
Abstract
Abstract
Objective:
Laparoscopic hepatectomy is widely used in the surgical treatment of left-sided hepatolithiasis (LSH). Lithotomy using a cholangioscope usually is required for the treatment of concurrent right-sided hepatolithiasis or choledocholithiasis. The primary objective of this study was to evaluate the effectiveness and safety of gallstone elimination using cholangioscopy through the left hepatic duct (LHD) orifice versus the common bile duct (CBD).
Patients and Methods:
Eligible LSH patients (n=41) were scheduled for laparoscopic left lateral segmentectomy or left hemihepatectomy with intraoperative biliary exploration using cholangioscopy through the LHD orifice (LHD group, n=23) or the CBD (CBD group, n=18) at the discretion of patients. Laparoscopic T-tube insertion was performed in selected patients. Patients were regularly followed up at monthly intervals or more frequently in the presence of any symptom. The primary outcome measures included overall operative time, duration of the cholangioscopy procedure, volume of blood loss, length of hospital stay, and frequency of procedure-related complications.
Results:
The two groups were comparable in sex, age, symptoms, site of lesion, and gallstone comorbidities (P>.05). Of the 18 patients in the CBD group, 12 (66.7%) patients had a T-tube inserted in contrast to 1 (4.5%) patient in the LHD group. The two groups were comparable in cholangioscopy duration and volume of blood loss (P>.05), whereas the LHD group had a significantly shorter operative time than the CBD group (221.4±58.6 minutes versus 171.2±63.5 minutes; P<.05). The postoperative duration of hospitalization was significantly shorter in the LHD group than in the CBD group (7.5±2.2 days versus 4.2±1.9 days; P<.05). No patient showed any recurrence of gallstones or cholangitis during the follow-up period.
Conclusions:
As an effective and safe technique that is comparable to choledochotomy, LHD cholangioscopy is a preferred alternative to choledochotomy in the laparoscopic treatment of LSH because it offers patients shorter operative duration and length of hospitalization.
Introduction
However, the use of laparoscopy alone is insufficient to treat LSH complicated with secondary right-sided hepatolithiasis or extrahepatic choledocholithiasis. 10 Therefore, additional bile duct exploration and possible lithotomy using endoscopic or surgical techniques are required in these cases. Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy has been reported to be an effective modality for the adjuvant treatment of primary and residual choledocholithiasis. 11 This minimally invasive approach, however, can lead to the destruction of Oddi's sphincter, enterobiliary reflux, and cholangitis, although it accelerates postoperative recovery. 12 Procedure-related acute pancreatitis and duodenal perforation are less likely to occur with ERCP, but the procedure is life-threatening in some cases. 13 Therefore, surgical exploration of the common bile duct (CBD), namely, choledochotomy with cholangioscopy, is generally recommended for the treatment of complicated hepatolithiasis and the preservation of biliary drainage. 14
The potential risks of choledochotomy include bile leakage and biliary stricture caused by the dissection of the CBD. 15 The placement of a T-tube is mandatory in some cases. 16 Laparoscopic insertion of the drain can be technically challenging and may require the additional assistance of access ports, which would prolong the operative duration. Additionally, the presence of a T-tube may affect patients both physically and psychologically, increasing the likelihood of biliary tract infection. 17 Hwang et al. 18 examined the CBD through the transected left hepatic duct (LHD) orifice in the open procedure of LSH. In their study, over 90% of patients avoided the choledochotomy and subsequent T-tube placement, with a minimal risk of residual gallstones and gallstone recurrence. This approach has been used in laparoscopy-assisted left lateral lobectomy. It significantly reduced the occurrence of operative complications and accelerated the postoperative recovery compared with the conventional open procedure. 19 It remains unknown whether cholangioscopy via the LHD orifice is superior to that via the CBD in terms of both procedural effectiveness and safety in the context of laparoscopic resection of the LSH. In this head-to-head comparative retrospective study, we evaluated the effectiveness and safety of gallstone elimination using cholangioscope insertion through the LHD stump versus the CBD.
