
Abstract
Abstract
Background:
To explore the value of minimally invasive surgery for the removal of calculus and preservation of the gallbladder with the combination of a hard gallbladder endoscope and a soft choledochoscope.
Patients and Methods:
A retrospective analysis was conducted of the clinical data of 42 patients with cholecystolithiasis who underwent minimally invasive surgery for the removal of calculus and preservation of the gallbladder from April 2009 to April 2011.
Results:
None of the 42 cases had bile flowing from the gallbladder neck tube to the gallbladder lumen after removal of stones in the gallbladder lumen by the hard gallbladder endoscope; all the 42 cases had residual stones in the gallbladder tube when probed by the soft choledochoscope. The numbers of stones range from one to three, while the diameters of the stones range from 0.5 cm to 1.0 cm. In 8 cases, there was one calculus embedded. In 39 cases, the calculi were taken out through the soft choledochoscope, and the gallbladders were preserved successfully; yet the other 3 cases failed to receive surgery to preserve the gallbladder because of calculi embedded in the gallbladder tube, which were finally treated by laparoscopic cholecystectomy.
Conclusions:
A hard gallbladder endoscope combined with a soft choledochoscope for removing calculi and preserving the gallbladder in laparoscopic microscopic trauma surgery can effectively find residual stones in the gallbladder tube and help to increase the rate of complete removal of calculi and preserving the gallbladder.
Introduction
Patients and Methods
Subjects
All of the 42 cases in the study group had gallbladder calculi. Of the patients, 34 were male, and 8 were female, with an average age of 35 years (range, 24–45 years). Among these patients, 4 cases had no symptom, 20 cases had atypical upper gastrointestinal symptoms, and 18 cases had biliary colic history. B-mode ultrasonography showed 17 cases had only one stone, with 10 cases in the neck of gallbladder; 5 cases had conspicuous inlay, 23 cases had several stones (less than 10), and 2 cases had more than 10 stones.
Operative equipment
The operative equipment used included a laparoscope operation camera system and mini-laparoscope from Karl Storz, CHiAO hard gallbladder endoscope from Hawk Endoscopes Co. (Hangzhou, China) (Fig. 1), a net for removal of stones, a biopsy clamp, a calculus suction box for draining stones, and a soft choledochoscope.
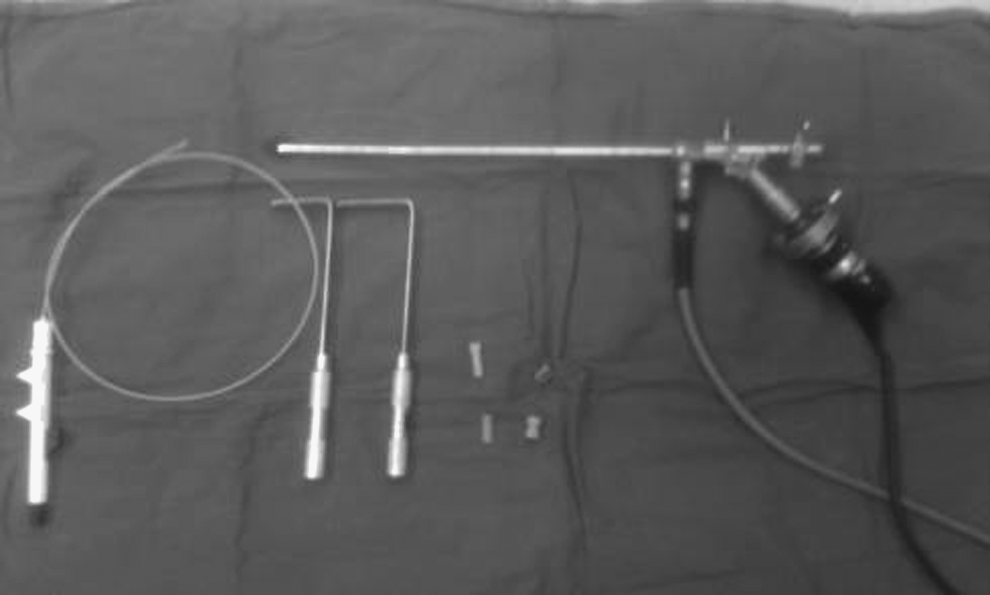
Bridge hard gallbladder endoscope and its accessories.
