
Abstract
Abstract
Purpose:
Laparoendoscopic single-site surgery (LESS) has been proposed for several intra-abdominal surgical interventions. However, application of the LESS technique in portal hypertension is still in its infancy. We report in this article a new technique of LESS splenectomy plus pericardial devascularization with conventional laparoscopic instruments in patients with portal hypertension.
Patients and Methods:
From January 2010 to April 2012, LESS splenectomy plus pericardial devascularization was performed on 5 patients with portal hypertension. Surgical techniques and short-term outcomes were summarized and analyzed retrospectively.
Results:
All the operations were successful with a mean operative duration of 252 minutes (range, 220–270 minutes), intraoperative blood loss of 290 mL (range, 250–350 mL), and hospital stay of 8.2 days (range, 7–9 days). No intraoperative or postoperative complications were recorded. The umbilical incision healed well with a satisfactory cosmetic effect.
Conclusions:
LESS splenectomy plus pericardial devascularization is feasible when performed by experienced laparoscopic surgeons and may offer safety comparable to that of the conventional laparoscopic operation.
Introduction
Laparoendoscopic single-site surgery (LESS) is performed either through a single port with several work channels or through independent trocars within a single incision (e.g., the umbilicus). The umbilical incision can be easily hidden in the umbilical fold, making it the most available technique for “scarless” surgery. Here, we describe our initial experience with the application of LESS splenectomy plus pericardial devascularization with conventional laparoscopic instruments in 5 patients with portal hypertension.
Patients and Methods
Patients
Five consecutive patients were retrospectively reviewed from a prospective database of laparoscopic splenectomy plus pericardial devascularization. All had a history of type B hepatitis, hepatocirrhosis, and recurrent hematemesis after medication. Gastroscopy showed a positive red-color sign. Laboratory readings and computed tomography scan showed Child–Pugh Class A liver function, a low platelet count, and splenomegaly. Splenectomy and pericardial devascularization were performed for the 5 patients. All patients were provided with complete informed consent regarding the nature of the surgical procedure and risks involved before consents were obtained. The study was performed under institutional review board approval.
Technique
The procedures were performed with the patient under general anesthesia and in the supine position with legs parted and the left shoulder raised 15°–20°. The viewing monitor was placed above the patient's left shoulder, with the surgeon standing between the patient's legs and the camera operator on the patient's right side. Pneumoperitoneum was established by using closed Veress needle technique through the umbilicus. After insufflation of CO2 and maintaining the pressure at 13 mm Hg, a 3-cm periumbilical incision was made, preserving the fascial layer for trocar access. Conventional trocars were used, including a 5-mm and a 10-mm standard trocar and an unbladed trocar (Xcel B12LT; Ethicon Endo-Surgery, Inc., a Johnson & Johnson Company, Cincinnati, OH). The three ports were placed within the umbilical incision in an inverted equilateral triangular configuration, 1 cm apart, with the camera placed at the apex. A 30° 10-mm rigid laparoscope (Stryker Endoscopy, San Jose, CA) was used throughout the procedures. A grasper is inserted through the 5-mm trocar, while a Harmonic® scalpel (Ethicon Endo-Surgery) or LigaSure™ (Covidien Surgical Solutions Group, Boulder, CO) is inserted through the 12-mm trocar for dissection.
First, the laparoscopic splenectomy was performed. It was performed by a lateral approach with the left side of the patient elevated 30°–45°. A thorough intra-abdominal examination was performed to assess for the presence of accessory splenic tissue. After this assessment has been completed, the dissection began with division of the splenocolic and gastrocolic ligament with a 5-mm Harmonic scalpel or a LigaSure. Then, the spleen was elevated properly by the assistant hand, while the LigaSure held by the dominant hand was used to divide and dissect the splenorenal ligament. Then, the splenophrenic ligament attached to the upper pole of the spleen was freed with the LigaSure, leaving the spleen hanging only on its pedicle. The branches of the splenic vein were engorged and contorted and were first ligated with absorbable clips before they were divided using a LigaSure. The position was reversed to stretch the pedicle, and a 60-mm endoscopic stapler (white cartridge) through the 12-mm trocar was used to dissect the pedicle (Figs. 1 and 2). The whole spleen was resected.

Introducing the Endo GIA.
