completion of the pancreaticoduodenal resection. The current series of patients comprised 6 male and 7 female patients ranging in age from 16 to 76 years (mean, 58.2 years). Five patients had pancreatic head malignancy, 6 had periampullary malignancy (3 ampullar carcinoma, 2 papillary carcinoma, and 1 distal bile duct carcinoma), 1 had a pancreatic intraductal papillary mucinous neoplasm, and 1 had pancreatic fibromatosis.
In our series, 10 patients had soft and 3 had hard pancreatic parenchyma. A dilated pancreatic duct was observed in 2 patients who had hard parenchyma.
The present study was approved by the Committee of Ethics of Sir Run Run Shaw Hospital of Zhejiang University, Hangzhou, China. All patients signed a written informed consent with the potential surgical risks. The same surgical team was responsible for all procedures in the study.
Surgical techniques
After the pancreas was severed on the scheduled line, hemostasis of the cut surface was done by electric coagulation or suture ligatures. The main pancreatic duct was identified, and a stent tube was inserted. The remnant of the pancreas was isolated for a distance of 2–3 cm and tightly wrapped in a mesh strip (1.0 cm wide) at about 1.0 cm from the cut edge. The mesh strip was fixed onto the pancreas with a few stitches (Fig. 1). Two types of mesh materials were applied, with nonabsorbable polypropylene mesh (Ethicon, Somerville, NJe) used in 6 cases and absorbable Biodesign® mesh (Cook, Limerick, Ireland) in 7 cases.
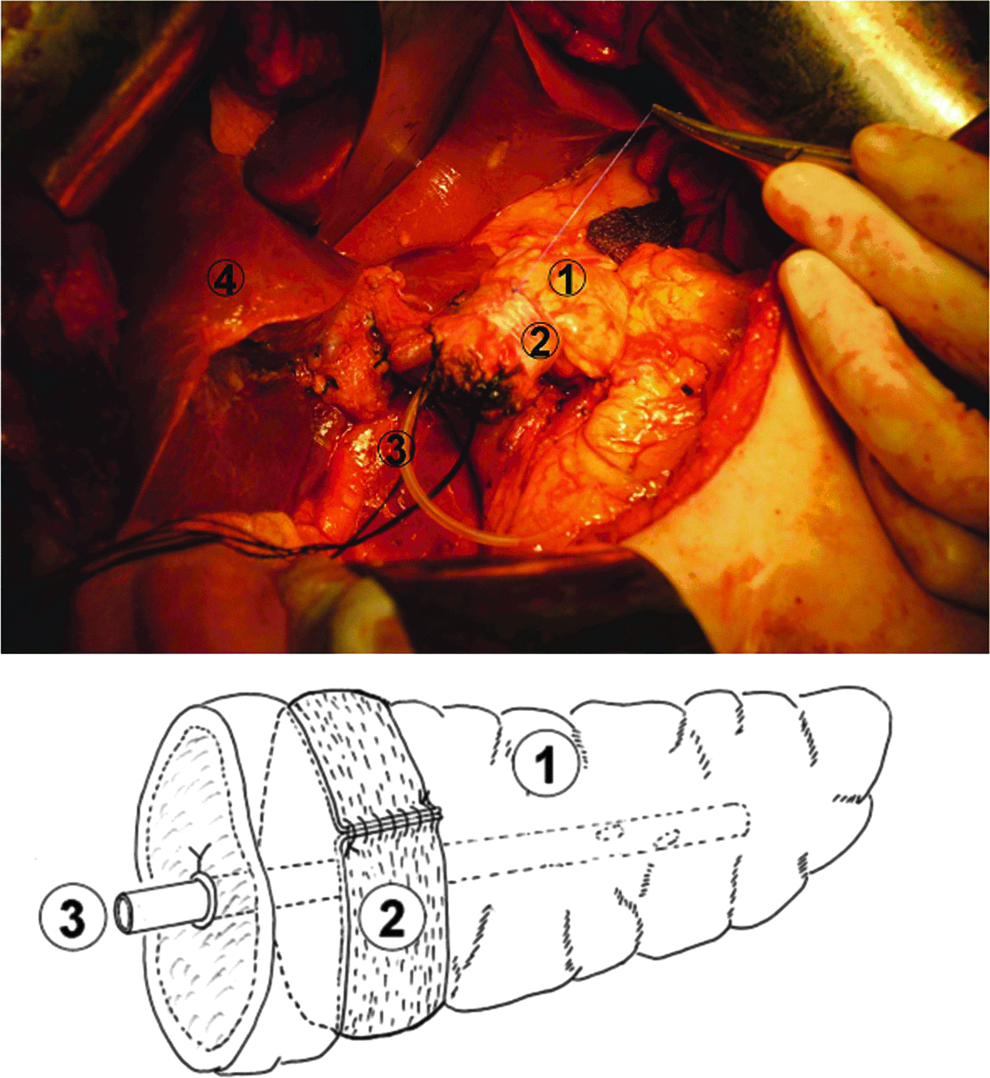
The remnant of the pancreas was tightly wrapped with a mesh strip. A stent tube was inserted into the pancreatic duct and fixed (① pancreas, ② mesh strip, ③ stent tube, ④ liver).
