
Abstract
Abstract
Background:
In laparoscopic surgery with CO2 pneumoperitoneum, serious complications often occur for elderly patients and those who undergo long operations. These complications mainly include respiratory and circulatory system changes. In patients with tumors, release of free tumor cells into the abdominal cavity is believed to be possible. Gasless laparoscopic techniques can avoid these complications of CO2 pneumoperitoneum. Currently, the main shortcoming of gasless laparoscopic techniques is inadequate operative space. Because of this shortcoming, gasless techniques have not been widely applied in clinical practice.
Materials and Methods:
We herein describe a new technique of gasless laparoscopic cholecystectomy in pigs using a self-designed umbrella-like abdominal wall-lifting device. This device lifts up the anterior abdominal wall by opening the umbrella leaf in the abdominal cavity.
Results:
Five pigs underwent laparoscopic cholecystectomy using this technique. The operation times were 85, 40, 28, 21, and 24 minutes. The corresponding bleeding volumes were 11, 20, 5, 2, and 8 mL.
Conclusions:
These preliminary outcomes suggest that the umbrella-like abdominal wall-lifting technique is safe and feasible in gasless laparoscopic surgery and can provide sufficient exposure of the operative field. Further study in the form of randomized controlled trials is needed to investigate the advantages of this new technique.
Introduction
Materials and Methods
Five male Bama miniature pigs weighing 26–31 kg were used for this study. The animals were not allowed anything to eat for 12 hours preoperatively, but drinking was not restricted. Atropine (0.02 mg/kg) and ketamine (10 mg/kg) were intramuscularly administered before the operation. The animals were placed in the supine position, and pentobarbital (20 mg/kg) was intravenously administered to induce anesthesia. After endotracheal intubation, 1.5% isoflurane was administered to maintain anesthesia. Electrocardiographic electrodes were connected on the body surface to constantly monitor the electrocardiogram and heart rate. Instruments and equipment used in the experiment included one scalpel, two pairs of towel clamps, one 10-mm trocar, two 5-mm trocars, one pair of laparoscopic scissors, one pair of laparoscopic electric coagulation forceps, one laparoscopic suction device, one umbrella-like abdominal wall-lifting device, one laparoscopic system with a 1.0-cm laparoscope and camera, and one cold light system.
A 10-mm-long incision was made in the lower edge of the umbilicus. The incision was lifted up with two pairs of towel clamps, and a 10-mm trocar was inserted. The needle core of the trocar was pulled out, and a laparoscope was inserted. A 10-mm-long incision was made in the wall 1–2 cm above the umbilicus, and the umbrella-like abdominal wall-lifting device was inserted under laparoscopic guidance. After the peritoneal cavity was entered, the umbrella leaves were opened. The anterior abdominal wall was lifted, and the lifting device was fixed on the mechanical arm. The other three trocars were inserted into the abdominal wall, and the operation equipment was placed into the peritoneal cavity to perform the cholecystectomy.
The operation time and intraoperative bleeding volume were recorded. The operation time was calculated as the time from cutting of the umbilical ring incision to completion of skin suturing, and the bleeding volume was computed by the gauze-weighing method and suction bottle determination method. The weight difference between the preoperative and postoperative gauze was the partial intraoperative bleeding volume (1 g=1 mL). The hemoglobin concentration was multiplied by the total amount (in mL) in the suction bottle, and this value was divided by the preoperative hemoglobin concentration in venous blood. The result was the other partial intraoperative bleeding volume. The sum of the two volumes was the total bleeding volume.
Results
Five pigs underwent laparoscopic cholecystectomy using this technique. The operation times were 85, 40, 28, 21, and 24 minutes, with a mean operative time of 29.6 minutes. The corresponding bleeding volumes were 11, 20, 5, 2, and 8 mL, with a mean operative bleeding volume of 9.2 mL.
