
Abstract
Abstract
Background:
Several studies have reported faster recoveries, lower pain scores, and superior cosmetic results after mini-laparoscopic cholecystectomy (MLC). The purpose of this study was to perform a randomized controlled trial, comparing MLC with conventional laparoscopic cholecystectomy (LC).
Subjects and Methods:
Forty-one patients with symptomatic cholecystolithiasis were randomized between the two groups: 23 having undergone LC and 18 MLC. The primary end point was postoperative pain, which was evaluated during the first 24 hours postoperatively, using the numerical rating scale. Patient satisfaction with the cosmetic result was evaluated after 1 month.
Results:
The two groups were comparable concerning age, sex, and body mass index. The median operating time (42 minutes versus 45 minutes; P=.386), complication rate, and duration of hospital stay (2 days; P=.611) were similar in both groups. The level of postoperative pain was analogous at every time. There was no difference in the analgesic requirements or cosmesis.
Conclusions:
MLC showed similar results concerning postoperative pain and did not lead to a greater patient satisfaction with the cosmetic result, compared with LC. MLC did not take longer to perform, nor was it associated with major complications or a high conversion rate. MLC is a safe and feasible technique for the treatment of gallbladder disease in elective patients.
Introduction
The goal of this randomized controlled trial was to prospectively evaluate the impact of the implementation of MLC in our center in an elective setting, after a positive initial experience.
Subjects and Methods
Patient selection and end points
Only patients with chronic cholecystitis or symptomatic cholecystolithiasis requiring an elective cholecystectomy were included in this study. Exclusion criteria comprised the presence of complicated gallstone disease that could be assessed by preoperative blood analysis, ultrasonographic findings, and clinical features (acute cholecystitis, acute pancreatitis, choledocholithiasis), previous upper abdominal surgery, body mass index >30 kg/m2, antecedents of psychiatric disorders, very high risk for general anesthesia (American Society of Anesthesiologists grade IV), pregnancy, coagulation disorders, suspected or proven malignancy, and history of alcohol or drug abuse.
Patients were randomly assigned by the envelope method to either the MLC group or the conventional LC group. A detailed written informed consent was obtained from every patient, and the study was approved by the local ethics committee. The patients were only told which operation they had undergone after a period of 24 hours during which the pain scores were obtained. All the operations were performed by the same experienced surgeon or by trainees under his direct supervision.
The primary end point of the study was to assess the difference in postoperative pain at 24 hours postoperatively. Secondary end points were assessment of the pain scores at other time points during the first 24 hours postoperatively, the rate of conversion to LC and open surgery, mean operating time measured from the first incision until the last suture of the skin (“skin to skin time”), occurrence of intraoperative complications (such as bile leakage, liver trauma, trauma of the biliary tract, and hemorrhage), postoperative analgesic requirements, hospital stay, postoperative complications, and satisfaction of the patient with the cosmetic result.
Surgical technique
The same protocol of anesthesia was applied to all patients. The patients received 1 g of paracetamol and 75 mg of diclofenac during the operation, provided there was no formal contraindication; otherwise 100 mg of tramadol was given as alternative. For MLC, a 10-mm umbilical incision was made, and a 12 mm Hg pneumoperitoneum was created via a Veress needle. A 10-mm cutting trocar was inserted followed by the introduction of a 30° 5-mm laparoscope (Opus Medical, Kuringem, Belgium). The other three trocars were placed under direct visualization of the laparoscope, forming a triangle on the right hypochondrium, according to the layout displayed in Figure 1. Two 2.8-mm cutting trocars (Opus Medical) and a 5-mm cutting trocar were used. All the wounds were previously infiltrated with ropivacaine (7.5 mg/mL). The laparoscope was switched to the 5-mm port. The two 2.8-mm ports accommodated the 2.5-mm graspers (Opus Medical) that are used for traction, and the hook-dissector was used through the 10-mm umbilical working port. The dissection was performed according to the protocol elsewhere described. 18 Before the dissection was begun, ropivacaine 7.5 (mg/mL) was squirted at the diaphragmatic dome to obtain a better postoperative analgesia.19,20 In total, 20 mL of ropivacaine (7.5 mg/mL) was used for the abdominal wall and diaphragm. Both the cystic duct and the cystic artery were sealed with two 10-mm clips and afterwards transected. A systematic cholangiogram was performed on every patient. The gallbladder was removed via the umbilical port with an endobag if the surgeon considered that there was a high risk of rupture or if a difficult extraction was expected. A drain with negative pressure was placed at the end of the surgical procedure in the area of dissection, through the 5-mm port, and was removed before discharge of the patient, provided there was no bile leakage. On completion of the procedure, special attention was given to letting the carbon dioxide of the pneumoperitoneum escape in order to avoid shoulder pain. The 10-mm incision was closed using a fascial absorbable suture, interrupted subcuticular absorbable sutures, an intradermal continuous nonabsorbable suture, and surgical strips. The 5-mm incision was closed with an intradermal nonabsorbable suture and strips. The 2.5-mm incisions were closed only with surgical strips.
