
Abstract
Abstract
Background:
The surgical management of morbid obesity is faced by several challenges. Alternative therapeutic strategies could have an important role in the perioperative risk reduction. The BioEnterics® intragastric balloon (BIB) (Inamed Health, Santa Barbara, CA) has been described as being effective in weight reduction and is used as a bridge before bariatric surgery. This study examined the efficacy of BIB in obese Egyptian patients and the value of the extended low caloric liquid diet program in weight loss.
Subjects and Methods:
A retrospective review of a prospectively maintained bariatric database was conducted. Weight changes and complications data were analyzed. Indications for BIB placement were discussed.
Results:
Records of 55 patients (11 males and 44 females) were retrieved. The mean initial body mass index (BMI) was 45.3±11 kg/m2. The mean of excess body weight percentage was 111.96±53.2%. Nausea was reported in 30 patients (54.5%). Epigastric discomfort was reported in 23 patients (41.8 %), and vomiting was reported in 27 patients (49.1%). Six patients (10.9%) had an early removal of the balloon, whereas 4 (7.2%) had delayed removal (more than 6 months). The mean excess weight loss percentage (EWL%) was 17.2%. There was significant reduction in patients' BMI from 45.3 to 38.3 kg/m2 (P<.001). There was no significant correlation between the EWL% and the gender, age, or initial BMI. Two patients had second balloon insertions without complications. There was no significant difference in the EWL% between the 1-week liquid diet group and the extended (4-week) low caloric diet group.
Conclusions:
The BIB is effective and safe in weight reduction in obese Egyptian patients. The impact of extended liquid dieting period is not significant.
Background
The use of the intragastric balloon as an adjuvant treatment for morbid obesity was first presented at the International Conference at Tarpon Springs, FL, in 1987. 11 The first balloon, called the Garren–Edwards bubble, 12 which was made of polyurethane filled with up to 220 mL of air, was associated with several frequent complications, such as balloon malfunction, stomach ulcers and perforations, and obstructions. These negative events resulted in a poor acceptance of the technique. 13 Moreover, the clinical efficacy of the Garren–Edwards bubble was questioned in several studies.13–18 The frequency of complications has been significantly reduced upon the introduction of the BIB, which is an elastic, soft spherical silicone balloon filled with saline. 19
The objective of this study is to examine the efficacy of the BIB as a weight reduction tool in an obese Egyptian population, as well as the value of an extended liquid dieting period in the weight loss.
Patients and Methods
The study was conducted at the Hepatobilliary and Pancreatic and Minimal Invasive Surgery Unit, Department of Surgery, Alexandria Main University Hospital, Alexandria, Egypt.
A retrospective review of a prospectively maintained bariatric database was conducted. Records for patients who had undergone BIB were retrieved. The collected data included the indications of balloon placement, initial weight, duration until removal, weight loss, and complications. Insertions were performed by two consultants who described two different early dieting regimens for their patients: Group 1 was instructed to intake an extended liquid diet for 4 weeks, and Group 2 was instructed to take liquid diet for 1 week only.
Informed consent was obtained from each patient. Patients were admitted for BIB placement while they were under general anesthesia. Diagnostic endoscopy was performed in all cases prior to the placement of the BIB to exclude any contraindications for insertion. The first five balloons were inflated with 650–700 mL, whereas all other balloons were inflated with 600 mL. All balloons were inflated with saline mixed with methylene blue dye to detect rupture if the urine color changed to blue. All patients received postoperative antiemetics and proton pump inhibitors. All patients were discharged after a few hours. Patients in Group 1 had only liquid low caloric diet for 4 weeks after the balloon placement, whereas patients in Group 2 had this regimen for only 1 week. Gradual commencement of solid low caloric intake was then initiated. Patients who developed vomiting were treated conservatively. Those with persistent vomiting were re-admitted to the hospital for intravenous fluid replacement, withholding the oral intake until cessation of vomiting.
SPSS version 16 (SPSS, Inc., Chicago, IL) was used for analysis of data as appropriate.