An incision was made on the posterior gastric wall midway between the lesser and greater curvatures, at least 6 cm proximal to the distal gastric staple line. The size of the gastrotomy was set to accommodate the pancreatic remnant. Anastomosis was begun between the anterior lip of the pancreatic stump and the proximal edge of the gastrotomy. Continuous running sutures using 3-0 Prolene™ (Ethicon) were performed. The sutures passed through the inner part of the mesh, the pancreatic capsule, and the full thickness of the gastric wall (Fig. 2). The running sutures were tightened after all of the anterior stitches were completed, thus embedding the pancreatic stump in the gastric cavity. The continuous sutures were subsequently extended to bind the posterior lip of the pancreatic stump and the distal edge of the gastrotomy using the same stitching rule (Fig. 3). Care was taken to cover all parts of the mesh in the gastric lumen. Saline solution was injected from the nasogastric tube to test for a watertight closure of the anastomosis.

Continuous running sutures were made between the inner part of the mesh and the proximal edge of the gastrotomy (① pancreas, ② mesh strip, ③ stent tube, ④ the posterior wall of the stomach).
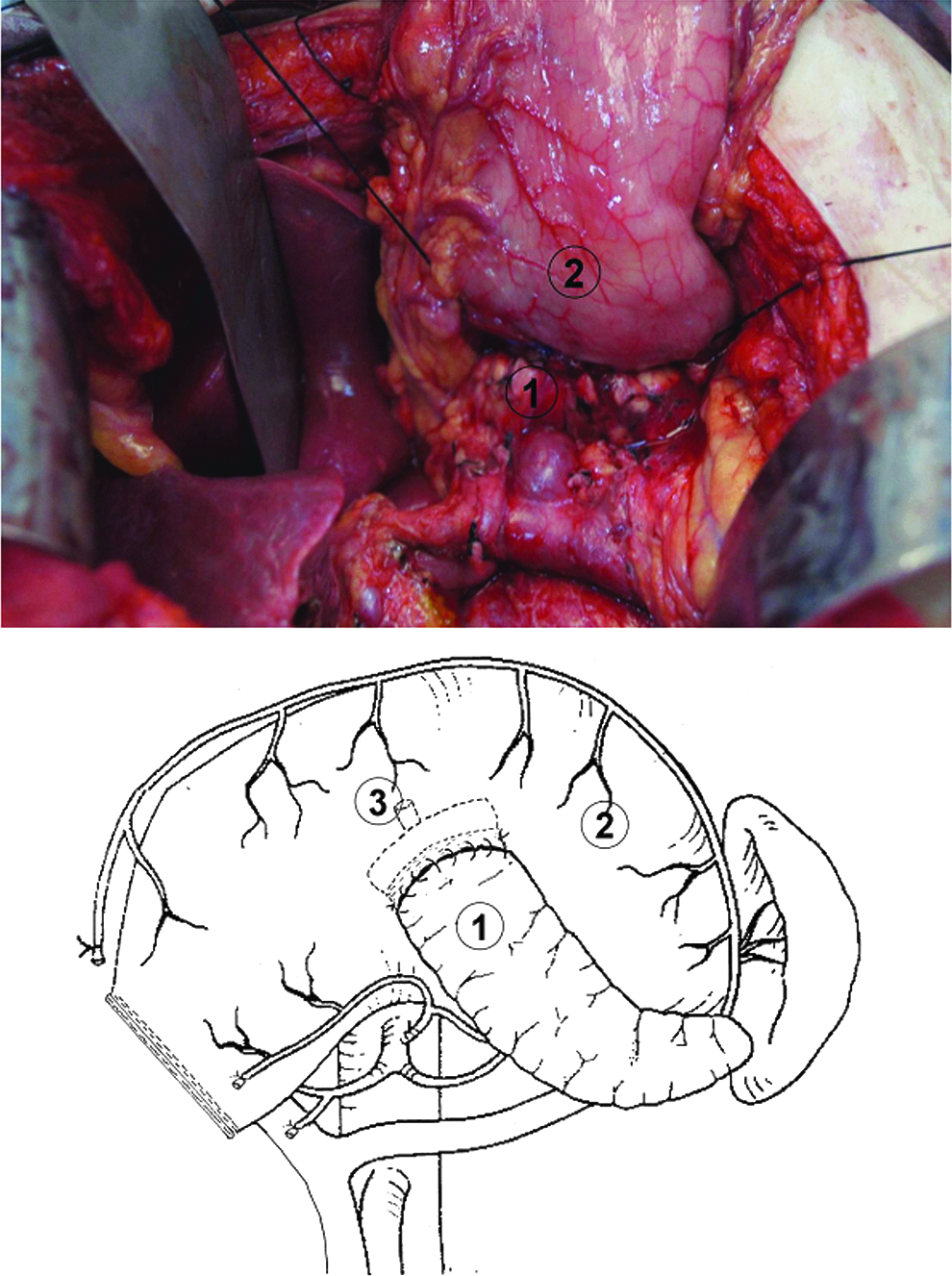
The continuous sutures were extended to bind the posterior lip of the pancreatic stump and the distal edge of the gastrotomy (① pancreas, ② the posterior wall of the stomach, ③ stent tube).
An end-to-side hepaticojejunostomy was performed to the proximal part of the jejunum followed by a standard gastroenterostomy 30 cm downstream. A Jackson–Pratt drainage tube was placed in the vicinity of the pancreaticogastrostomy.
Prophylactic octreotide was not used in this study.