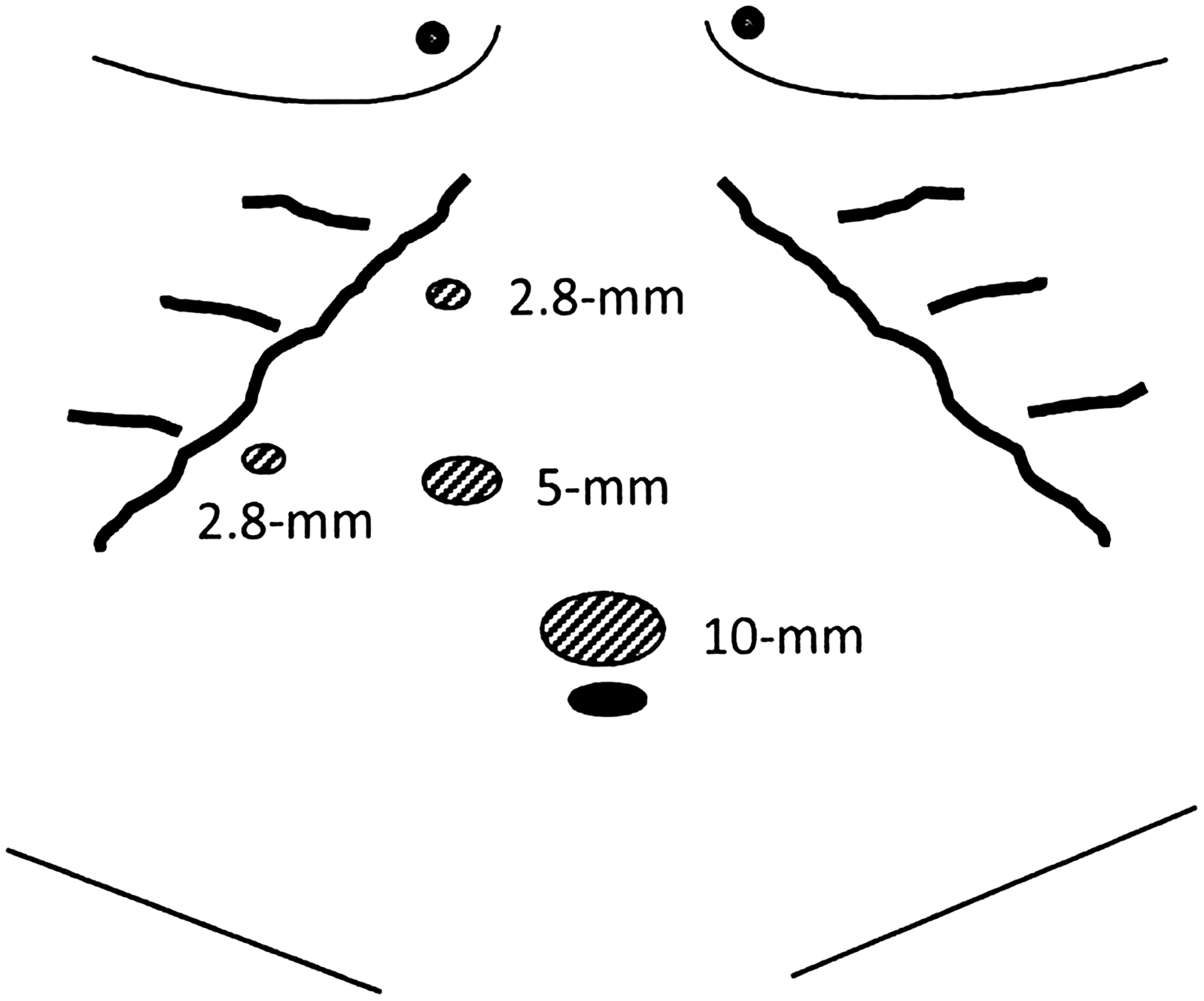
Position of the trocars in the abdomen for the mini-laparoscopic cholecystectomy.
Conventional LC was performed following the above-mentioned principles. A 10-mm 30° laparoscope (Karl Storz, Tuttligen, Germany) was used through the umbilical 10-mm trocar along with two 5-mm ports in the epigastrium and right hypochondrium for retraction of the gallbladder with atraumatic graspers. A 10-mm working port was placed in the left hypochondrium through which 10-mm clips were applied to seal the cystic duct and cystic artery. The patients received no routine postoperative analgesia. Analgesia was provided only on demand with a sequence of paracetamol, diclofenac, tramadol, and piritramide according to an increasing degree of the pain.
Pain assessment and follow-up
The degree of postoperative pain was assessed by a surgical trainee or nurse, using a numerical rating scale, ranging from 0 (no pain) to 10 (worst possible pain). Assessments were made at 1 hour postoperatively at the recovery room and subsequently at 3, 6, 12, and 24 hours postoperatively on the ward. A clear distinction was made between incisional pain and general abdominal pain, both at rest and when coughing. Pain related to the postoperative abdominal drain was not specifically asked about. A follow-up consultation at 1 month postoperatively was planned for each patient. In addition to documenting any late complication or adverse reaction, the cosmetic result was assessed by asking the patient the degree of satisfaction with the scars according to a scale that ranged from 0 (not satisfied) to 10 (very satisfied).