Operative methods
Endotracheal intubation was performed with the patient under intravenous balanced general anesthesia in all cases. The incision was made 0.6 cm next to the navel. Pneumoperitoneum was induced by penetration of the aeroperitonia needle. Then a trocar was implanted, and a mini-laparoscope was used to explore whether the gallbladder and extrahepatic biliary tract were abnormal and to define the position of the gallbladder. A 2.0-cm incision was made under the right rib edge near to the fundus of the gallbladder, and a 10-mm trocar was implanted. The fundus of the gallbladder was pulled outside the abdominal wall with laparoscope forceps, and 1.0 cm was cut off (the incision can be adjusted according to the size of the gallbladder). After bile was suctioned, the gallbladder was explored with a hard gallbladder endoscope under low pressure water injection; stones that were >0.5 cm in diameter were removed by the net for stone removal versus stones that were <0.5 cm in diameter were drained out through the calculus suction box. After stones were removed from the gallbladder lumen, if the stones in the gallbladder tube were found not to be taken out or the bile was not seen squirting from the gallbladder tube when the gallbladder tube was explored with the hard gallbladder endoscope, we switched to the soft choledochoscope to probe the gallbladder neck tube and remove residual calculi from the gallbladder neck tube completely. The cases whose stones could not be completely removed were treated by laparoscopic cholecystectomy instead.
Results
After gallbladder lumen stones were removed in 42 cases, 18 cases exhibited residual stones in the gallbladder tube, and 8 cases had calculi embedded conspicuously when viewed from the side view of the hard gallbladder endoscope. Thus all the stones could not be taken out. Sixteen cases did not have bile flowing from the gallbladder neck tube to the gallbladder lumen when probed repeatedly. When explored again, this time with a soft choledochoscope, all 42 cases had residual calculi in the gallbladder tube, with the number of the stones ranging from one to three, the diameter of which ranged from 0.5 cm to 1.0 cm; 39 cases had calculi taken out through the soft choledochoscope, and the gallbladder was successfully preserved. Three cases had to be treated finally by laparoscopic cholecystectomy because of calculi embedded in the gallbladder tube. Among the 39 cases in which the gallbladder was successfully preserved, 16 cases had one stone, but 23 had several stones, the number of which ranged from 1 to 18 and the diameter ranged from 0.2 cm to 2.5 cm. When re-examined with B-mode ultrasonography at 3 months after operation, all 39 cases were found not to have recurring stones in the gallbladder and bile duct.
Discussion
As medicine continuously improves, with the recognition of the importance of gallbladder function and the harmful effect on the human body after cholecystectomy, more and more experts sanction conserving gallbladder function. 1 With minimally invasive technology like the laparoscope and choledochoscope widely used in clinics, there is also a revolutionary change in the technology of preserving the gallbladder. In the past, it was very problematic to touch the stones by hand just as it was impossible to view the internal gallbladder directly in fistulation of the gallbladder and removal of calculi. Omitted calculus, especially muddy stone, has become the main reason for the high recurrence rate of calculus. Using a laparoscope combined with a choledochoscope for removal of the calculus and preservation of the gallbladder not only can fully reflect the characteristics of minimally invasive technology, but also greatly reduces the rate of residual stones by watching the true face of the mucosa of the gallbladder lumen directly with an endoscope and taking the calculus and polyp completely.2,3 We have carried out laparoscopy combined with hard gallbladder endoscopy for the removal of calculus and preservation of the gallbladder in our hospital beginning in April 2009, on the basis of which we used a hard gallbladder endoscope combined with a soft choledochoscope for the removal of calculus and preservation of the gallbladder under the laparoscope in patients who had residual or inlaid calculus, which yielded good results.