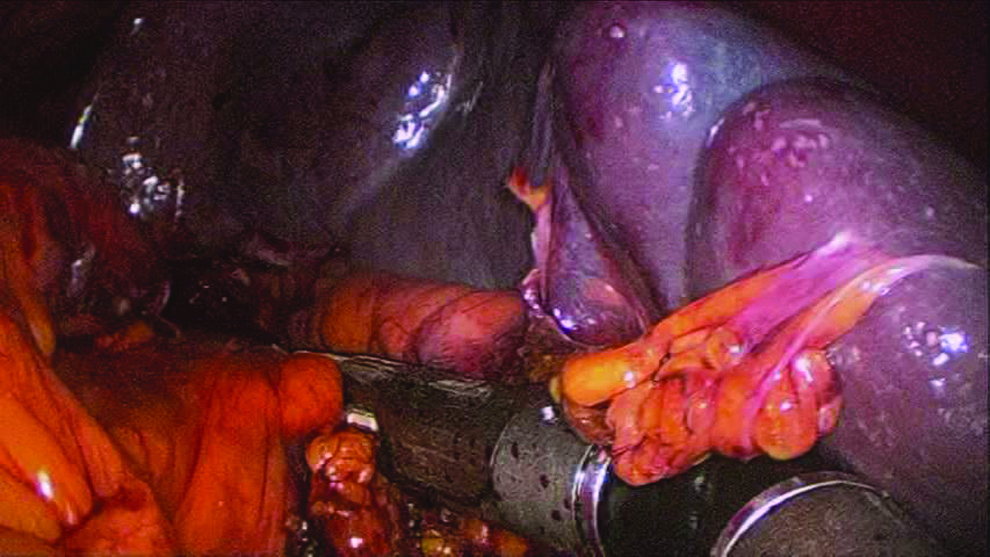
The splenic pedicle was stapled with the Endo GIA.
For the second stage of the procedure, devascularization was performed from the greater curvature of the stomach, which had been opened during the splenectomy procedure to the area of the upper gastric fundus. The esophagus was pulled downward. Vessels around the lower esophagus were dissected superior to a point 6 cm away from the esophagocardia junction. Then the gastrohepatic ligament was opened, and devascularization of the lesser curvature was performed by the same way. With the use of a LigaSure, this procedure can be performed without significant bleeding. A large draining vein left gastric vessel was ligated with an Endo GIA™ stapler (Covidien, Mansfield, MA) (Fig. 3).
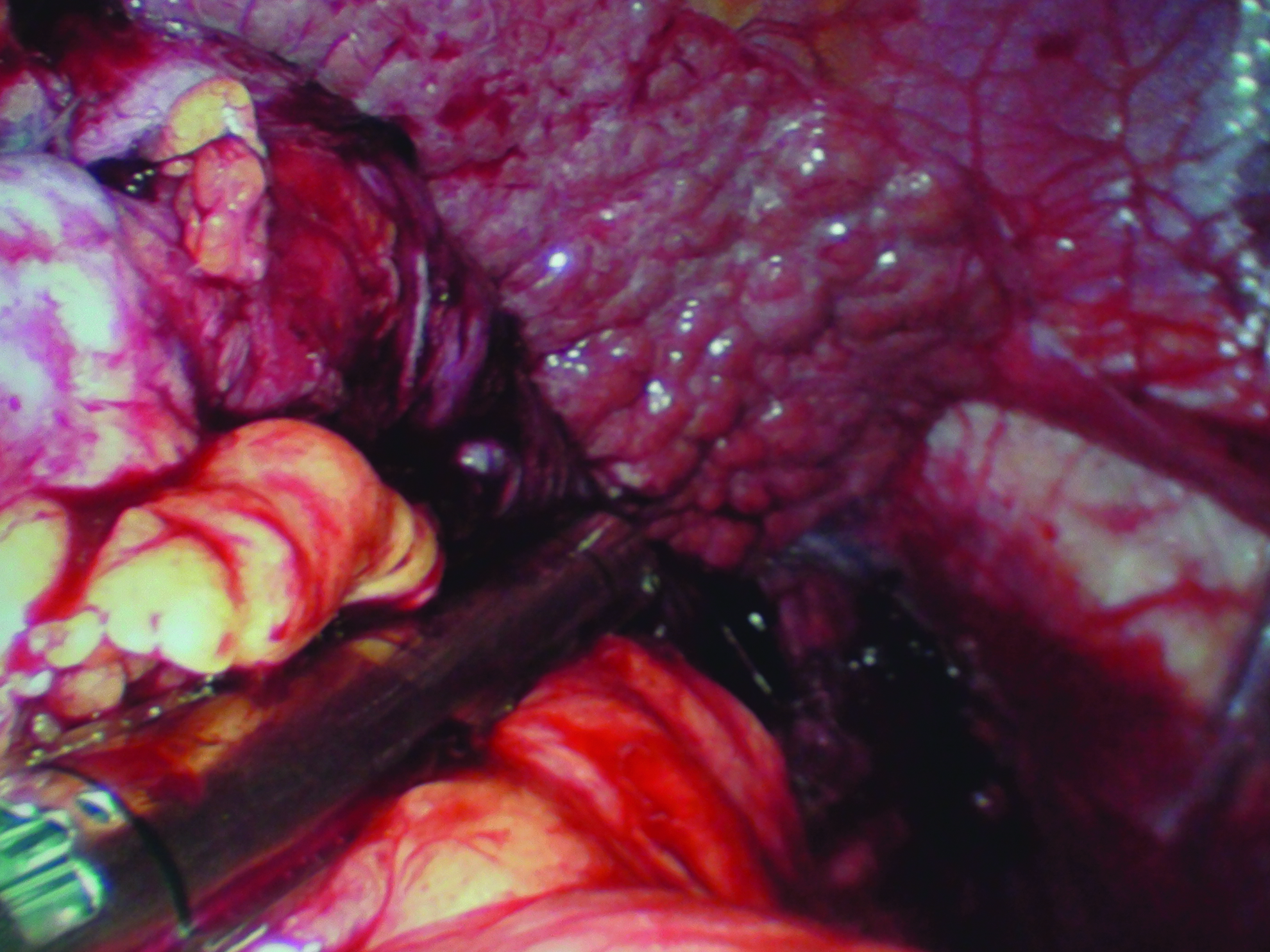
Ligation of the coronary vein with the Endo GIA.