Statistical analysis
Based on preliminary data, a total sample size of 50 patients was required to detect a reduction of 40% in the pain score at 24 hours postoperatively with MLC, with a power of 80% and a Type I error of 5%. 3 Two-tailed P<.05 was considered significant. Data were analyzed on the basis of intention to treat using the IBM SPSS version 19.0 statistical software (IBM Corp., Armonk, NY). For quantitative data, Student's t test was used in the case of normal distribution of the data, and the Mann–Whitney U test was used for non-normal distributed data. Categorical data were compared by Fisher's exact test.
Results
Between March 2010 and December 2011, 41 patients were included in the trial: 23 patients underwent an LC, and 18 patients underwent a MLC. There was no difference between the two groups in terms of age, sex, or body mass index (Table 1). A systematic intraoperative cholangiography was performed successfully in every patient. The mean operating times were comparable in the two techniques (42 minutes versus 45 minutes, P=.386) (Table 1). Two cases of choledocholithiasis were detected in 2 patients from the LC group despite normal preoperative findings, and postoperative endoscopic retrograde cholangiopancreatography (ERCP) was performed during the same hospitalization. The 2 patients had an uneventful recovery. Major complications such as bile leakage, liver trauma, trauma of the biliary tract, or hemorrhage were not encountered in either group of the study. There were 5 cases of intraoperative gallbladder perforation in the MLC group and 2 cases in the LC group. We had no conversions to an open procedure, but in 3 patients from the MLC group we had