
Abstract
Abstract
Purpose:
Over the past decade, laparoscopic techniques have markedly evolved, and it has been shown that minimally invasive surgery can provide a safe, effective, and less traumatic management of various surgical diseases. Additionally, it is well known that pancreatitis itself also produced severe oxidative tissue injury by increasing levels of reactive oxygen species. This study therefore aimed to investigate the effects of pneumoperitoneum on the severity of pancreatitis in a rat model of acute pancreatitis induced by cerulein.
Materials and Methods
: Thirty-five Wistar albino rats were divided into five groups with seven rats in each. Experimental pancreatitis was induced using intraperitoneal injection of cerulein. The first group received open laparotomy. Groups 2–5 were treated with 5, 10, 15, and 20 mm Hg, respectively, achieved by applying pressure and waiting for 60 minutes. After this waiting interval, all of the rats were sacrificed; blood samples were taken by intracardiac puncture for biochemical assays, and pancreatic tissue samples were taken for light microscope analysis. Histopathology was scored according to edema, granulation, polymorphonuclear leukocytes, and mononuclear cells in all groups.
Results:
Great increases in malondialdehyde and reduced glutathione levels were seen in all of the groups in which pancreatitis was induced. In Group 2–5, more significant increases were detected than in the open laparotomy group (P<.005). In the histopathological examination, Groups 2–5 showed more inflammatory cell infiltration, edema, and granulation tissue than the open laparotomy group (P<.005).
Conclusions:
It is useful to remember the parameters of the medical treatment of pancreatitis. While surgical treatment is being decided, we think that the process of all kinds of surgery, including laparoscopic surgery, can increase the severity of pancreatitis.
Introduction
Although more than a century has passed since their identification, and a large number of clinical experimental studies have been conducted during this time, there is still no consensus on the pathogenesis of AP, whether there is a direct relationship between the etiological factors and pathogenesis, and the most efficient treatment. Moreover, today AP is one of the most important medical problems with high rates of morbidity and mortality.3–5
Diagnosis of AP can be established after the clinical picture and biochemical and radiological evaluations. Open or laparoscopic cholecystectomy is planned, especially in gallstone-induced pancreatitis cases.
Laparoscopic interventions have been implemented for the diagnosis and treatment of almost all the benign or malignant pathologies, especially in the last two decades. These operations are increasingly accepted by both the patients and surgeons and are widely used. Laparoscopic cholecystectomy is applied in cases with biliary pancreatitis due to the pathology of the gallbladder. There are only a few studies about the effects of laparoscopy in the case of pancreatitis. To our knowledge, there is no study about the effects of the level of pneumoperitoneum on the severity of pancreatitis.
The objective of this study was to investigate the effects of pneumoperitoneum and laparotomy induced with various intra-abdominal pressures on the severity of pancreatitis in the model with created experimental AP.
Materials and Methods
Animal groups
Thirty-five Wistar albino rats weighing 280–350 g were used in this study. The animals, supplied from the Experimental Animals Laboratory of the Afyon Kocatepe University Faculty of Medicine, were housed in individual cages and kept under standart conditions(12-hour light–dark cycle and temperature between 22°C and 28°C) with free access to a standard rat chow and water ad libitum. The present experimental protocol was designed in accordance with the 1996 guidelines for the care and use of laboratory animals from the U.S. National Institutes of Health and approved by the ethics commission of the Afyon Kocatepe University.
Experimental procedure
Following an overnight fasting AP was induced in the animals by three subcutaneous injections of cerulein (Sigma-Aldrich, Munich, Germany) at 80 μg/kg of body weight. After a 1-hour observation period from the last cerulein injection, anesthesia was induced by intramuscular injection of ketamine HCl (5 mg/kg; Ketalar®; Eczacıbaşı-Werner Lambert, Istanbul, Turkey). Additional anesthesia was given for the rats that required excess anesthesia during the experimental procedure.
