
Abstract
Abstract
Background:
Single-port laparoscopic cholecystectomy (SPLC) has been one of the hottest topics in minimally invasive surgery. Various techniques have been described, but the search for better techniques and equipment still continues. The aim of this study is to share a new retraction technique and the results in 27 patients.
Patients and Methods:
Between May 2010 and May 2011, 27 patients underwent SPLC with the presented technique. The data related to the operative and postoperative measures were collected prospectively. Operation time, pain score (visual analog scale) in the first 24 hours after the operation, and length of hospital stay were recorded by an independent nurse.
Results:
Twenty-seven SPLCs were performed. Indications were symptomatic gallstone disease or gallbladder polyps without active inflammation. Mean operation time was 45.7 minutes (range, 30–80 minutes). In none of the patients was introduction of an additional port or conversion to conventional laparoscopic cholecystectomy needed.
Conclusions:
The endoloop technique can be used to overcome retraction problem while preventing spillage of bile and reducing crowding of instruments with a practically invisible scar in selected patients.
Introduction
The most important issue in SPLC is maintenance of the critical view of safety described in 1995. 18 The crowding of hand instruments and the insufficient retraction of the gallbladder interfere with establishment of the critical view. Long and flexible camera systems and long articulated instruments have been developed to overcome this problem. However, there is still an ongoing search for optimal technique and instruments. Our endoloop technique arose after the initial 17 cases of SPLC as a result of the search for an alternative method to retract the gallbladder and to reduce the number of instruments introduced through the multichannel port while preventing spillage of bile. Herein we report the endoloop technique and results in 27 patients.
Patients and Methods
Between May 2010 and May 2011, SPLC was performed in 27 patients with this technique. The data were collected prospectively. All of the operations were performed by the same surgical team experienced in advanced laparoscopic surgery.
Patients with symptomatic gallstone disease without active inflammation or gallbladder polyps and who demanded SPLC were included in the study. The patients signed an informed consent before the operation. The exclusion criteria were as follows: (a) acute cholecystitis, cholangitis, or common bile duct stones, (b) biliary pancreatitis, (c) cirrhosis, (d) bleeding disorders, (e) suspicious or proven malignancy, (f) American Society of Anesthesiologists (ASA) score of >II, (g) patients with a history of abdominal operation other than cesarean section, (h) mentally ill, (h) pregnant, and (i) patients who rejected SPLC or refused to sign the informed consent.
Surgical technique
The patient was placed in a modified Lloyd Davies position. The surgeon worked between the legs of the patient with the first assistant on the right side of the surgeon and the scrub nurse on the left.
A vertical incision with hooked ends (a ying-yang incision) through the umbilicus was made. After the peritoneal cavity was intruded into with the open technique, a multichannel port was introduced. Two types of multichannel port systems were used in the operations: a Covidien SILS™ port (Covidien, Inc., Norwalk, CT) or an Olympus TriPort™ (Olympus Medical Systems Corp., Tokyo, Japan).
A 5-mm HD EndoEye™ video laparoscope integrated with the EVIS EXERA II system (Olympus Medical Systems) was used. The fundus of the gallbladder was held with a grasper. An endoloop (Surgitie™; Autosuture™, Tyco Healthcare United States Surgical, Norwalk) was placed through a 5-mm port in the system. The fundus was strangulated with the endoloop (Fig. 1). A puncture was made in the 8th or 9th intercostal space medial to the anterior axillary line to introduce an endoclose. The free end of the ligature was pulled out through the abdominal wall between the ribs with the aid of the endoclose (Fig. 2). The gallbladder was retracted with the endoloop, and the triangle of Calot was exposed (Fig. 3).