to partially convert to LC, by substituting a 2.8-mm trocar by a 5-mm trocar, because of difficulties in exerting enough traction on the tissues with the fragile mini-instruments. The median pain scores for incisional and general abdominal pain, evaluated by the numerical rating scale during the first 24 hours after the procedure, at rest and while coughing, were not statistically different at any time point when comparing the two techniques, as shown in Figures 2–5. The analgesic requirements and the duration of hospital stay were analogous in the two groups (Table 2). Most patients were discharged the morning after the operation. Clinical follow-up after 1 month was obtained for 28 patients (68%). All the patients were very satisfied with the cosmetic result after 1 month, and there was no significant difference between the two techniques (Table 2). There were 3 cases of minor wound infection at the umbilical incision detected at the follow-up consultation: 2 in the LC group and 1 in the MLC group.
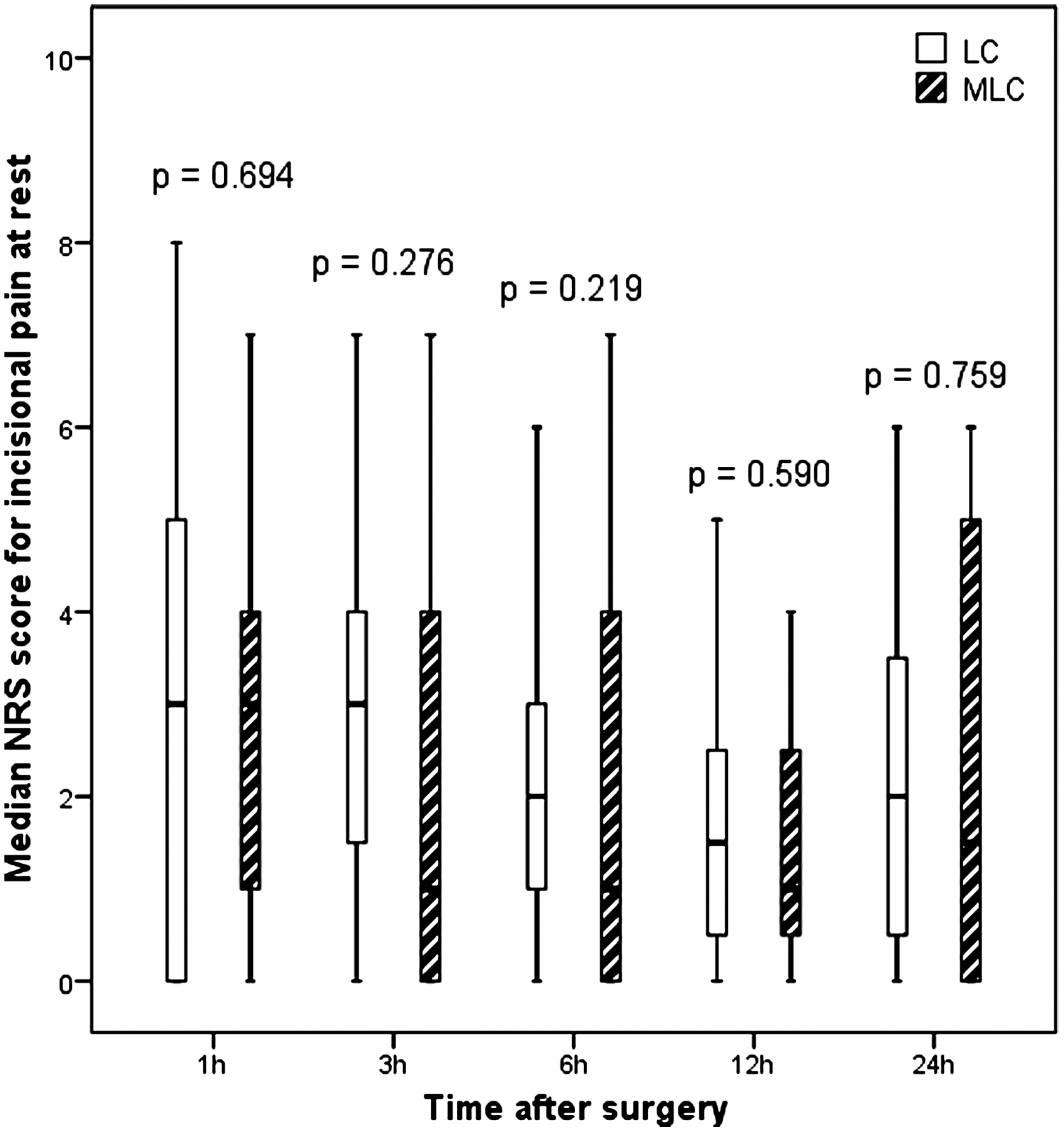
Median pain score on the numerical rating scale (NRS) for incisional pain at rest at 1, 3, 6, 12, and 24 hours postoperatively, comparing conventional laparoscopic cholecystectomy (LC) and mini-laparoscopic cholecystectomy (MLC). No significant difference was detected using the Mann–Whitney U test.
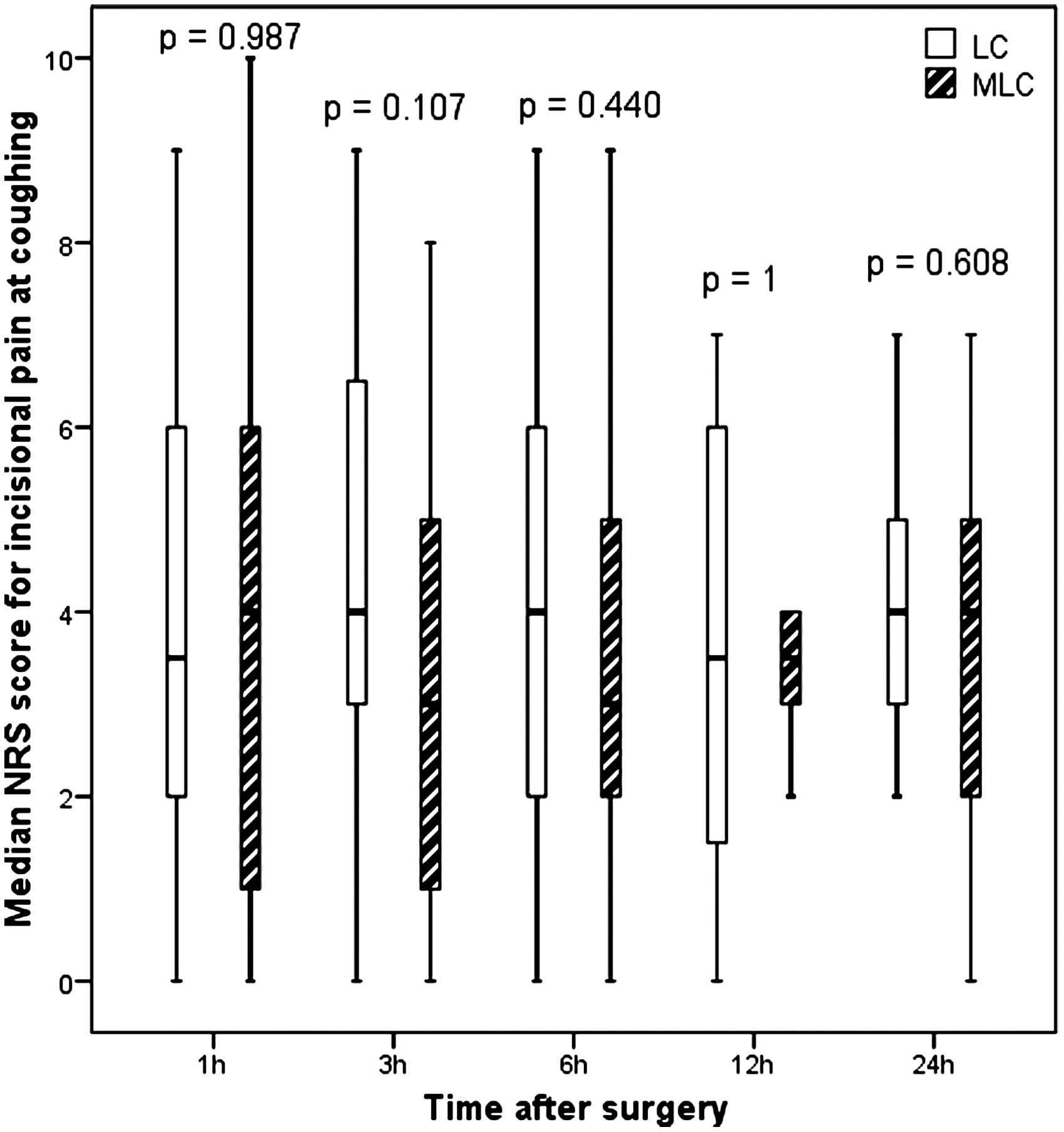
Median pain score on the numerical rating scale (NRS) for incisional pain at coughing at 1, 3, 6, 12, and 24 hours postoperatively, comparing conventional laparoscopic cholecystectomy (LC) and mini-laparoscopic cholecystectomy (MLC). No significant difference was detected using the Mann–Whitney U test.