Patients and Methods
Patient enrollment
This study was approved by the Institutional Review Board at each participating center. Patients (n=120) diagnosed with primary hepatolithiasis were retrospectively and consecutively enrolled between June 2002 and December 2009 (Fig. 1). Eligible patients (n=41) were scheduled for laparoscopic left lateral segmentectomy or left hemihepatectomy with intraoperative biliary exploration through the LHD orifice (LHD group) or choledochotomy (CBD group) if gallstones were found to be mainly located in the left intrahepatic bile duct and were causing a marked parenchymal atrophy of the left lobe, as visualized using magnetic resonance cholangiopancreatography (MRCP), ERCP, and/or computed tomography. The patients were well informed of the advantages and disadvantages of the two approaches and gave informed consent prior to surgery. The assignment to either approach was at the discretion of the patient himself or herself. A patient was excluded if he or she had right-sided intrahepatic biliary stricture and hepatic atrophy requiring bilateral hepatectomy, extensive intrahepatic gallstones requiring biliary enteric anastomosis, or hilar cholangiocarcinoma requiring the resection of extrahepatic bile duct and lymph nodes. All procedures were performed by the surgical team led by R.L.
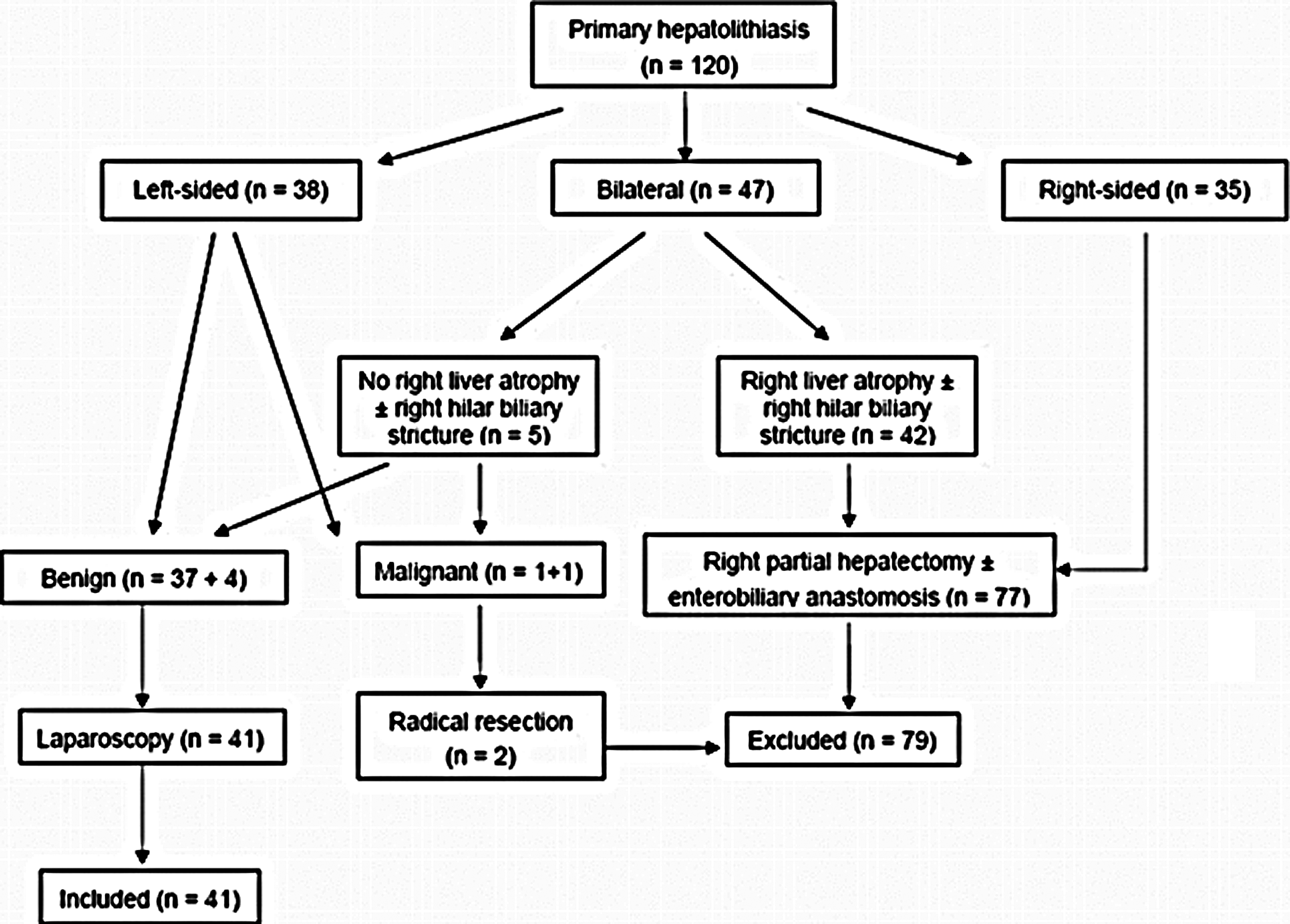
Flow chart of patient enrollment and treatment algorithm.
Laparoscopic liver resection
