
Abstract
Abstract
Background and Objectives:
Despite being pioneered by gynecologists, single-incision endosurgery has not been widely reported for the treatment of ovarian and adnexal pathology in neonates, children, and adolescents. We describe our initial experience using single-incision pediatric endosurgery (SIPES) for these indications and discuss advantages and drawbacks.
Subjects and Methods:
All children who underwent SIPES with a preoperative diagnosis of ovarian or adnexal pathology were included in the study. Data on age, operative time, complications, length of hospital stay, and outcomes were collected.
Results:
From January 2010 until January 2012, 19 girls (mean age, 11.4 years; range, 6 days–17 years; weight range, 4.0–90 kg) underwent SIPES procedures for ovarian or adnexal diagnoses, including hemorrhagic/follicular/paratubal cysts (n=8), torsion (n=7), tumor (n=3), and parauterine cyst (n=1). The operations included cyst unroofing (n=4), detorsion and oophoropexy (n=7), (salpingo)oophorectomy (n=5), marsupialization of cyst (n=2), and cyst aspiration (n=1). Median operative time was 42±29 minutes; there were no conversions to conventional laparoscopy or open surgery. Fifteen patients (79%) were discharged within 24 hours after the procedure. There were no peri- or postoperative complications. Histopathology showed hemorrhagic/follicular/paratubal cyst (n=7), necrotic/calcified ovarian tissue after torsion (n=6), cystadenofibroma (n=1), granulosa cell tumor (n=1), and mature teratoma (Grade 0) (n=1).
Conclusions:
SIPES is an excellent alternative to conventional laparoscopy for the treatment of adnexal pathology. Using a single umbilical incision that can be enlarged instead of three smaller trocar sites facilitates the resection and extraction of ovarian masses without compromising cosmesis.
Introduction
SIPES has gained popularity for ablative procedures in many pediatric surgical centers. Our group previously reported on its successful application in a variety of procedures and even in reconstructive surgery.10–12 However, this method has not been widely used for treatment of ovarian or adnexal pathology in neonates and girls.
Therefore, the aim of the current prospective study was to report SIPES for adnexal and ovarian indications in our initial cohort of 19 children. Also, having established the safety of SIPES procedures in many other indications, our interest was to assess feasibility, safety, and advantages and drawbacks in treating ovarian pathology using this new technique.
Subjects and Methods
Data acquisition
After Institutional Review Board approval was obtained, data were prospectively collected in our hospitals on all SIPES procedures for ovarian or adnexal pathology performed from January 2010 through January 2012, including age, weight, indication, operative time, intraoperative complications, introduction of additional trocars, estimated blood loss, postoperative hospitalization time, and histology. Postoperative complications were assessed upon follow-up in our outpatient clinic.
Clinical management and surgical technique
In all patients tumor markers, including alpha-fetoprotein, beta-human chorionic gonadotropin, and lactate dehydrogenase, were preoperatively sent to the laboratory. Five attending surgeons performed the procedures with different fellows and residents, leading to a certain degree of variability in the technique. As previously reported,12,13 entry into the abdomen was accomplished through a ≤2-cm longitudinal incision in the umbilicus. The underlying midline fascia was opened over a length of 1.5–2.5 cm to enter the peritoneal cavity. Two different SIPES devices were used: (1) TriPort™ (Olympus, Center Valley, PA) and (2) a homemade port, using a plastic ring rolled up onto the wrist portion of a surgical glove and then inserted through the umbilical incision site. A 5-mm, 30–45°, 45–50-cm endoscope (from one of several different suppliers) was introduced into the port, and the patient was placed in moderate Trendelenburg position to get maximum exposure of the lower abdomen. With reusable 5-mm standard straight laparoscopic instruments, the adnexa were mobilized, and a straight electocautery instrument was used for unroofing a cyst. If indicated, the pathologic segment was amputated either using electrocautery or a 12-mm endosurgical stapler (Endo GIA™ Universal stapler; Covidien, Mansfield, MA) and removed in a 10-mm endoscopic retrieval bag (Endo Catch™ [Covidien] or Endobag® [Ethicon, Blue Ash, OH]). The capnoperitoneum was deflated, and the fascial incision was approximated with a running 2-0 or 0 polyglactin suture. Finally, the skin incision was closed using interrupted subcuticular 4-0 polyglecaprone sutures, with the central stitches anchored to the fascia in order to invert the umbilicus. In an attempt to lower the number of wound infections, we devised and used a low-cost vacuum dressing to cover the umbilical incision. 14
Results
In a period of 25 months, in total, 19 SIPES procedures for ovarian or adnexal pathology were performed (Table 1). Median age was 11.4 years (range, 6 days–17 years), and median weight was 60 kg (range, 4.0–90 kg). None of the patients had elevated preoperative tumor markers (alpha-fetoprotein, beta-human chorionic gonadotropin, and lactate dehydrogenase). The indication for laparoscopy was severe abdominal pain and cystic adnexal masses with or without sonographically suspected ovarian torsion in 14 children (74%) and ovarian tumor in another 5 children (26%) (Table 1). Intraoperatively, the following procedures were carried out: unroofing of cyst (n=4), detorsion±oophoropexy (n=7), (salpingo)oophorectomy (n=5), marsupialization of cyst (n=2), and aspiration of cyst (n=1) (Table 1).