Discussion
In 1991, in Japan, Nagai et al. 7 completed a laparoscopic cholecystectomy with a gasless technique for the first time. The principle of the Japanese laparoscopic gasless devices of the Daoke Medical Company (Shanghai, China) currently follows the example of Nagai et al. 7 We call this the Daoke lifting system. A pair of Kirschner wires is used to penetrate the subcutaneous tissue of the anterior abdominal wall, which is pulled up by a mechanical device to create an operation space. 8 In 1996, in Taiwan, Chang et al. 9 reported an airlift balloon retraction system comprising one balloon retractor and one Laparolift™ (Covidien, Norwalk, CT) arm. In 1997, in the United States, Hirsch et al. 10 reported use of the Laparofan™ (Covidien)/Laparolift system. The closed Laparofan retractor was inserted into the abdominal cavity and then opened for planar retraction of the abdominal wall. These early gasless lifting systems have had great impacts on the design concept of newer gasless techniques.
Some new systems for gasless laparoscopic surgery were recently reported. In 2003, in Japan, Izumi et al. 11 reported a loop-shaped metallic retractor designed for planar lifting of the anterior abdominal wall. The radius of the loop was 8.5 cm. The retractor was inserted into the peritoneal cavity through the port incision and pulled up using the Kent retractor system. Its shortcomings are mainly as follows: first, the retractor had some degree of upward slippage because the rod and hook connected at an angle of 97° instead of 90°. Second, it was difficult to get through the abdominal wall of obese patients. In 2010, Wu et al. 12 reported a self-designed gasless laparoscopic device that comprised one self-retaining retractor and holder. A 5-cm abdominal incision was needed, which was pulled up through four small retractors to lift the anterior abdominal wall. The requirement of a large incision was the main disadvantage.