Follow-up
The volume and amylase content of the drainage fluid were measured every day postoperatively. The incidence and severity of pancreatic leak were determined according to the International Study Group on Pancreatic Fistula definition. 5 All of the patients were closely followed up for a period of at least 4 weeks after discharge.
Results
The mean operative time was 6.9 hours (range, 5–11 hours), and the mean time required for pancreaticogastrostomy was 25 minutes (range, 22–35 minutes). Intraoperative tests showed all pancreatic anastomoses were watertight.
There was no postoperative death. One patient was recognized to have high amylase content in the peripancreatic peritoneal drainage 7 days postoperatively but without clinical consequence (grade A pancreatic leak). No patient developed grade B or grade C pancreatic leak. Complications of hemorrhage, intra-abdominal abscess, or cholangitis were not observed. The postoperative hospital stay was 11–30 days (mean, 20 days). After discharge, all patients recovered well in the 4-week follow-up period without an emergency room visit or re-admission.
Discussion
Pancreatic leakage remains a major cause of morbidity after pancreaticoduodenectomy. Various preventive measures have been proposed, including methods to decrease pancreatic secretion (using octreotide and its analogs) 6 or modifications in pancreatic–enteric anastomotic techniques that can be discriminated by the site of jejunum used (end versus side), the type of anastomosis (invagination versus duct-to-mucosa), the use of an isolated Roux-en-Y limb, and the use of pancreatic ductal stenting or fibrin glue.7–12 However, there is yet no consensus on one particular technique being safer and less prone to pancreatic leakage.