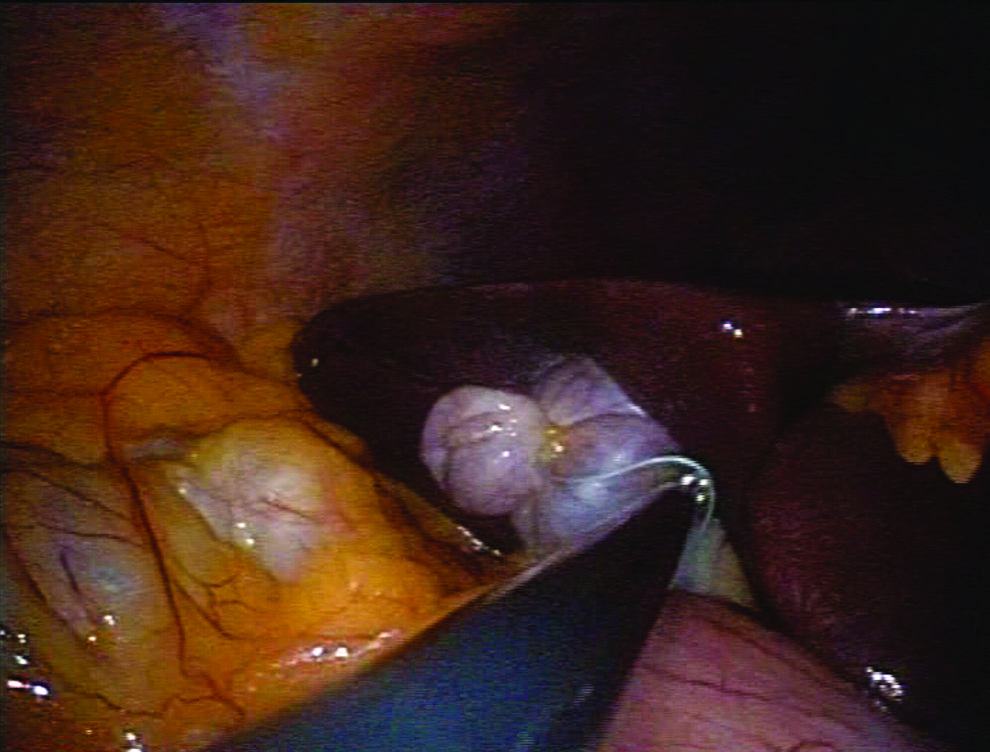
Strangulation of the fundus of the gallbladder with an endoloop.
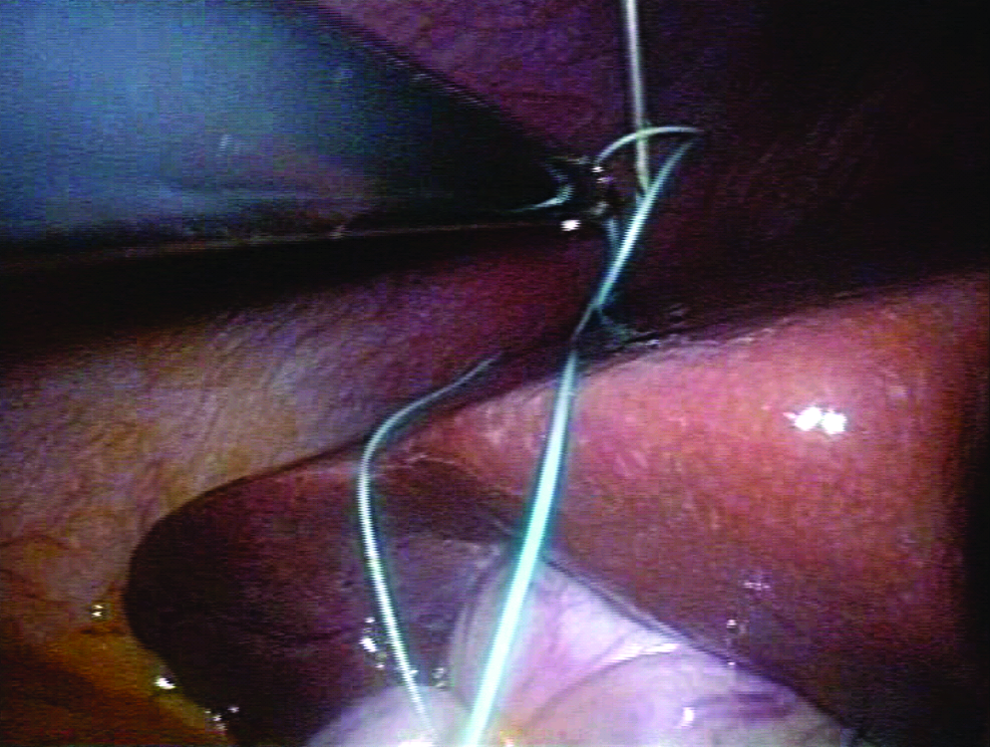
The free end of the ligature is retrived through the abdominal wall.