In its early stages of development, gasless laparoscopic surgery was mainly applied in simple operations such as cholecystectomy and appendectomy. After years of development, it is now applied in various complex surgeries such as radical resection of colorectal carcinoma, 13 gastrectomy, 14 hepatectomy, 15 live-donor nephrectomy, 16 ovarian tumor resection, 17 and thyroidectomy. 18 However, gasless laparoscopic surgery has not been widely applied in clinical practice. The main reason is that the disadvantage of insufficient exposure of the operative field has not been overcome.
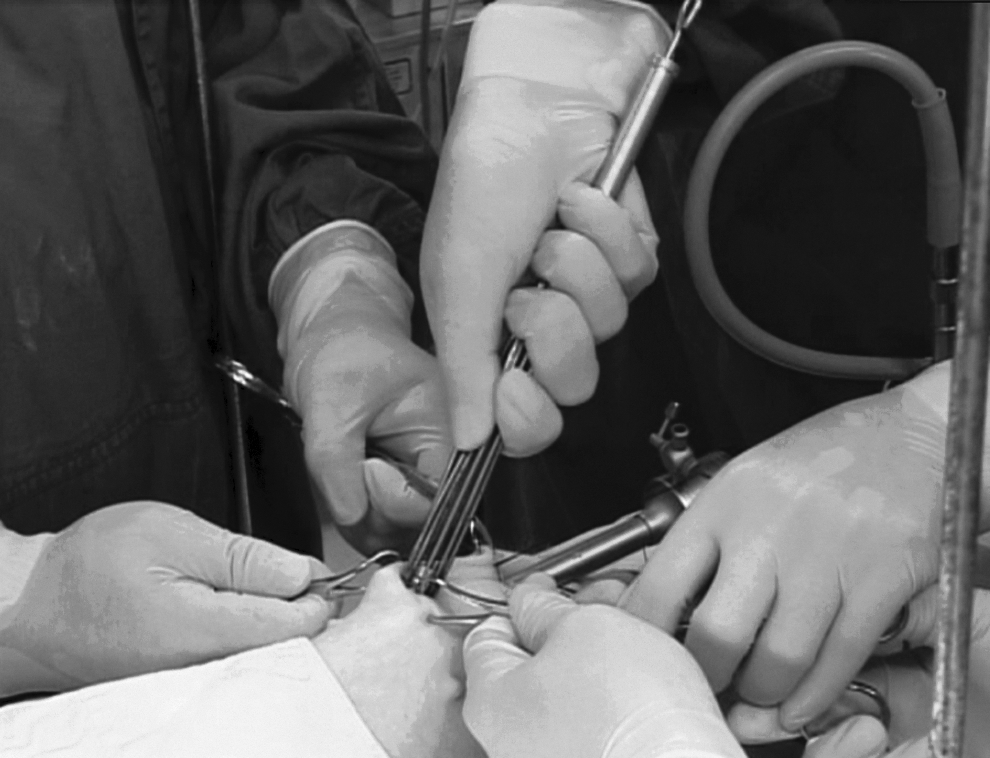
Our self-designed umbrella-like lifting system comprises one umbrella lifting device and one mechanical arm, which can be fixed on the side rail of the operating table (Fig. 1). Ten spokes form an umbrella through a folding movement (Fig. 2). The umbrella is 150 mm in diameter. The principle of our novel abdominal wall-lifting system is fundamentally different from those of previous abdominal wall-lifting systems. For example, the holding point of the lifting power in the Daoke lifting system is linear in the subcutaneous tissue of the abdominal wall with one pair of Kirschner wires. Because the subcutaneous tissue is loose, the lifting effect of the abdominal wall is insufficient. However, our umbrella-like lifting device is opened under the anterior abdominal wall and then pulls it up. The holding point of the lifting power is planar under the anterior abdominal wall with 10 spokes of the umbrella (Fig. 3). Thus, compared with previous lifting systems, our novel abdominal wall-lifting system can provide a larger operative space. When closing, the shape of the umbrella lifting device is similar to that of a trocar, and the procedure of entering the abdominal cavity is almost identical between the two (Fig. 4). Thus, the operating procedure is familiar and easy for surgeons to master. When opening, the umbrella is round in shape. The round shape is matched with the side of the ribs in the upper abdomen and pelvis in the lower abdomen and can give full play to suspending effects (Fig. 5).

Umbrella lifting system used in an operation.
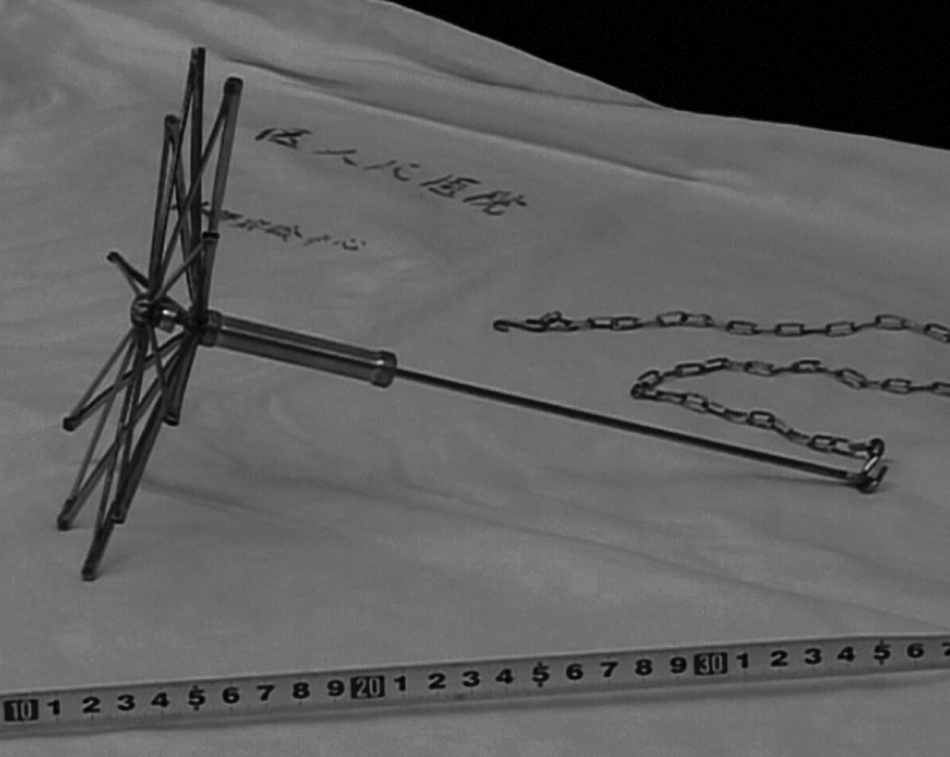
Umbrella lifting device, fully opened.