CAM, cystic adnexal mass; CT, computed tomography; L, left; OP, operative; OT, ovarian torsion; Otu, ovarian tumor; Pt, patient; R, right; WT, weight.
All SIPES cases were performed using an intracorporeal approach with the dissection and removal of the ovarian tissue being carried out inside the abdomen. Additional (unplanned) trocars were not needed in any of the cases. On average, total median operative time was 42±29 minutes (range, 23–123 minutes). Median estimated blood loss was 4 mL (range, 2–30 mL). The postoperative length of stay was 1 day (n=15), 2 days (n=3), and 3 days (n=1) (a neonatal patient hospitalized for other reasons). There were no intraoperative complications. Pathology reports (n=16; no specimen in 3 cases) revealed hemorrhagic/follicular/paratubal cyst (n=7), necrotic/calcified ovarian tissue after torsion (n=6), cystadenofibroma (n=1), granulosa cell tumor, adult type (n=1), and mature teratoma (Grade 0) (n=1) (Table 1). Median follow-up (n=19) in our outpatient clinic was 15 months (range, 10–21 months). None of the patients underwent reoperation or were readmitted.
Discussion
This study evaluates the feasibility of SIPES for ovarian/adnexal pathology in neonatal and adolescent patients. The threshold to perform laparoscopy for this indication was low. This is because of the fact that a normal Doppler ultrasound cannot exclude ovarian torsion. Sonography can only detect interruptions of arterial flow but may have limitations to diagnose venous flow interruptions, which often precede arterial compromise. 15 Even in children with severe abdominal pain, a mass >5 cm, and age >1 year, its sensitivity does not exceed 83%. 16 Therefore, we consider laparoscopy without delay as the gold standard to rule out ovarian torsion to save ovarian function.
The median age of the children in our study was 11.4 years and therefore lower than in other pediatric reports of single-incision endosurgery for ovarian/adnexal pathology.9,17 This is quite relevant as technically there is no difference in operating on adolescent girls of 16 years and older compared with adult women. However, the proprietary trocars on the market are not designed for smaller children and require great care during insertion in these small patients. By successfully operating two neonates (6 and 48 days) using SIPES, we underscore the feasibility of this technique for ovarian/adnexal indications at any age (Table 1).