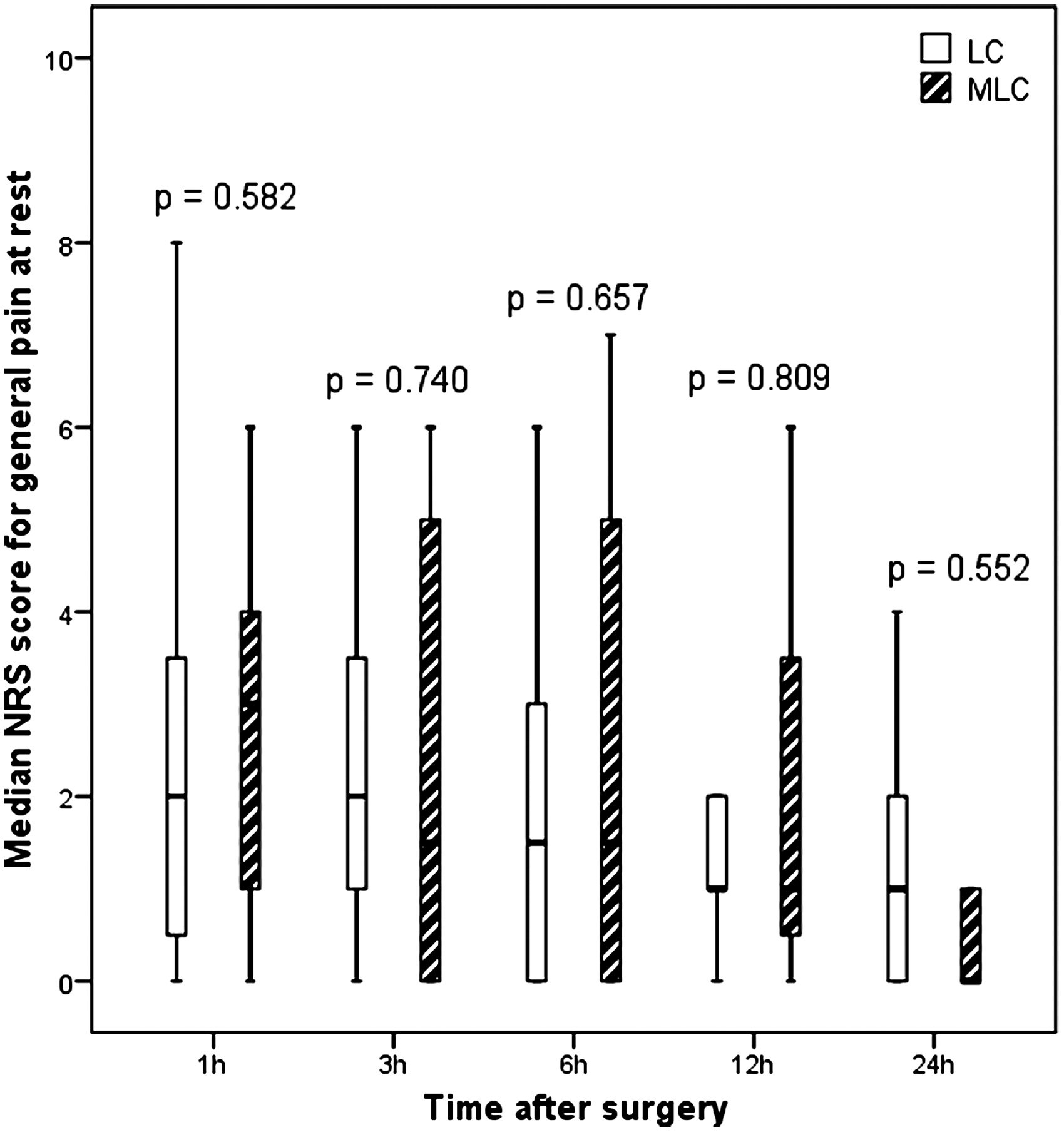
Median pain score on the numerical rating scale (NRS) for general pain at rest at 1, 3, 6, 12, and 24 hours postoperatively, comparing conventional laparoscopic cholecystectomy (LC) and mini-laparoscopic cholecystectomy (MLC). No significant difference was detected using the Mann–Whitney U test.