In laparoscopic left hemihepatectomy, the falciform ligament, left coronary ligament, left triangular ligament, and hepatogastric ligament were sequentially transected to mobilize the left lobe. The left hepatic artery was dissected and securely ligated (Fig. 2A), followed by the ligation and transection of the left main portal vein branch (Fig. 2B). The main trunk of the left hepatic vein was identified and temporarily clipped (Fig. 2C), and the left hepatic bile duct was interrupted and labeled. The hepatic parenchyma was transected along the proposed division line using an ultrasonic dissector (Ethicon Endo-surgery, Cincinnati, OH). Major vessels and bile ducts were securely clipped preceding the transection. The left hepatic vein and the surrounding parenchymal tissues were transected in proximity to the second hepatic hilum using an Echelon™ 60 stapler (Ethicon Endo-surgery, Guaynabo, Puerto Rico) (Fig. 2D). Additionally, in laparoscopic left lateral segmentectomy, the left lobe was dissected using the same protocol. The second hepatic hilum was exposed, and the left hepatic vein was temporarily disrupted. The liver parenchymal tissues were dissected approximately 2 cm along the falciform ligament to identify the hepatic pedicle of the left lateral segment. The pedicle was subsequently transected using the stapler, followed by the parenchymal dissection toward the second hepatic hilum. The left hepatic vein and the surrounding parenchymal tissues were transected using the stapler. Following the completion of liver dissection, the orifice of the transected LHD was identified and labeled on the stump.