The hard gallbladder endoscope could observe the mucosa of the gallbladder at a close distance and magnify it 8–10 times. Its image is stable and clear, and it also helps to discover minimal diseases easily and take out the stones with a diameter of >0.5 cm but <2.5 cm in the gallbladder lumen smoothly through the net for stone removal. The unique draining box that goes with the hard gallbladder endoscope could conveniently and quickly take out those calculi with a diameter of <0.5 cm or sand stones. It is also of clinical significance to clear away stones from the gallbladder mucosa and bile mud or floccules on the surface of gallbladder mucosa. 4 The hard gallbladder endoscope has a biopsy clamp and a coagulation clamp that give it a particular advantage when observing and treating polyps of the gallbladder; its endoscope body has an inlet hole and a suction hole so that it could easily adjust the pressure of the gallbladder lumen and is not likely to lead tiny stones (diameter, <4–6 cm) into the common bile duct as the internal pressure of the gallbladder is too great. Residual stones in the gallbladder duct usually cannot be observed or taken out due to the rigidity of the gallbladder endoscope, as well as the short diameter and anatomic feature of the gallbladder duct that is separated from the gallbladder body by Heistera lamella. Stones were taken out of the gallbladder lumen smoothly during operation in all 42 cases, of which 18 cases had residual stones in the gallbladder lumen found just from the side view by the hard gallbladder endoscope, 8 cases had calculi embedded evidently in the gallbladder duct because the extremity of the hard gallbladder endoscope cannot swerve to take out gallbladder duct calculi, and the remaining 16 cases were changed to use of the soft choledoscope for exploration because bile was not found flowing from the gallbladder neck tube to the gallbladder lumen.
A characteristic of the soft choledochoscope is the good activity performance of its extremity: it could observe every corner of the inner wall of the gallbladder, and it is beneficial to adjust to different angles so that calculi can be taken from different positions. 5 It could smoothly enter the gallbladder tube and directly observe the entrance of the gallbladder tube to the common bile duct. The soft choledochoscope has the advantage in judging whether there has been bile circumfluence and helping to take out the calculi embedded in the gallbladder tube or the gallbladder neck if there are calculi in the gallbladder duct 6 ; the hard gallbladder endoscope cannot do this. After it was found that the stones in the gallbladder tube cannot be taken out or the bile was not observed squirting from the gallbladder tube, the 39 cases were changed to using the soft choledochoscope to explore and had the stones in the gallbladder tube taken out smoothly. This fully reflects the advantage and significance of the soft choledochoscope in minimally invasive surgery for the removal of calculus and preservation of the gallbladder. But, the soft choledochoscope is not equal to the hard gallbladder endoscope in dealing with larger stones, mucosa stones, and polyps in the gallbladder tube because of its narrow-vision scope and accessory equipment. As the space of the gallbladder tube is larger, the soft choledochoscope does not need the increase of the pressure of pumping water like in the bile duct, which could avoid stones dropping into the common bile duct caused by higher water pressure. When re-examined with B-mode ultrasonography in 3 months after operation, none of the 39 cases was found to have recurring stones in the gallbladder and bile duct. The results indicated that the hard gallbladder endoscope combined with the soft choledochoscope is safe and feasible for clinical removal of calculus and preservation of the gallbladder.
The hard gallbladder endoscope and soft choledochoscope have their own characteristics and advantages for the removal of calculi and preservation of the gallbladder. The combination of the two would be helpful to maximize favorable factors and minimize unfavorable ones for the removal of calculi and preservation of the gallbladder and to efficiently discover residual calculi of the gallbladder tube, increase the rate of removing calculi completely, and augment the rate of preserving the gallbladder. There exists a broad prospect in clinical application.
Footnotes
Disclosure Statement
No competing financial interests exist.