Results
Fifty-five patients have undergone balloon insertion from February 2010 to August 2011. The mean age was 33.22 years (range, 9–68 years). Eighty percent of the patients were females (n=44), and 20% (n=11) were males. The first surgeon treated 32 patients (Group 1), and the second surgeon treated 23 patients (Group 2). The initial weight and body mass index (BMI) values were 124.4±35.8 kg and 45.3±11 kg/m2, respectively (Table 1). Sixteen patients (29%) with BMI >50 kg/m2 had balloon placement to reduce the operative risk, whereas 20 patients (36.4%) with BMI <40 kg/m2 and 19 patients (34%) with BMI between 40 and 50 kg/m2 were seeking a nonoperative measure for weight reduction.
Data are mean±standard deviation values (range).
Data are mean±standard deviation values (range) or mean, mode values (range).
One patient who had her balloon removed at 3 days was excluded from weight loss analysis.
By paired t-test.
Number of patients is 55.
BMI, body mass index; EWL%, excess weight loss percentage; n, number of patients.
All patients were discharged a few hours after the procedure. All patients received proton pump inhibitors along with antiemetic therapy for 1 week as a routine. Patients in Group 1 had low caloric liquid diet for 4 weeks, whereas patients in Group 2 had liquid diet for only 1 week. Solid low caloric diet (800 kcal) was gradually resumed thereafter.
The mean duration for the intragastric BIB was 5.7 months (range, 3 days–9 months). Six patients (10.9%) had their balloons removed before 6 months (range, 3 days–5 months). Four patients (7.2%) had their balloons removed after the 6-month period (range, 7–9 months). Excluding cases with very early removal (less than 1 month), the mean excess weight loss percentage (EWL%) at the time of BIB removal was 17.17±8%.
There was a significant difference between the mean of the initial weight (124.4 kg) and the weight at the removal of the BIB (107.2 kg) (P=.0001). Similarly, the mean BMI decreased significantly from 45.3 kg/m2 to 38.2 kg/m2 (P=.001) (Table 1) No significant relation was found between the gender, age, or the initial BMI and the EWL% (P=.134). No significant difference was found in the EWL% between Group 1 and Group 2 (P=.645).
The most frequently reported post-insertion complication was nausea in 30 patients (54.5%), whereas epigastric discomfort was reported in 23 patients (41.8%). Vomiting was reported in 27 patients (49.1%). In 6 patients (10.9%) it was severe enough to require rehospitalization for intravenous fluids administration and antiemetic therapy; 3 patients (5.5%) had vomiting for 2 days, whereas the other 3 patients had vomiting for 3–5 days. Figure 1 summarizes the frequency of complications encountered in this series.
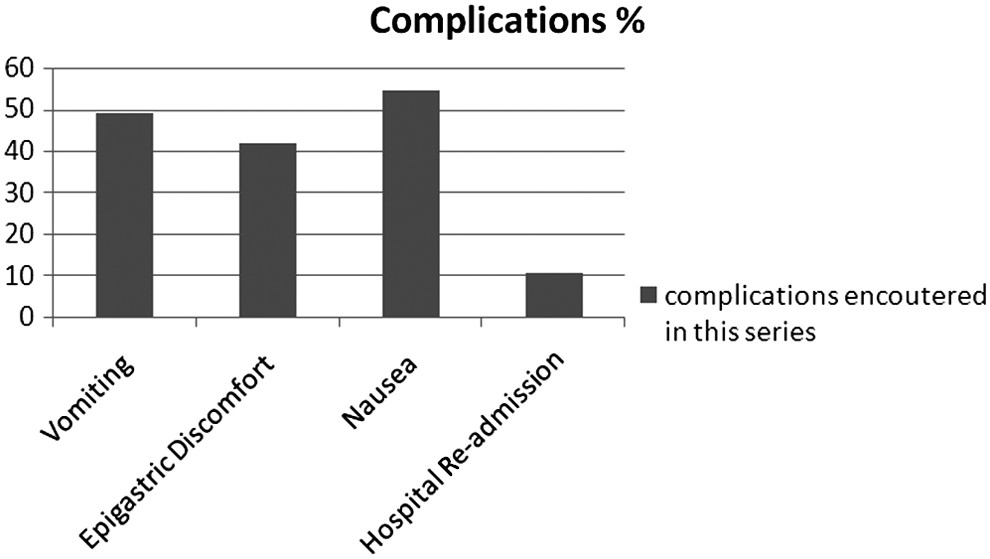
Summary of complications encountered in this series represented on a percentile scale.