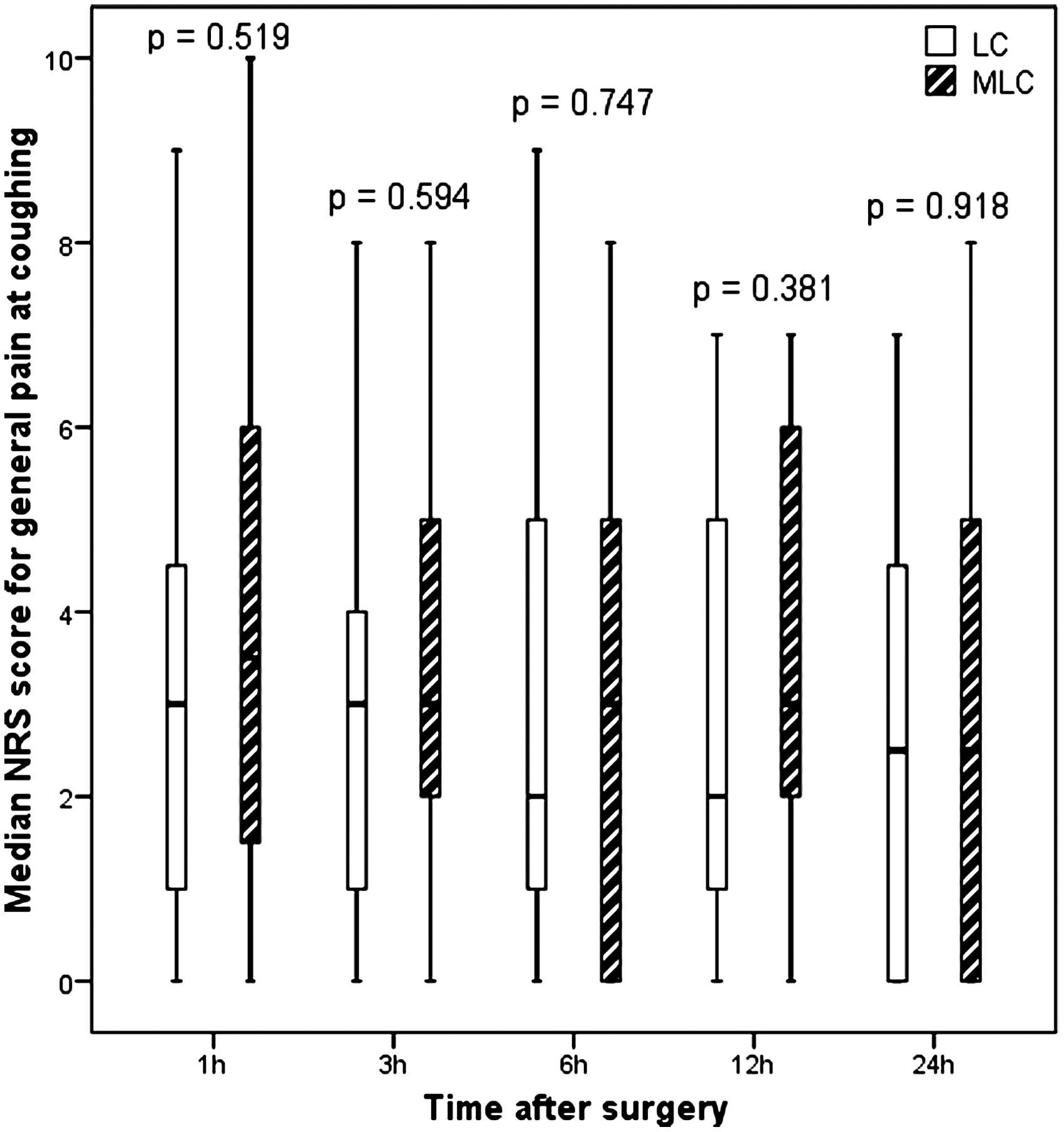
Median pain score on the numerical rating scale (NRS) for general pain at coughing at 1, 3, 6, 12, and 24 hours postoperatively, comparing conventional laparoscopic cholecystectomy (LC) and mini-laparoscopic cholecystectomy (MLC). No significant difference was detected using the Mann–Whitney U test.
Data are mean±standard deviation values or number (%) as indicated.
By Student's t test and Fisher's exact test.
BMI, body mass index; LC, conventional laparoscopic cholecystectomy; MLC, mini-laparoscopic cholecystectomy.
Data are median values (interquartile range).
By Mann–Whitney U test.
Patient-rated cosmetic score after 1 month, on a scale of 0=not satisfied to 10=very satisfied.
LC, conventional laparoscopic cholecystectomy; MLC, mini-laparoscopic cholecystectomy.
Discussion
In this trial we prospectively assessed the standard implementation of MLC in our hospital for selected patients who undergo an elective cholecystectomy. We could not show any statistically significant intergroup difference between MLC and LC regarding our primary outcome measure, which was the postoperative pain evaluated at 24 hours. Other end points such as pain scores at other time points, operating time, analgesic requirements, duration of the hospital stay, or the satisfaction of the patient with the cosmetic result did not differ.
