
Abstract
Abstract
Background:
Choledocholithiasis is a complex problem in patients with Roux-en-Y gastric bypass anatomy. Several techniques of biliary clearance have been described, but these can be limited by intra-abdominal adhesions.
Patient and Methods:
A 36-French surgical gastrostomy was created and was allowed to mature for 10 weeks. It was exchanged for a 15-mm laparoscopic surgery trocar under fluoroscopic guidance. Endoscopic retrograde cholangiopancreatography (ERCP) was carried out using the trocar as a stable access point. Complete biliary clearance was achieved in one sitting using sphincterotomy, large-diameter biliary orifice balloon dilation, and balloon/basket sweeps.
Results:
Total endoscopy time was 120 minutes. There were no complications associated with the procedure. The postprocedure length of stay was 2 days. The total bilirubin level at discharge was 1.2 mg/dL (20 μmol/L).
Conclusions:
In patients with gastric bypass anatomy and severe adhesions, successful salvage therapeutic ERCP can be achieved using a gastrostomy tract and a large-bore laparoscopy trocar for access to the defunctioned stomach.
Introduction
Patient and Methods
A 53-year-old man was referred with choledocholithiasis. He had undergone laparoscopic Roux-en-Y gastric bypass surgery 3 years earlier and lost only a modest amount of weight. He weighed 181 kg at presentation (body mass index, 58 kg/m2). Prior to this referral, he also had a challenging laparoscopic subtotal cholecystectomy converted to the open procedure, complicated by prolonged bile leak.
The patient underwent laparotomy and attempted CBD exploration, after a failed attempt at percutaneous transhepatic biliary drainage (only mildly dilated bile ducts). Unfortunately, the abdomen contained prohibitive adhesions, and the porta hepatis was severely scarred, preventing the successful completion of the procedure. Instead, a Stamm gastrostomy was fashioned in the defunctioned portion of the stomach using a 36-French Malecot catheter. This tube was positioned on the anterior mid-body and was exteriorized directly through the overlying abdominal wall. Given the significant thickness of the abdominal wall, the gastrostomy was allowed to mature for 10 weeks. This time delay was felt to be acceptable in the context of incomplete biliary obstruction (the total bilirubin level was always 1–2 mg/dL [35–50 μmol/L]).
The patient was brought back electively for ERCP. The gastrostomy was removed over a guidewire. The tract was dilated using a 16-×40-mm balloon, and a 15-mm bariatric laparoscopy trocar (Versaport™ Plus Bladeless; Covidien, Mansfield, MA) was inserted. Intragastric positioning was confirmed with fluoroscopy (Fig. 1). For added security, a 450-cm ERCP guidewire (Hydra Jagwire®; Boston Scientific, Natick, MA) was positioned in the distal duodenum and exteriorized through the trocar. The patient was positioned in 45° left lateral decubitus, allowing adequate access to the anterior abdominal wall. The side-viewing duodenoscope was then inserted through the trocar and advanced into the second portion of the duodenum (Fig. 2). Adequate positioning of the trocar was also confirmed endoscopically (Fig. 3). The papilla was readily visualized, and deep biliary cannulation was achieved using a combination of wire and contrast techniques. Given the unusual patient position, selective biliary cannulation required a slightly longer scope and a significant degree of bowing on the sphincterotome (Hydratome® RX; Boston Scientific). The final stable scope position was shorter and flatter than usual because of the direct access to the pylorus from the mid-body trocar, rather than the usual descent along the lesser curve of the stomach.