Some authors have stated that for ovarian pathology, articulating instruments are mandatory in order not to hamper procedure accuracy, which could result in a longer operating time and unnecessary rupture of the cyst.18,19 However, as the ovaries are directly accessible from the umbilical approach and the moderate Trendelenburg position generally allows sufficient working space in the lower abdomen, special laparoscopic instruments for SIPES on ovarian/adnexal pathology are not needed.10–12 By using a long camera–endoscope combination, long straight instruments, or even instruments of different lengths, the operators' hands are separated and not restricted by clashing. Therefore, in our institutions roticulating graspers are only used for certain reconstructive indications, during which they may sometimes facilitate the operative dissection by creating a different angle. 11
The median operative time was 42 minutes, which is favorable compared with other reports (60–74 minutes). 8 One publication on SIPES for ovarian pathology from Turkey describes an extremely short mean operating time of 25 minutes including an ovary-preserving teratoma excision that was carried out in 19 minutes. 9 A multi-institutional evaluation on laparoendoscopic single-site surgery showed that operating time decreases and reaches a plateau after about 20 cases. 20 We attribute the missing classic learning curve in our study to the fact that our group has had previous experience with other SIPES cases.10,11 Although the loss of triangulation using the SIPES technique may pose a handicap for procedures such as cholecystectomy, splenectomy, and fundoplication,10,11 this effect may be less pronounced during mobilization of the ovaries and adnexae, as they are generally easy to access in children. As current evidence demonstrates the effectiveness and safety of electrosurgical devices in gynecologic surgery, 21 a monopolar cautery device was used for unroofing and marsupialization. In the case of salpingectomy and salpingo-oophorectomy an endosurgical stapler was introduced to minimize bleeding and decrease operating times.
There are several publications showing the feasibility and safety of single-incision endosurgical approaches for treatment of select malignancies such as early-stage endometrial or ovarian cancer, pelvic masses, and precancerous conditions in adults. 22 In a retrospective study of 26 single-incision endosurgery cases on a gynecologic adult oncology service, multiple procedures were successfully carried out with low perioperative complications. 20 One of the concerns using single-incision laparoscopic surgery has been potential cyst rupture, which was recorded in 13.6% of cases in a prospective adult trial on benign adnexal disease. 23 Of note is that the rate of cyst rupture during laparoscopy with multiple trocars has been reported in a comparable range of 6%–27%.24–26 Including our own study, in children there are only 7 cases of teratoma resections reported by single-incision endosurgery so far.8,9 Therefore at present no recommendation can be made for the use of this technique in the treatment of adnexal masses with malignant potential. Moreover, in these cases every effort should be made to spare the ovary, especially if the tumor markers are normal. 27 In Patient 4 the surgeon had a reasonable certainty that no viable gonadal tissue could be salvaged because of frank necrosis of the ovary. Therefore the individual decision was made against ovarian-sparing surgery.