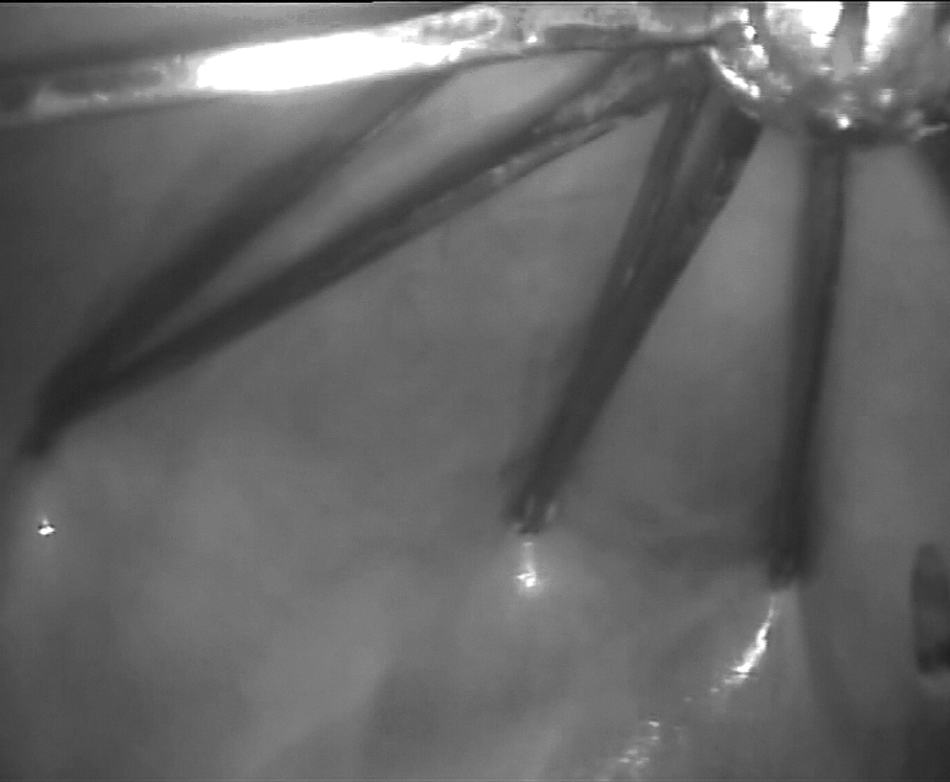
Umbrella lifting device, opened under the abdominal wall.
Umbrella lifting device, fully closed.

Umbrella lifting device and the side of the ribs (where the tips of the thumbs are placed).
In the first 2 cases in the present study, the greater omentum got stuck on the spokes during the process of opening the umbrella, and we had to spend some extra time dealing with it. That was why the first 2 cases, especially the first case, required more operative time than the other 3. To avoid this problem, two points should be considered. First, the operation should be monitored laparoscopically when the umbrella enters and opens in the abdominal cavity. Second, when fully present within the abdominal cavity, the umbrella should be pulled upward while simultaneously opening until its spokes are completely opened.
In our 5 cases, the bleeding volume and operation time were acceptable with the exception of the first case, in which the operation time was a bit too long. We plan to perform additional animal experiments to demonstrate the advantages of this umbrella-like lifting system.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Fund Projects (number 581160187).
Disclosure Statement
No competing financial interests exist.