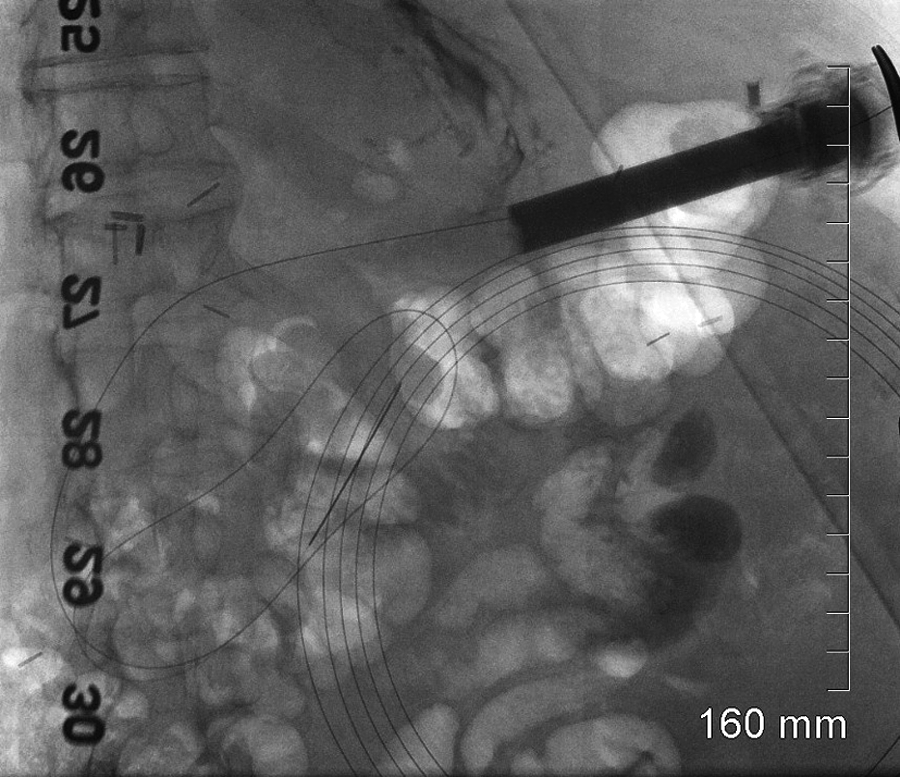
Fluoroscopic view demonstrating the trocar positioned within the stomach with the guidewire advanced into the distal duodenum.
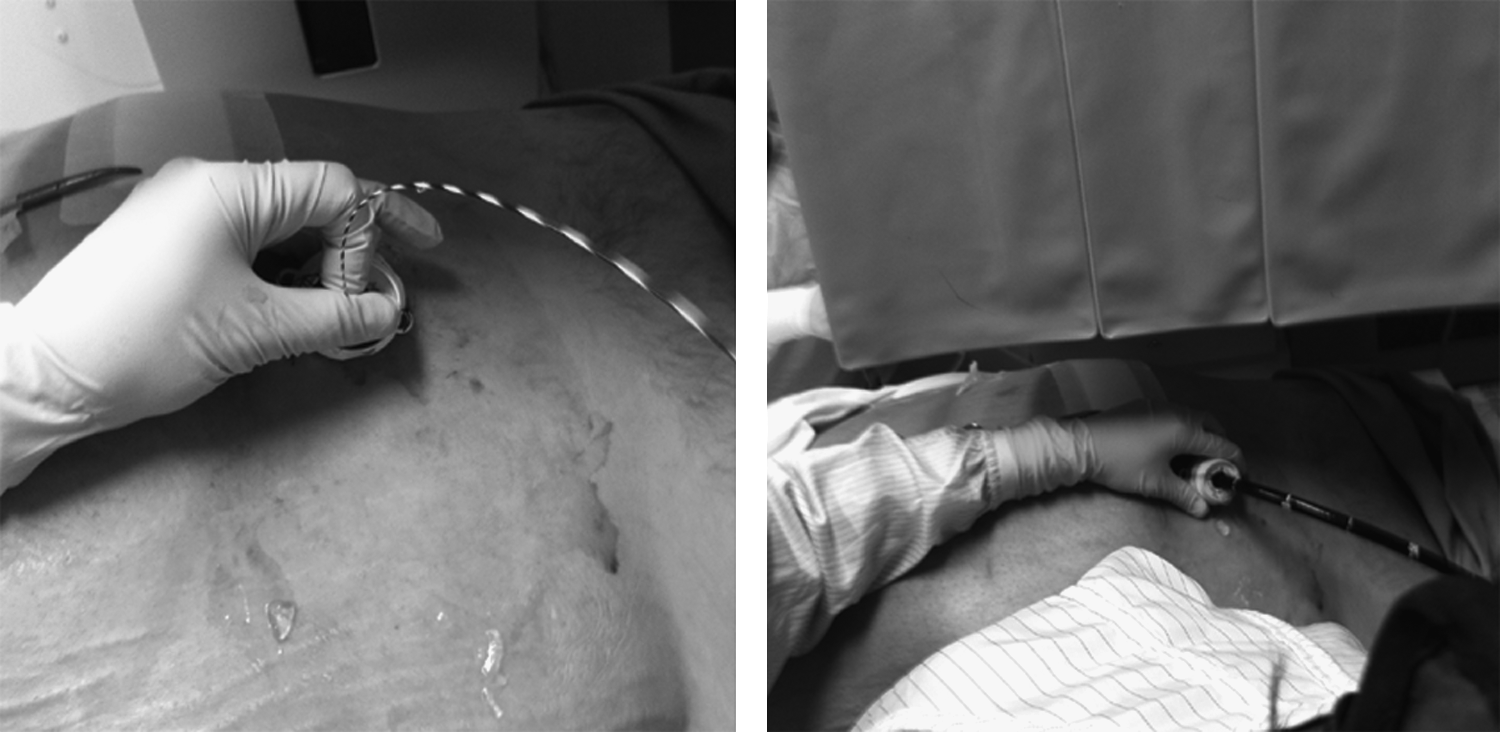
Intubation of the defunctioned stomach over a guidewire using a percutaneous 15-mm laparoscopic surgery trocar.