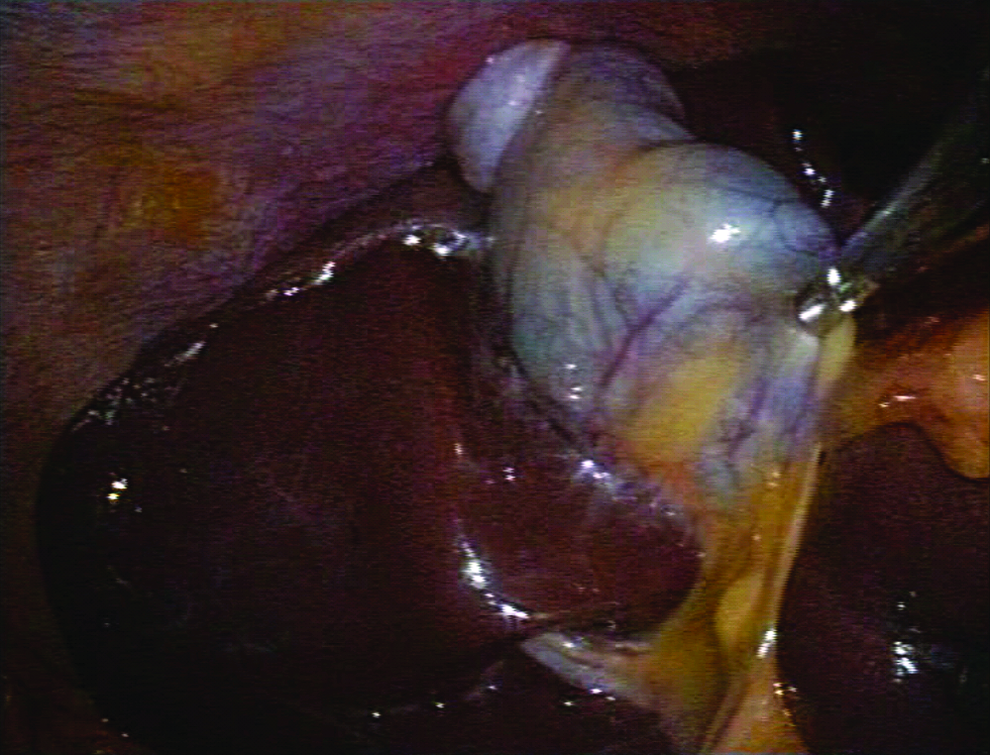
Exposure of the triangle of Calot.
The operative dissection of the gallbladder was similar to conventional laparoscopic cholecystectomy. Once the gallbladder was retracted, dissection was done until the cystic duct and the cystic artery was clearly identified. The artery was clipped once, and the cystic duct was clipped three times before bisection. Cholecystectomy was performed in a retrograde fashion. Bile leak or bleeding from the gallbladder bed was meticulously controlled just before the last move to separate the gallbladder from the liver. The bleeding points were coagulated with electrocautery in the spray mode. After aspiration of the surgical field—if necessary—cholecystectomy was completed, and the specimen was retrieved with the ligature through the umbilicus with the port system. After desufflation of the abdominal cavity the incision was closed with Vicryl™ (Ethicon, Somerville, NJ) and polypropylene sutures in two layers.
Results
In total, 27 patients were operated on with the same technique. There were 25 females and 2 males. Mean age was 39.1 years (range, 26–58 years). The indications were symptomatic gallstone disease in 25 patients and gallbladder polyps in 2 patients. All the patients had ASA scores of I–II and a body mass index below 30 kg/m2.