The rats were randomly divided into five groups of seven rats each, as follows: Group 1 (control group), nonmanipulated; Group 2, CO2 pneumoperitoneum applied for 60 minutes at a pressure of 5 mm Hg after induction of AP; Group 3, CO2 pneumoperitoneum applied for 60 minutes at a pressure of 10 mm Hg after induction of AP; Group 4, CO2 pneumoperitoneum applied for 60 minutes at a pressure of 15 mm Hg after induction of AP; and Group 5, CO2 pneumoperitoneum applied for 60 minutes at a pressure of 20 mm Hg after induction of AP.
First, midline laparotomies were performed in all rats, and then catheters were placed into the peritoneum to create a pneumoperitoneum using the technique of Polat et al. 6 Study groups 2–5 were subjected to 60 minutes of pneumoperitoneum with intra-abdominal pressure of 5, 10, 15 and 20 mm Hg, respectively, followed by 30 minutes of deflation.
At the end of the experimental procedure, the rats were sacrificed. Incisions were reopened, and then blood samples (5 mL) were obtained from the heart for biochemical assays. Tissue (2×2cm) samples were taken from the pancreas for histopathological examination. Plasma was separated by centrifugation at 800 g at 4°C for 10 minutes after blood samples were drawn into the heparinized tubes. The tissue samples were fixed in a 10% buffered formalin for histopathological analysis. They were embedded in paraffin, cut into sections 3 μm thick, stained with hematoxylin–eosin, and examined by a pathologist who was unaware of treatment and test groups. Each section of pancreatic tissue was scored from 0 to 3 points in terms of the presence and degree of interstitial edema, mononuclear cell infiltration, polymorphonuclear cell infiltration, granulation tissue, and necrosis. The severity of pancreatitis was evaluated to these individual scores (Table 1).
The total sum of histopathological scores was obtained for all study groups by combining the individual parameters. Data were expressed as mean±standard error of the mean values. Data analyses were performed by using chi-squared test. The Monte Carlo simulation method was used for values less than 5. One-way analysis of variance was used to compare the parameters that had three or more groups. As a result of the one-way variance analysis, Bonferroni's test was used to compare variables with significant differences. Statistical significance was set at P<.05.
Results
The microscopic view of the pancreatic tissues revealed that cerulein injection caused edema, inflammatory cell infiltration, and the formation of granulation tissue in all rats in which pancreatitis was induced. Edema was less in the control group than in the other study groups (P<.05) (Fig. 1). There was a statistical difference for mononuclear cell infiltration and polymorphonuclear leukocyte infiltration between the study groups and the control group (P<.005). Mononuclear cell infiltration and polymorphonuclear leukocyte infiltration in the 5 mm Hg group were higher than in the other groups (Fig. 2). Levels of granulation tissue in the 5, 10, 15, and 20 mm Hg study groups were significantly higher than in the control group (P<.005). The most significant granulation tissue was encountered in the 15 mm Hg group (Fig. 3).
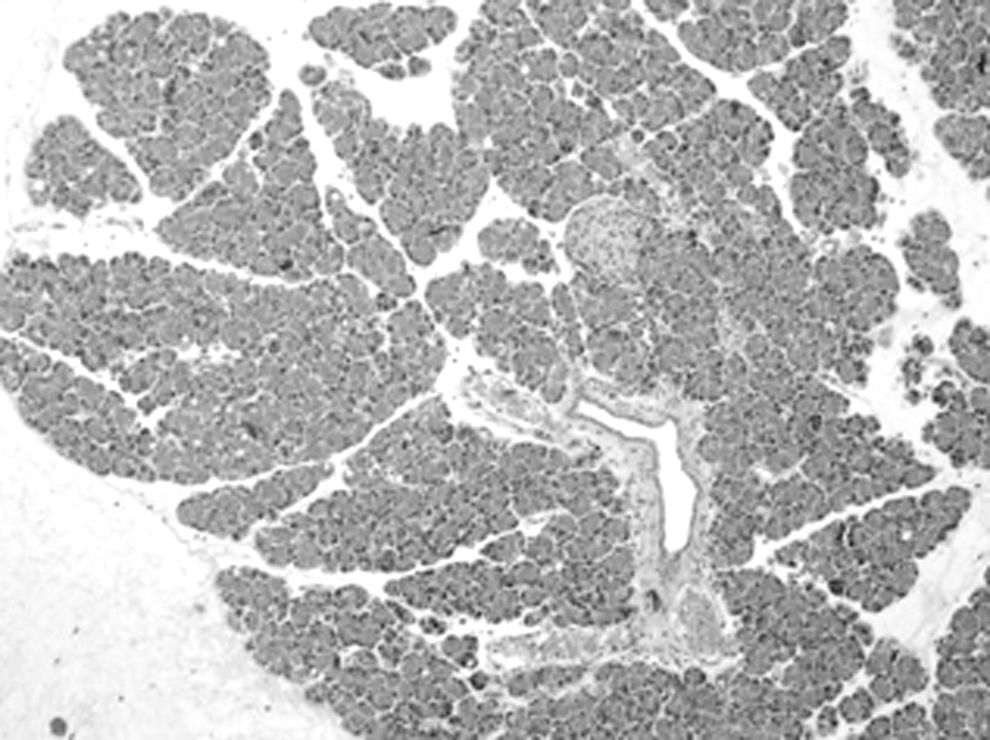
Microscopic view of the pancreatic tissue edema in the control group.