For all cases, a specimen bag was finally inserted through the 12-mm trocar, and the spleen was placed in it to be removed piecemeal from the abdominal cavity. We placed a single drainage tube at the splenic bed, which came out from the abdomen through the umbilical incision. The umbilical incision was closed in two layers, with a purse string left around the drain for later closure when the drain was removed.
Results
The demographic data for each patient are shown in Table 1. All the five operations were successful without conversion to open or conventional multiple-incision laparoscopic surgery with a mean operative duration of 252 minutes (range, 220–270 minutes), intraoperative blood loss of 290 mL (range, 250–350 mL), and hospital stay of 8.2 days (range, 7–9 days). No intraoperative or postoperative complications were recorded. There were no wound infections in the cohort (Table 2). Patients were uniformly pleased with the cosmetic results of the operation (Fig. 4).

Postoperative umbilical incision.
BMI, body mass index.
Discussion
The ideal surgical procedure for patients with bleeding portal hypertension and secondary hypersplenism should control bleeding, correct hypersplenism, and avoid recurrence of bleeding, with little impairment of liver function and a low rate of encephalopathy.
The many treatment modalities available suggest that no single therapy is entirely satisfactory for all patients or for all clinical situations.7–9 Currently, shunt and devascularization surgeries are two basic surgical methods, but shunt procedures are more commonly used in Western countries, and devascularization procedures are more commonly used in China.10,11 Recently, endoscopic treatments have showed great promise for esophageal varices. However, such treatment cannot treat severe hypersplenism. Although combined open splenectomy and pericardial devascularization is a suitable procedure, it has several disadvantages, including more surgical stress, bigger operation incision, etc. A new minimally invasive surgical treatment is necessary for patients with portal hypertension who usually have poor tolerance ability for the operation. The laparoscopic procedure is a typical minimally invasive operation, which is accepted throughout the world. Laparoscopic splenectomy has become the gold standard for removal of normal to moderately enlarged spleens. However, it is really more challenging when laparoscopic splenectomy is performed on patients with cirrhosis, portal hypertension, and splenomegaly because portal hypertension and the severity of liver cirrhosis are the risk factors for high intraoperative blood loss during the procedure.
Although experience with LESS is still its infancy, as clinical experience increases, no differences in any operative variables compared with conventional laparoscopy were noted in some reports. 12 It is undeniable that LESS is made difficult because of the parallel arrangement and clashing of instruments, added to the constant interference between the surgeon and the camera operator.13–15 In our operation, the instruments were arranged in an inverted triangular form, with the instruments above the camera to ensure an adequate field of view. Coordination between the surgeon and the camera operator in this procedure is vital; the laparoscope viewing the operating field at an lateral angle giving way to the main work instrument at the center of the field of view, coupled with minute adjustments by the surgeon and camera operator, should ensure smooth completion of surgery.
A massively enlarged spleen may be seen in hypersplenism due to portal hypertension.When making the umbilical incision and placing the trocars, care should be taken to prevent accidental injury of a massively enlarged spleen. The whole procedure should be carefully done here, avoiding using a Harmonic scalpel or LigaSure to directly coagulate the engorged splenic vein, as this vessel is wide and thin-walled, and bleeding from it may be difficult to control. Therefore the LESS procedure should be done first with the easy steps and then later with more difficult steps, dissecting areas with no blood vessels or fewer blood vessels first, freeing the spleen of its attachments, and then using the endoscopic stapler to dissect the blood vessels of the portal spleen in one bite.
Application of LESS in laparoscopic splenectomy was first performed in 2 cases of idiopathic thrombocytopenia successfully by Barbaros and Dinççağ 16 in 2009. Herein we successfully performed single-incision splenectomy plus pericardial devascularization in 5 cases of portal hypertension with hepatic cirrhotic. However, we are still in the initial learning curve. Although LESS splenectomy plus pericardial devascularization may further reduce injury caused by surgery and produce a better cosmetic result, we should be aware of the potential difficulties and challenge of the procedure. Validated patient outcome data are required to objectively address this final comment.
Conclusions
It is our opinion that LESS splenectomy plus pericardial devascularization is feasible for experienced laparoscopic surgeons. However, it requires a considerably high level of skills to perform and should only be attempted by highly skilled persons. It should be kept in mind that improved cosmesis must be carefully weighed against the potentially increased difficulties and risks of the procedure. Its merits and shortcomings when compared with the conventional laparoscopic splenectomy are yet to be demonstrated in a prospective clinical study.
Footnotes
Disclosure Statement
No competing financial interests exist.