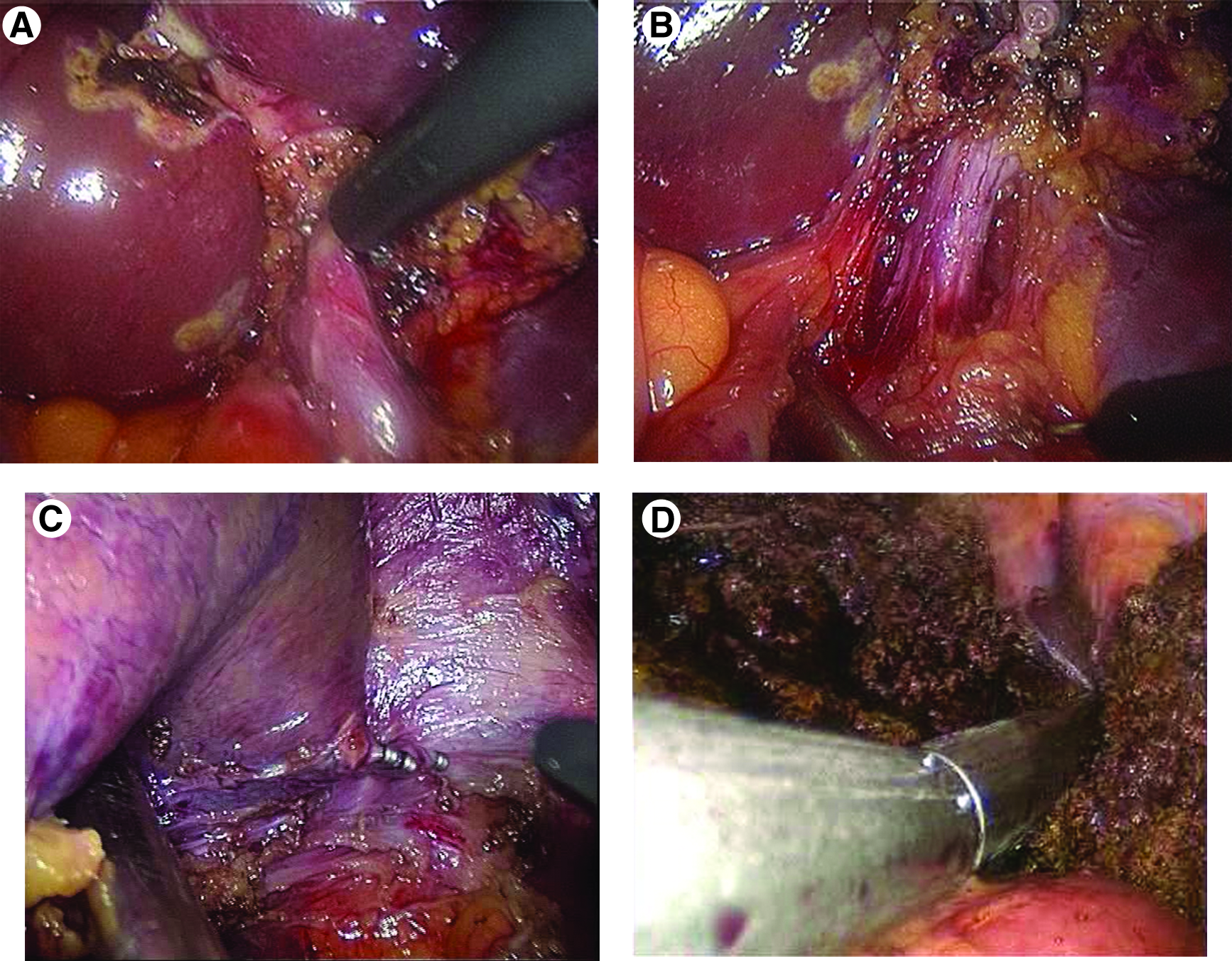
Laparoscopic left hemihepatectomy and subsequent cholangioscopy via the left hepatic duct orifice:
Intraoperative biliary exploration
For the LHD group, the LHD stump was dilated and retracted using sutures. A fiber cholangioscope (model CHF-P20; Olympus Medical Systems Corp., Tokyo, Japan) was inserted through the subxiphoid access port into the LHD with laparoscopic assistance. Following the removal of residual gallstones through the LHD stump, the cholangioscope was further advanced to explore sequentially the common hepatic duct, right hepatic duct, caudate lobe duct, and CBD, including Oddi's sphincter (Fig. 3A). Residual gallstones were removed using a retrieval basket if applicable, followed by repeated bile duct flushing. After withdrawal of the cholangioscope, the LHD orifice was securely clipped or ligated. Laparoscopic choledochotomy and subsequent insertion of a T-tube were described previously (Fig. 3B). 20 The indications for T-tube placement were as follows: the patient was at a high risk of having residual gallstone(s), the Oddi's sphincter was strictured or regurgitated or exhibited poor function, or the diameter of bile duct to be anastomosed was less than 1 cm in the cases of one-stage primary resection and anastomosis.