Retroflexed endoscopic view of the trocar positioned within the defunctioned stomach.
Large chronic, cast-like gallstones were identified on cholangiography (Fig. 4). A generous sphincterotomy was carried out. Given the size of the stones, the ampulla and distal CBD were dilated up to 15 mm using a balloon (CRE™ wireguided balloon dilator; Boston Scientific). 4 All stones were extracted in one session using a combination of 12–15-mm balloons (Extractor™ RX Pro; Boston Scientific) and baskets (FlowerBasketV™; Olympus, Richmond Hill, ON, Canada). At the end of the procedures, the laparoscopy trocar was exchanged over a guidewire for a 22-French Foley catheter, in order to maintain access for any further endoscopic intervention in the immediate postoperative period. This catheter size was much more convenient and comfortable for the patient. This catheter was subsequently removed in the clinic.
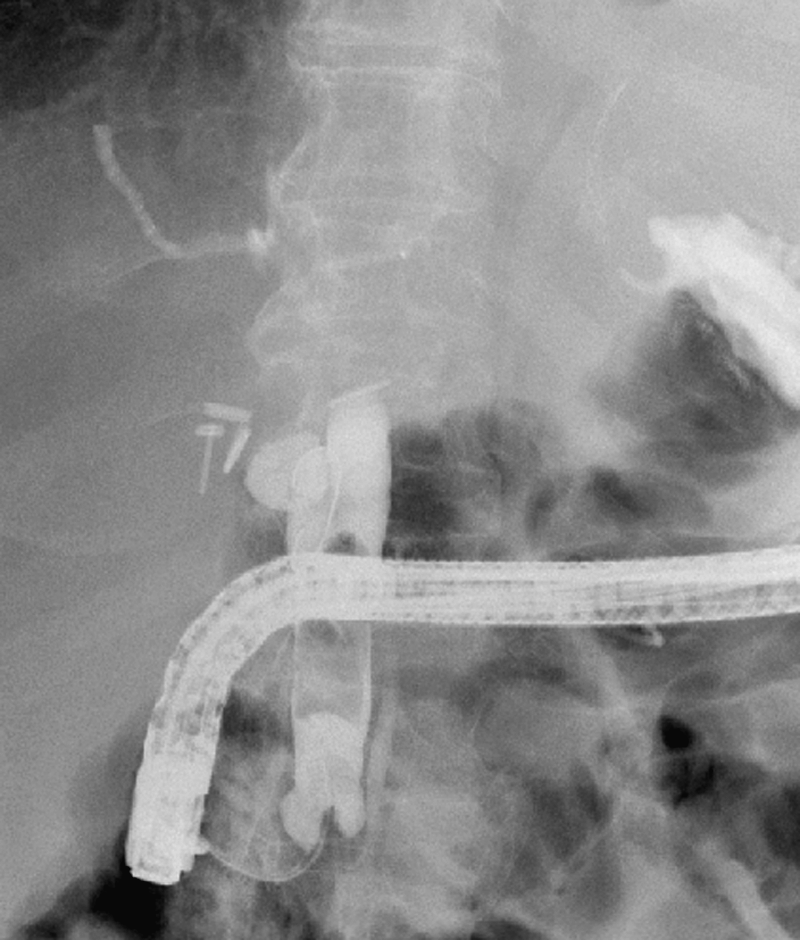
Cholangiogram demonstrating large cast-like calculi within a dilated common bile duct (note the duodenoscope's horizontal position).