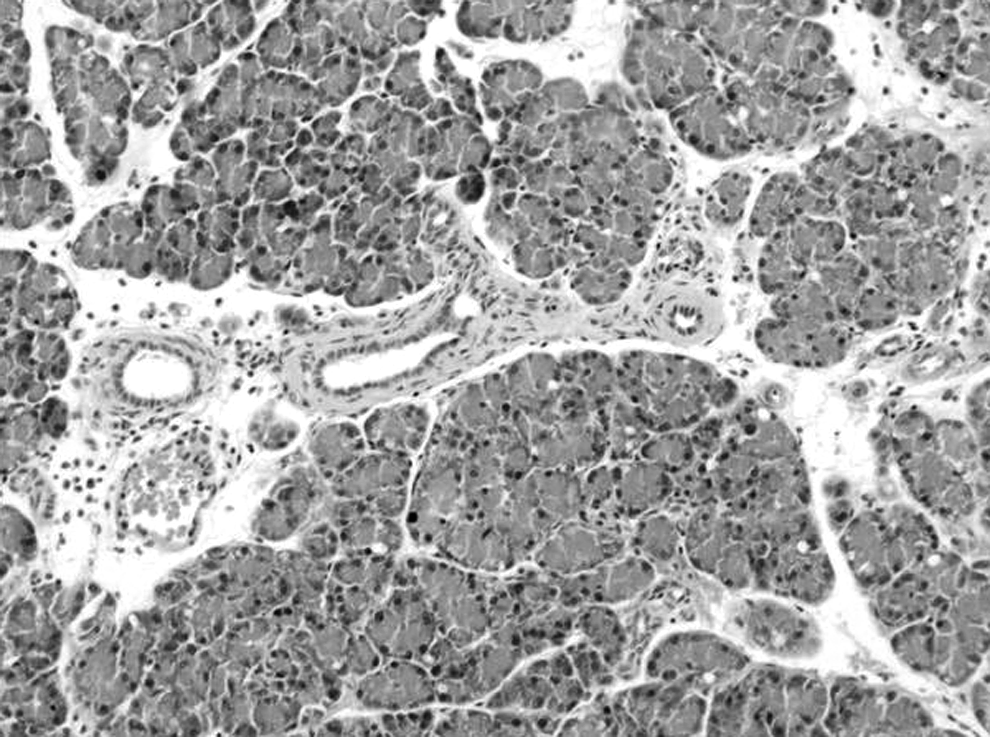
Mononuclear cell infiltration and polymorphonuclear leukocyte infiltration of pancreatic tissue in the 5 mm Hg group.

Formation of granulation tissue in the 15 mm Hg group.
Mean malondialdehyde and reduced glutathione values of the control group and groups treated with intra-abdominal pressures of 5, 10, 15 and 20 mm Hg are shown in Figures 4 and 5, respectively. Great increases in malondialdehyde and reduced glutathione levels were seen in all of the groups in which pancreatitis was induced. In Groups 2–5, subjected to intra-abdominal pressures of 5, 10, 15, and 20 mm Hg, respectively, more significant increases were detected than in the open laparotomy group (P<.05).