Obesity has been suggested to be a technical obstacle and a risk factor for conversion to laparotomy, as well as prolong the operation time and hospital stay in patients undergoing laparoscopic ovarian surgery. 28 However, we could not confirm this for SIPES as the two girls both weighing 90 kg were operated in 39 minutes and 41 minutes, respectively (Table 1). Others also found that obesity is not necessarily a problem, and certainly not a contraindication, for performing single-incision laparoscopic surgery. 20
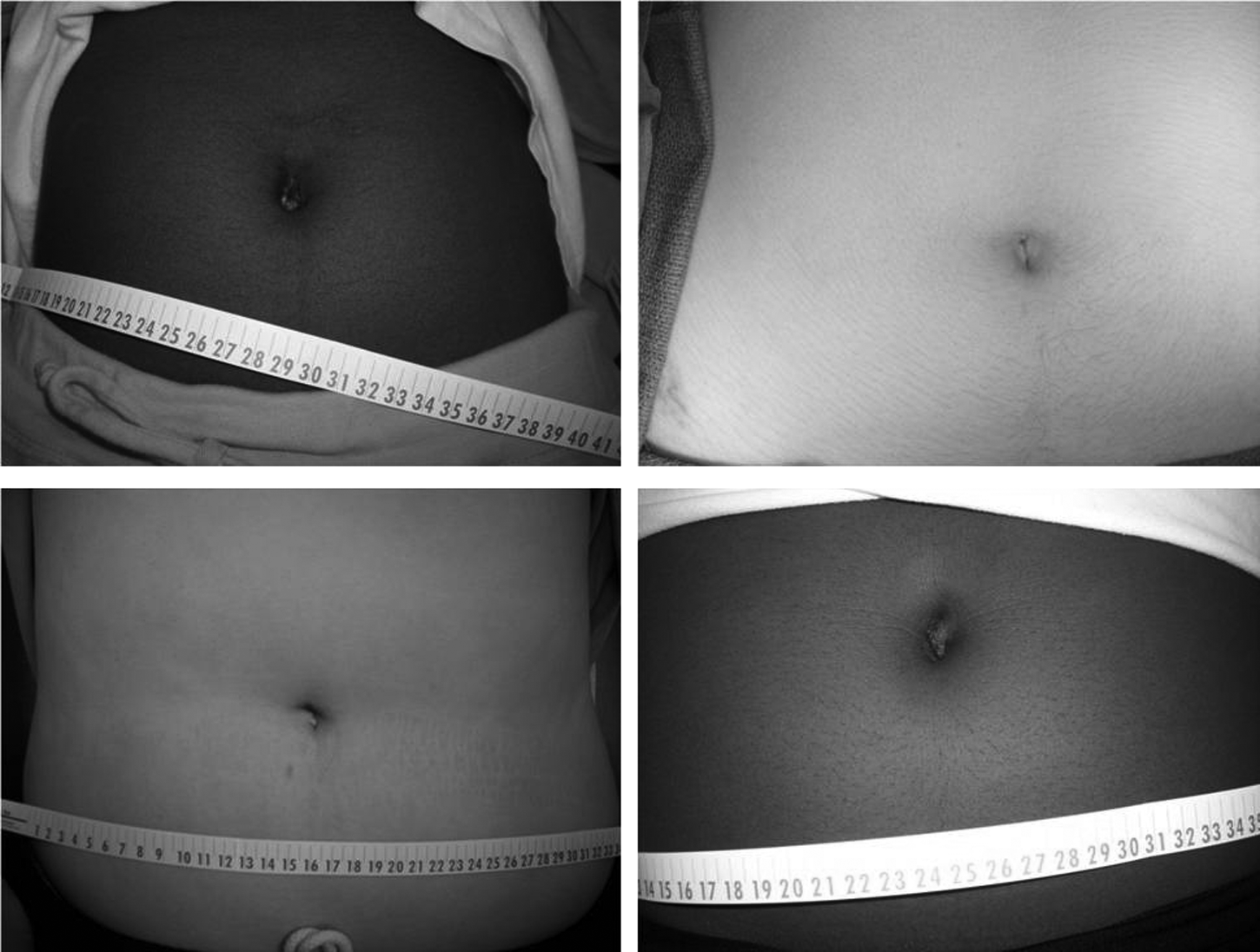
In the present study, the scar resulting from single-incision endosurgery was cosmetically appealing and highly appreciated by all patients and parents (Fig. 1). Although this benefit is obvious, the more important indicator for its future acceptance will be whether or not SIPES demonstrates minimized postoperative discomfort, perioperative morbidity, and decreased convalescence. If this is the case, the increased technical demands will be justified when compared with conventional laparoscopy. However, evidence for this is lacking, and whether single-incision laparoscopic surgery causes less or more pain is under current debate.29,30 Preliminary comparative studies in children indicate that postoperative pain after SIPES is at least no worse than after conventional laparoscopy. As the learning curve of these kind of procedures is overcome, large prospective studies are warranted to address these questions.31,32
The strength of the study presented here is the sample size of neonatal and adolescent patients undergoing SIPES. However, we recognize that this is still a small population with a short follow-up and lack of control group. Furthermore, as most cysts resolve spontaneously in adolescent girls within two to three menstrual cycles, 33 there still is controversy on the ideal treatment of these patients, regardless the number of ports used. Once the patients present with severe abdominal pain and the decision is made to operate, we consider laparoscopic unroofing with or without marsupialization as the procedure of choice in the adolescent patient, in accordance with other authors.34–36 Although the recurrence rate of this technique is described to be as high as 5%–8%, 33 we favor this method over resection to maximize ovarian preservation. 37 Because the surgeon can never be completely certain that the ovarian mass is not a cystadenoma or a cystic teratoma, a thorough preoperative workup including radiologic imaging (computed tomography/magnetic resonance imaging) and tumor markers is mandatory.
In summary, surgery for ovarian or adnexal indications can be accomplished successfully and safely in any pediatric age group, including neonates, using single-incision endosurgery. For this indication it is an excellent and virtually scarless alternative to conventional laparoscopy that facilitates the resection and extraction of ovarian masses without compromising cosmesis. Although the preliminary results are promising, the routine application of this novel technique requires further scientific evaluation in larger, prospective studies.
Footnotes
Disclosure Statement
No competing financial interests exist.