Besides the anastomotic technique, other factors as soft pancreatic texture (most emphasized), small pancreatic duct (<2 mm), and high pancreatic juice output have also been considered predisposing to pancreatic leakage.3,6,13 Soft pancreatic parenchyma might be a risk factor because the sutures tend to lacerate the fragile pancreatic gland and thus cause pancreatic leakage. 14 The technique of mesh-reinforced pancreaticojejunostomy is favored for patients with a soft pancreatic remnant, as the mesh solidifies the pancreatic stump to sustain the anchoring sutures, thus reducing the probability of anastomotic dehiscence from disrupted sutures in soft pancreatic parenchyma. Furthermore, the mesh in the anastomosis may promote fibroblast attachment and enhance the anastomotic healing process.
However, when a narrow jejunal lumen cannot accommodate the pancreatic stump, even one constricted by a mesh strip, the mesh-reinforced pancreaticojejunostomy is obviously not an appropriate option. We therefore established the present new pattern of pancreaticogastrostomy with application of the mesh-reinforcement technique to solve this problem.
In recent years, pancreaticogastrostomy has regained its popularity as an option for digestive tract reconstruction after pancreaticoduodenectomy.15,16 It has been considered to have potential advantages over pancreaticojejunostomy in terms of reducing the incidence of postoperative pancreatic leakage. First, with pancreaticogastrostomy, secretions from the pancreatic stump can be effectively drained by a nasogastric tube, and this is particularly favored for those cases with high pancreatic juice output. Second, after pancreaticogastrostomy, the pancreatic secretions enter the potentially acidic gastric environment, where the low pH prevents their activation. 17 Post-pancreaticoduodenectomy hemorrhage from the pancreatic stump occurs in 5%–16% of patients who undergo pancreaticojejunostomy,18–21 and re-laparotomy is usually needed. In contrast, with pancreaticogastrostomy, pancreatic stump bleeding can be conveniently controlled by gastroscopic hemostasis. 22
The procedure of mesh-reinforced pancreaticogastrostomy exploited the technique of wrapping the pancreatic remnant with a mesh strip, which was designed to avoid laceration of anastomotic sutures and prevent pancreatic leakage. It spontaneously contained the potential advantages of pancreaticogastrostomy over pancreaticojejunostomy noted above. In our series, no patient was recognized to have a grade B or C pancreatic leakage after pancreaticoduodenectomy. Grade A pancreatic leakage occurred in 1 case (7.7%). The incidence of postoperative pancreatic leakage with the current procedure seems encouraging when compared with the results from high-volume centers. 17 Nonetheless, further prospective study in randomized patients is needed to validate our preliminary results.
In the present procedure, the pancreatic remnant was wrapped and compressed with a mesh strip. To decrease the potential risk of pancreatic duct stricture, a stent tube was used. Nine patients who originally possessed normal-sized pancreatic ducts were followed up with ultrasonography 3 months after operation, and the diameters of the ducts were measured for comparison with preoperative data. Not a single case had a dilated pancreatic duct in the follow-up, demonstrating that the stent withstood compression by the mesh strip.
Another concern about this technique is whether the mesh strip, an implanted foreign body, increases the risk of intra-abdominal infection. None of the patients in the current study had a postoperative infected intra-abdominal collection. Therefore, the use of a mesh strip during the procedure seems to be safe, so long as all parts of the mesh were covered in the gastric lumen after completion of the anastomosis. During the later period of this study we used mesh strips of absorbable material (Biodesign), which degrades in 2–3 months and thus avoids the persistent stimulation by foreign material. The initial results are promising and still need a large sample experience for appropriate evaluation.
In conclusion, the mesh-reinforced pancreaticogastrostomy provides surgeons with a new way to perform pancreatic–enteric drainage after pancreaticoduodenectomy that is simple, procedurally straightforward, and applicable to all types of pancreatic remnant.
Footnotes
Acknowledgments
The authors thank Prof. Iain C. Bruce (Zhejiang University School of Medicine) for reading this manuscript. The study was supported by Zhejiang Science and Technology Agency grant 2009C33095.
Disclosure Statement
No competing financial interests exist. None of the authors received any money or free supplies from the mesh manufacturer.