Discussion
Bariatric surgery in superobese patients is technically difficult. Our preoperative strategy for those patients is to encourage them to commit to a preoperative strict weight loss dietary regimen. BIB as a weight reduction measure 20 was not used in our practice until early 2010. The initial indication for the BIB placement was to reduce preoperative weight in order to decrease the surgical morbidity and mortality in superobese patients. 21 Two other categories of patients underwent BIB placement: patients with BMI <40 kg/m2 and patients with BMI between 40 and 50 kg/m2 who were seeking nonsurgical treatment. BIB is mainly used as a bridge for morbidly obese patients, before undergoing bariatric surgery, in order to decrease the operative risk.22,23 Indications for BIB usage in lesser grades of obesity has been increasingly accepted24,25 and the improvement of the metabolic profile after BIB placement has been reported in several studies.26–29
The insertion of BIB is usually safe and easy. Our first 5 cases had significant epigastric discomfort and persistent vomiting, which were not encountered in the rest of the cases. These patients required rehospitalization for symptoms control with intravenous fluids and antiemetic therapy. This was ascribed to the inflation volume, which was 650–700 mL. These symptoms occurred less intensely after reduction of the inflation volume to 600 mL in subsequent patients. Contrary to data published in other series, 30 our patients could not tolerate the maximum inflation volume of the balloon. The greater weight loss reported by Lopez-Nava et al. 30 could be attributed to the greater inflation volume.
It was clear that BIB with a suitable dietary regimen could result in a significant weight loss, as has been demonstrated in other studies.30,31 The weight loss accomplished at the time of balloon extraction was statistically significant. Our weight loss results were in range of those published in other trials.22,23,25,32–34 In our study the consistency of diet did not influence the weight loss accomplished at the time of balloon removal, nor did it impact the reduction of vomiting.
Up to 30 kg/m2 in BMI was reported to be the average weight loss by Sedov and Fishman. 35 The effectiveness of the BIB system was reported by several other studies.24,36,37 The best weight loss results was reported to be in patients with BMI from 35 to 40 kg/m2. 38 The balloon, by itself, was proved to have an active role in weight reduction over that induced by diet alone. 31 Second balloon insertion was reported to be beneficial to augment the weight reduction induced by the first balloon.39–41
Long-term effect of BIB combined with pharmacotherapy was superior to the combination with only lifestyle modification.42,43 Some patients were reported to continue lose weight for up to 22 months of follow-up after balloon extraction. 44 Long-term maintenance of weight loss is controversial. Some studies confirmed it,10,45 whereas others reported that weight regain after BIB was universal and that almost all patients needed surgery after balloon removal. 46
Forty-five patients (81.8%) in our series had their balloons removed at the scheduled date. Intractable vomiting required balloon removal after 3 days in 1 case. Recurrent vomiting and unrelieved epigastric discomfort were the cause of early removal in 3 patients at 1–3 months. Totte et al. 34 reported early removal for vomiting in 3 patients. Halitosis in 1 patient was the reason for removal at 5 months in our series; retained putrefied food inside the stomach was seen at the time of removal. One patient requested the removal of the balloon at 4 months without somatic cause. Four patients, who did not commit to the removal date, had their balloon removed at 7 months (2 patients), 8 months (1 patient), and 9 months (1 patient). There were no adverse effects noticed in these patients; nevertheless, the balloon showed some disintegration of the shell on removal at 9 months.
Gastric perforation,47,48 small intestinal obstruction,49–52 and fungal colonization 53 were reported as complications secondary to the insertion of BIB, yet the overall incidence is considered acceptable, with the majority of complications being mild and corrected by the balloon removal. 20 None of these complications was encountered in our series.
We conclude that BIB is effective in weight reduction in the Egyptian obese population. BIB is a safe procedure for weight loss. An inflation volume of 650–700 mL was not tolerated in our patients. There was no significant impact of the extended liquid diet period on the weight loss at the time of removal.
In future studies risk analysis of patients undergoing surgery following BIB insertion will be conducted in comparison with those who are going directly for surgery in a prospective study.
Footnotes
Acknowledgments
The authors express their gratitude to Dr. Heba El Komy and Dr. Mohannad Ibrahim Abbas Gaber for their effort in maintaining the database.
Disclosure Statement
No competing financial interests exist.