Results
The total fluoroscopy time was 12.4 minutes. The total endoscopy time was 120 minutes. In total, 250 μg of intravenous fentanyl and 3 mg of midazolam were required for the procedure. There were no complications associated with the procedure. The patient did not develop pancreatitis or any other complication related to the large gastrostomy tract. The patient was monitored in the hospital for 2 days. At discharge, the total bilirubin level was 1.2 mg/dL (20 μmol/L).
Discussion
Gallstones develop in 13%–36% of patients following rapid weight loss.2,3 Fortunately, gallstone-related complications have been reported in only 0.2%–2.0% of gastric bypass surgery patients. 5 ERCP for choledocholithiasis is considered highly challenging in patients with Roux-en-Y anatomy. This is particularly true following gastric bypass surgery, where the Roux limb measures at least 100 cm and the biliopancreatic limb measures 50 cm from the ligament of Treitz to the enteroenterostomy. 1
Therapeutic ERCP options with Roux-en-Y anatomy have recently been reviewed. 6 The traditional option would require the advancement of a duodenoscope, enteroscope, or colonoscope per os, with the objective of navigating the Roux-en-Y anatomy. A variation on this approach involves the use of double- or single-balloon enteroscopes per os. Finally, the most recent technique requires that the endoscopist gain access to the defunctioned portion of the stomach by means of laparoscopic assistance or by means of a gastrostomy (surgical or radiologically assisted).
In this report, we have presented a technical variation upon the existing surgical gastrostomy-assisted ERCP technique first described by Baron and Vickers. 7 The approach we have described was highly successful because it allowed sufficient time for the track to mature completely, thus yielding excellent apposition of the stomach and abdominal wall. As well, the use of a large-bore laparoscopic surgery trocar positioned in the stomach allowed excellent manipulation of the duodenoscope, while providing a stable access point to the stomach. The ringed design of the trocar used in this case helped prevent insufflated air leakage around the gastrostomy track and prevented the trocar from slipping out of the stomach. Finally, this technique allowed endoscopic clearance of the CBD, despite intra-abdominal adhesions that were so severe as to prevent the safe completion of an open exploration and would have clearly prevented laparoscopic-assisted access to the stomach. Disadvantages of this technique include the time required for tract maturation and the invasive nature of a surgical gastrostomy, as well as the limited ability to use this approach for acute biliary clearance.
When faced with a patient with gastric bypass anatomy and choledocholithiasis, the treating team has now several therapeutic modalities at its disposal. Care of such patients should be reserved for centers with significant experience with the care of bariatric patients, as well as with advanced endoscopic/laparoscopic techniques. A few recent small series have detailed the use of gastrostomy-assisted ERCP in bariatric patients.8,9 Although the various endoscopic options have not been subjected to formal clinical trials, a recent report by Schreiner et al. 10 would suggest that laparoscopic-assisted ERCP is superior to balloon enteroscopy in achieving cannulation (100 versus 59%, P<.001) and therapeutic success (100% versus 59%, P<.001). We argue that the first line of endoscopic therapy for biliary pathology in patients with bariatric anatomy should be individualized. Factors to consider should include the acuity of presentation, the current weight of the patient, and a history of adhesions or previous intra-abdominal sepsis.
Conclusions
The management of choledocholithiasis in patients with Roux-en-Y gastric bypass anatomy is challenging. Successful salvage therapeutic ERCP can be achieved in the context of severe intra-abdominal adhesions using a gastrostomy tract and a large-bore laparoscopy trocar for access to the defunctioned stomach.
Footnotes
Acknowledgments
The Division of General Surgery and Department of Surgery at the Ottawa Hospital, University of Ottawa, are supported by unrestricted educational grants from Covidien Canada and Storz Canada.
Disclosure Statement
No competing financial interests exist.