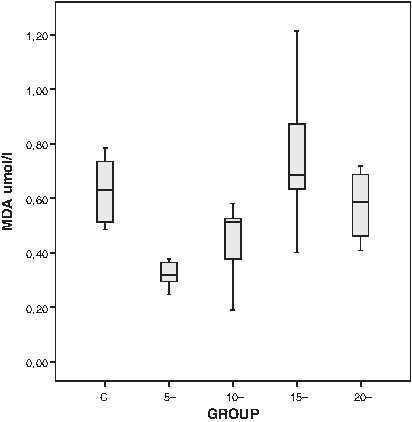
Mean malondialdehyde (MDA) values of the study groups: C, control group; 5, 5 mm Hg pneumoperitoneum; 10, 10 mm Hg pneumoperitoneum; 15, 15 mm Hg pneumoperitoneum; and 20, 20 mm Hg pneumoperitoneum.
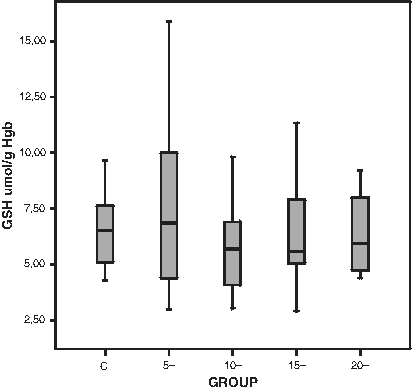
Mean reduced glutathione (GSH) values of the study groups: C, control group; 5, 5 mm Hg pneumoperitoneum; 10, 10 mm Hg pneumoperitoneum; 15, 15 mm Hg pneumoperitoneum; and 20, 20 mm Hg pneumoperitoneum. Hgb, hemoglobin.
Discussion
Surgical treatment of cholelithiasis, which is the most important cause of pancreatitis, is administered to the patients in an early period following hospitalization and medical therapy of patients with AP. 7 There is, however, a serious debate on the timing of the cholelithiasis operation. Most centers recommend the surgical operation to be done after the pancreatitis attack has subsided in the hospitalization period, but a few centers prefer to perform the proper operation after 6 weeks of medical therapy of pancreatitis.8,9 The main discussion around delaying the surgery is the probability for the risk of recurrence of AP during the waiting period. This recurrence may lead to a series of complications and problems, including necrotizing pancreatitis and even death.10–13 In addition, it is well known that when surgery is performed in the same period of hospitalization due to pancreatitis, patients will have quite low rates of complication and mortality with more economical conditions than the delayed surgery. However, surgical operation in the early period after subsidence of the pancreatitis attack has been reported to cause a higher level of operative risk, conversion, and complications because of the concurrent inflammation and adhesions, resulting in higher rates of morbidity and mortality.11,14
Surgical operation must be performed laparoscopically unless there is a definite contraindication. Laparoscopic surgery can also be achieved with the occurrence of pneumoperitoneum. Pneumoperitoneum is frequently realized via intraperitoneal insufflation of CO2 during laparoscopy, and it has been shown that laparoscopic procedures alter systemic and pulmonary hemodynamic parameters, change acid–base profiles, increase the incidence of bacterial translocation, and affect hepatic and gastrointestinal perfusion.15–20 Besides gastrointestinal system organs, pancreatic circulation is also affected in some degree even at very low intra-abdominal pressure values. Schafer et al. 21 demonstrated that pancreatic circulation was decreased by 52.2% with an intra-abdominal pressure value of 4 mm Hg and that the rates even reached 57.5% at the values below usual pressures used during surgical operations such as 10 mm Hg. Therefore, we used intra-abdominal pressure values of 5, 10, 15, and 20 mm Hg. Decreased perfusion of splanchnic organs due to increased pressure during pneumoperitoneum and reperfusion developing after the termination of pneumoperitoneum reflect a typical ischemic reperfusion model. 22
Ischemic reperfusion injury causes the majority of damages complicating the reversible arterial regurgitation of the splanchnic area. Morover, ischemic reperfusion injury impairs healing and is the most likely mechanism of the detrimental effect of the high intra-abdominal pressures on anastomoses reported originally by our group. 23 Ischemia reperfusion injury leads to “oxidative stress,” which propagates further injury.20,24