This study is underpowered because only 41 patients were recruited, therefore failing to achieve the calculated sample size of 50 patients in the course of 22 months. Several conditions contributed to the underpowering of this study. First, we had a slower inclusion rate of patients than expected. Second, our sample size calculation was based on a study with very favorable results that showed a decrease of 40% in the pain score between LC and MLC. 3 However, when analyzing our preliminary results it became obvious that if we were to demonstrate a difference in pain score between the two techniques, it would be marginal. This fact, combined with the transfer of the main investigator to another hospital to continue his residency program, led us to end the study prematurely because the quality of the assessment of the parameters and follow-up of the patients would be logistically more difficult to achieve.
Our results may seem to show that there is little improvement by introducing MLC. However, it has to be taken into account that most of the patients undergoing LC already have an uneventful postoperative course with little postoperative pain and are often discharged on the same day of the surgery. 2 In all our patients, the wounds are infiltrated with ropivacaine, which is also used at the diaphragmatic domes. These measures, together with the release of the carbon dioxide of the pneumoperitoneum at the end of the operation, already diminish the pain in LC. According to Thakur et al. 2 the measurement of the pain scores and use of postoperative analgesia are not as important in the assessment of MLC as the evaluation of other key outcomes such as conversion to LC or open cholecystectomy, which indicate failure of technique, or the occurrence of adverse events such as biliary injury.
Several randomized controlled trials have already compared MLC with LC, mostly in an elective setting (Table 3), and produced mixed results. None of the studies is multicentric, and only three are double-blind trials.4,7,13
ITT, intention-to-treat analysis; LC, laparoscopic cholecystectomy; MLC, mini-laparoscopic cholecystectomy; NE, not evaluated; OC, open cholecystectomy; PC to LC, partial conversion to conventional laparoscopic cholecystectomy (placing one extra trocar or increasing the diameter of one port); POD, postoperative day; VAS, visual analog scale; VRS, verbal rating scale; X, no difference.
In general, when reading the literature on the subject, there is no difference in the operating time between MLC and LC. This is confirmed by our results. However, in three studies the operating time was longer with MLC.4,10,11 In the majority of these studies, two scopes were required to complete the procedure: a 10- or 5-mm laparoscope for most of the dissection of the gallbladder and a mini-scope to be able to clip the cystic duct and cystic artery as well as to extract the gallbladder from the abdominal cavity. The clips have to be applied through at least a 5-mm port, and visualization of the gallbladder is necessary while the extraction is being performed through the larger port. The mini-scope does not provide the same optic resolution, brightness, or width of operative field for the surgeon to perform the entire operation safely. 11 Huang et al. 11 suggested the preparation of two sets of cameras and light sources in order to save time with the permutation of the cameras. In our study, like in three other studies,5,11,13 a 5-mm scope was used during the whole procedure, avoiding time-consuming camera switches.
Concerning postoperative pain, there were three studies that could not show any benefit for the MLC group.6,8,9 In the other studies, there was no uniformity of results concerning the advantage of MLC (Table 3). Depending on the study, there is a subcategory of pain that is diminished at some time point or port. In the study from Sarli et al., 12 the mean visual analog scale pain scores in the MLC group were consistently lower at different time points until 24 hours postoperatively, when the evaluation stopped. But looking at the first study from Bisgaard et al., 4 there is, in the first 3 postoperative hours, less overall pain during mobilization and less incisional pain at rest and during mobilization, as measured by the verbal rating scale, although there is no statistical difference between the visual analog scale pain scores during the same time period. In the second study from the same group 7 they stated that incisional pain was decreased in the first postoperative week and significantly decreased in the first postoperative day when comparing the cumulative patient's self-reported incisional pain scores on a visual analog scale. Nevertheless, when comparing the median pain scores of incisional and overall pain at each time, there was no significant intergroup difference. We used a postoperative abdominal drain routinely like in three other studies.5,9,12 The use of a drain will have an influence in the postoperative pain, causing more discomfort and therefore probably leading to higher pain scores, but like in the other three studies5,9,12 we did not specifically ask for the pain score at the drain site. Because the drain is used in both groups systematically and removed by every patient before discharge, any difference in the pain scores between the groups will result from the differences in the operative technique and not because of the more frequent selective use of a drain in one of the groups.
The analgesic requirements were not reduced after MLC in five studies, similar to our study (Table 3). The other studies that do show a diminished intake of analgesics after MLC refer most of the time only to parenteral analgesia, and the benefit seems quite minimal or simply not clear (Table 3). The protocol of anesthesia, the injection of local anesthetic at the port sites and intra-abdominally, or even the possibility of providing routine postoperative analgesia differs according to the study. In our study we did not provide any standard postoperative analgesia. This interstudy heterogeneity makes it difficult to compare the analgesic requirements and pain scores among studies. From our point of view, with the already benign postoperative course of the patients after LC, any possible advantage in the MLC group becomes even more difficult to demonstrate if standard postoperative analgesia is provided.