The operation time ranged between 30 and 80 minutes with a mean of 45.7 minutes. Mean pain score according to the visual analog scale in the first 24 hours was 4.2 (range, 2–8). Mean hospital stay was 1.14 days (range, 1–3 days). None of the patients needed addition of ports, conversion to conventional laparoscopic cholecystectomy, or the open technique. No perioperative cholangiography was performed during these operations.
There were no peri- or postoperative complications, morbidities, or mortalities. No pneumothorax was encountered in any case, and there was no need for postoperative chest X-ray. Median follow-up was 1 week. No wound-related problems like infection were observed. All of the patients were satisfied with the cosmetic result, although 2 female patients were not pleased because of the severe pain they experienced in the umbilical incision.
Discussion
The search for “scarless” and “painless” surgery, patients' demands, and technological drives have resulted in the rise of natural orifice translumenal endoscopic surgery (NOTES™; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) and single-incision surgery. Unlike NOTES, single-incision surgery has met with enthusiasm among those performing minimally invasive surgery.
Various studies about SPLC have been reported, and the search is still ongoing for optimal instruments and methods. The most challenging part of the single-port technique is to expose the triangle of Calot and maintain the critical view for safe dissection.10,14,19,20 Crowding and fencing of hand instruments occur, which interfere with fine movements of the surgeon. Additionally, the necessity to work with the instruments in a crossed-over manner instead of triangulation requires re-coordination of hands and eyes of the surgeon. Long and angled camera systems and articulated hand instruments help to overcome fencing of the instruments to some degree. However, adequate retraction of the gallbladder remains as the most important issue to identify and dissect the cystic artery and the cystic duct for safe clipping. Most commonly, traction suture with a Keith needle,5,15,17,21–23 a mini-loop retractor,9,11,13 or suspension hooks12,24 were used in the literature. The main issue in suspension with traction sutures is the concern that the bile leak from the puncture sites may contaminate the surgical field. There may be an increased risk of bile peritonitis, especially in the presence of acute cholecystitis. Additionally, loss of tension of the gallbladder may adversely affect dissection. Retraction of the gallbladder with a mini-hook retractor is a good technique that prevents perforation of the gallbladder. However, there was a mild criticism that introduction of a mini-hook retractor has made the operation a double-incision laparoscopy. 25 The endoloop technique was developed after 17 initial cases of SPLC performed by the same surgeon to overcome the retraction problem while avoiding spillage of bile. The major issue in this technique is the proper placement of the endoloop around the fundus of the gallbladder.
After strangulation, the gallbladder is retracted craniolaterally. Then, the free end of the ligature is extracted out of the abdominal cavity. Placement of the endoloop is relatively easy for a floppy and pronounced fundus, whereas small and embedded gallbladders create an anatomic challenge. In such cases the fundus should be separated from the liver bed in an antegrade fashion to create a suitable part for placement of the endoloop and strangulation. This maneuver should be carefully performed to prevent perforation of the gallbladder and bleeding from the liver bed. In our series we have to dissect the fundus of the gallbladder to create a suitable part for proper placement of the endoloop in 7 patients. Bleeding from the liver bed occurred in 1 of these patients and was managed successfully without compromising the operation. However, the operation time increased in this patient (80 minutes). In 1 patient the endoloop slid, and we placed another endoloop after we removed the first one. But, this did not lead to failure or complication. This technique has been used safely and successfully in 27 cases and helped to overcome the retraction problem as well as fencing of the instruments.
Conclusions
The endoloop retraction technique is easy to perform and has the following advantages: (a) it is a good substitute for traction sutures; (b) it eliminates the risk of bile peritonitis; (c) if placed properly it provides effective retraction of the gallbladder and eases the establishment of the critical view; (d) it reduces the number of hand instruments, thus decreasing the conflict; and (e) there is no visible scar at the puncture site with an excellent cosmetic result. On the other hand, the potential pitfall is the hindrance of anatomy in patients with embedded gallbladders, which may prevent the proper placement of the endoloop and effective retraction.
Footnotes
Disclosure Statement
No competing financial interests exist.