Besides laparoscopic operations, pancreatitis itself has been shown in several clinical and experimental studies to lead occurence of oxygen free radicals forming lipid peroxides, especially in the early period.25,26 Different experimental pancreatitis models can be created for this purpose. Injection of intraperitoneal cerulein induces limited moderate edematous pancreatitis without major pancreatic complications. 27 This model is preferred to investigate nonfatal cellular biological events in pancreatitis. Inflammatory cells that infiltrate interstitial spaces in pancreatitis induced by cerulein are neutrophils, monocytes, and macrophages. Inflammatory cell infiltration is a common finding in human pancreatitis, and the cells that produce the most free oxygen radicals are neutrophils. The resultant free oxygen radicals cause changes in acinar cells and lead to endothelial damage as well as microvascular disorder in the tissue and increase in capillary permeability with fluid accumulation. These products have been shown in detail to create a severe tissue damage in several experimental and clinical studies.28–30 It is well known that in the presence of pancreatitis many inflammatory mediators and oxidative stress markers formed in the early period play a key role in the pathogenesis of AP regardless of the causal factor.31–33
We found that laparoscopy procedures increased the histopathological injury observed after laparoscopy alone. This detrimental effect was related especially to decreased inflammatory cell infiltration and acinar vacuolization. It also significantly increased the levels of malondialdehyde, which is a reliable marker for end-stage oxidative injury in the study groups in which pancreatitis occurred (P<.05). Reduced glutathione has a pivotal role in cellular defense mechanisms and plays a major role in decreasing the tissue injury induced by free oxygen radicals following ischemic reperfusion injury.18,19 We found that laparoscopic procedures have also increased the reduced glutathione consumption (P<.05). The results of the present study suggest that laparoscopy may deteriorate the severity of the pancreatis in patients with pancreatitis.
In AP, tissue edema, polymorphonuclear leukocytes, mononuclear cell infiltration, and formation of granulation tissue were seen in our study groups. However, we found these factors to be lower in the laparotomy group than in the other groups. Significant findings included that the edema beaome severe with increased pneumoperitoneum, the massive increase of the number of mononuclear cells in the 5 mm Hg group, and the prominent infiltration of polymorphonuclear leukocytes. In a study by Yol et al. 9 with the same parameters, less edema and mononuclear cell infiltration were reported in the pneumoperitoneum groups.
To our knowledge from the literature, the opposite of our current results were found only by Yol et al. 9 regarding the effects of pneumoperitoneum on the severity of pancreatitis in cases of experimental pancreatitis. Contrary to the results of Yol et al. 9 indicating that intra-abdominal pressure application of 12 mm Hg for 30 minutes did not negatively affect the severity of pancreatitis, in our study we found that CO2 pneumoperitoneum negatively affected the severity of pancreatitis. Yol et al. 9 used a pneumoperitoneum duration of 30 minutes, whereas performing a laparoscopic cholecystectomy operation requires a period of approximately 1 hour in cases with biliary pancreatitis due to gallbladder stones. Therefore, we used a pneumoperitoneum time of 1 hour in all our study groups and found that the severity of the pancreatitis was affected negatively following the pneumoperitoneum application. Perhaps in the previous studies negative changes with CO2 pneumoperitoneum application such as splanchnic hypoperfusion, changes in systemic and pulmonary hemodynamics, disturbances in acid–base profile, and formation of bacterial translocation do not take place adequately after the application of 30 minutes of pneumoperitoneum. Thus, we believe that designs of studies evaluating the changes following pneumoperitoneum application of 30 minutes should be re-evaluated.
In conclusion, we can say that treatment of pancreatitis should be medical as before, and even if the decision is made for laparoscopic surgery that is minimally invasive, it would be more appropriate to think one more time of all the operations in pancreatitis cases.
Footnotes
Disclosure Statement
No competing financial interests exist.