In our study, there were no conversions to open cholecystectomy. In the MLC group there were 3 patients partially converted to LC (17%) because of inadequate grasping with the mini-instruments. Partial conversion to LC occurred in three studies,6,7,9 at a rate varying from 3.3% to 33%. In Table 3 we can see that there were conversions from MLC to open cholecystectomy in four studies3,6,7,12 in up to 11% of the cases. In this last study, there were 2 cases of biliary injury that required conversion to open cholecystectomy. Conversions to LC were more common (Table 3), with rates as high as 24%.8,13 The study from Bisgaard et al. 4 from 2000 was ended prematurely because of an unacceptable high rate of conversion to LC (38%). In the majority of the studies, there was no intention-to-treat analysis, as the cases of conversion were excluded from the trial.4,6,7,8,11,13
In the present study we did not record major complications. In the study from Bisgaard et al. 7 from 2002, 1 case of re-admission because of pancreatitis was described that was treated with ERCP for extraction of a stone in the common bile duct. Sarli et al. 12 stated that it remains undetermined whether or not cholangiography can be performed during MLC with the same safety and ease as in traditional LC. We performed a systematic cholangiography in every patient of the trial without finding specific technical difficulties or prolonging the operating time. Two cases of choledocholithiasis were detected in the LC group, and a postoperative ERCP was performed during the same hospitalization without the occurrence of complications. Sarli et al. 12 described 1 case of re-intervention in the MLC because of bile leakage.
The studies in Table 3 were performed in elective patients with the exception of the study from Huang et al. 11 that also included patients with acute cholecystitis. The selection criteria among the studies differed. Alponat et al. 8 excluded 14 patients from the trial at the first laparoscopic exploration because of the presence of an inflamed gallbladder or dense adhesions, and even so there was a conversion rate from MLC to LC of 23%. How much would the conversion rate be if those 14 patients were not excluded from the study? A more recent randomized controlled trial by Hsieh 14 has suggested that the results for early operation of acute cholecystitis with MLC are as good as those of LC.
In various trials5,7,8,10,12 the patients were more satisfied with the cosmetic result after MLC. However, cosmesis tends to be a subjective evaluation that is influenced not only by what the patient considers to be a reasonable result, but also by the expectations they have towards the new technique. Cheah et al. 3 evaluated the size of the scars after 2 weeks, noting that they were significantly smaller after MLC. In the study from Novitsky et al. 13 the cosmetic result after MLC was superior according to the evaluation of both the patients and study nurses. In our study, the patients who underwent MLC and LC were both very satisfied with the cosmetic result, resulting in patient-rated scores of 9.75 and 9, respectively. Despite the fact that the cosmetic score was slightly higher in the MLC group, we could not show any statistically significant difference. In our subjective opinion, the cosmetic result was significantly superior after the punctiform 2.8-mm incisions that were only closed with surgical strips. Because it would take a much greater logistic organization to implement a double-blinded study, with objective evaluation of the cosmetic result, we decided to merely assess the patient-rated evaluation of the cosmesis.
The possibility of improving the surgical results of cholecystectomy after MLC, with reduction of postoperative pain and better cosmetic results, is advocated in the review article by Hosono and Osaka. 15 The review by Sajid et al. 16 shared the same conclusions but highlighted the longer operating time and higher conversion rate with MLC. In the review by McCloy et al., 17 the limited improvements in surgical outcomes after MLC are emphasized, at the cost of higher conversion rates. A recent meta-analysis by Thakur et al. 2 stated potential advantages of MLC such as reduced pain and improved cosmesis, which can be jeopardized if there is frequent failure of the technique due to conversion.
Our study clearly reports that MLC is feasible and safe in elective patients. There are many randomized controlled trials on the topic (Table 3) that do not show evident advantages after MLC. The fact that most trials lack an intention-to-treat analysis must not be forgotten, as well as some dubious study designs, the marginal superiority in postoperative pain scores and analgesic requirements, and, most importantly, the existence of conversions (also to the open procedure) and complications in a benign procedure such as an LC in elective patients. It is not surprising that the reviews and meta-analyses that compare MLC and LC2,16,17 speak of possible surgical advantages but alert to the frequent failure of the technique and risk of conversion.
In conclusion, performing MLC according to a highly standardized technique with systematic intraoperative cholangiography did not take longer to perform than LC, nor was it associated with adverse events or a high conversion rate. Despite causing smaller surgical wounds, MLC showed no statistically significant improvements in postoperative pain and did not lead to a greater patient satisfaction with the cosmetic result. Above all, this trial has proven MLC to be a safe and feasible technique for the treatment of gallbladder disease in elective patients.
Multicenter, double-blind, randomized controlled trials with large sample sizes are necessary to achieve stronger evidence about the possible advantages of MLC in the treatment of gallbladder disease. Perhaps the difference in postoperative pain scores between LC and MLC is not as prominent as we thought it to be, and therefore we need more patients in larger studies to be able to demonstrate such a difference. Some paramount areas of consideration for the future studies should be the standardization of outcome measures, particularly of pain and cosmetic results, 15 the objective evaluation of the cosmetic results, and intention-to-treat analysis in order to be able to fully appreciate the potential pitfalls of MLC. 2
Footnotes
Acknowledgments
The statistical analysis was performed with the assistance of the Department of Biostatistics of Ghent University Hospital.
Disclosure Statement
No competing financial interests exist.