Intraoperative biliary exploration (schematic) using cholangioscopy via
Postoperative care and follow-up
All patients received routine care and monitoring and resumed oral intake if tolerated on postoperative Day 1. The nasogastric tube also was removed on postoperative Day 1. In the absence of bile leakage or peritonitis, patients were discharged following the removal of the peritoneal drain. Patients treated with cholangiography via T-tube who did not have residual gallstones had their T-tube removed 2 weeks following the operation during an outpatient visit. Those patients showing residual gallstones underwent cholangioscopy for gallstone removal 6 weeks after the first surgery. Patients were followed up regularly at monthly intervals or more frequently in the presence of any symptom. All patients received a routine hematology test, liver function test, and serum biochemistry assay, as well as abdominal ultrasonography, computed tomography scan, and MRCP at postoperative Months 1, 3, and 6 during follow-up visits. The overall treatment outcome was evaluated using the following criteria: excellent, the patient complains of no biliary symptoms and exhibits normal liver function and serum biochemistry; good, the patient complains of occasional mild biliary symptoms and exhibits a slight increase in liver-specific enzyme, which responds well to medical treatment and does not interrupt the patient's daily activities; or poor, the patient complains of clinically significant biliary symptoms, such as fever, jaundice, and biliary colic, that do not respond to medical treatment and require a secondary surgery.
Outcome measures
The primary outcome measures were the frequency of residual or recurrent gallstone disease or cholangitis as well as surgical complications. The secondary outcome measures consisted of the duration of cholangioscopy (from the insertion until the withdrawal of cholangioscope; it excludes the time required to close the bile duct or to place the T-tube), volume of blood loss, frequency of T-tube placement, and length of hospital stay.
Statistical analysis
All quantitative data were expressed as mean±standard deviation values. The difference in the means between the two groups was compared using the two independent samples Student's t test. All qualitative data were expressed as n (%). The difference between the two groups was compared using Fisher's exact probability test. P<.05 was considered to be statistically significant.
Results
Baseline characteristics of patients
In this study, the 41 patients eligible for laparoscopic hepatectomy integrating intraoperative cholangioscopy consisted of 15 men and 26 women, 31–69 years old. Table 1 showed the baseline characteristics of the LHD group (n=23) and the CBD group (n=18). The two groups were comparable in sex, age, previous history, hepatobiliary symptoms, site of lesion, and gallstone comorbidities (P>.05). No patient had received any previous upper abdominal surgery. The most frequently reported symptom was right upper quadrant pain and fever (cholangitis). Additionally, the majority of patients in the two groups had concomitant choledocholithiasis.
CBD, common bile duct; F, female; LHD, left hepatic duct; M, male; SD, standard deviation.
Surgical outcomes
Total laparoscopic hepatectomies were successfully completed in 40 patients (40/41, 97.6%), including left hemihepatectomy in 15 patients (15/40, 37.5%) and lateral segmentectomy in 25 patients (25/40, 62.5%). In the LHD group, the laparoscopic procedure was converted to open hilar cholangioplasty in 1 patient, who was excluded from further analysis, because of the unexpected stricture of the right hepatic duct orifice. Concomitant laparoscopic cholecystectomy was performed in 7 patients undergoing the CBD approach (7/18, 38.9%) and 5 patients undergoing the LHD approach (5/22, 22.7%). Intraoperative bile duct exploration using cholangioscopy was completed in all patients (40/40, 100%) via the assigned approach. Following liver resection, residual gallstones were identified and removed using CBD-approach cholangioscopy in 1 patient, whereas no residual stones were found on LHD-approach cholangioscopy. The two groups were comparable in duration of cholangioscopy and volume of blood loss (P>.05). No patient in either group required blood transfusion, as no uncontrollable bleeding occurred in the process of laparoscopic hepatectomy or cholangioscopy. Of the 18 patients in the CBD group, 12 (66.7%) patients had a T-tube inserted, whereas 1 patient (4.5%) in the LHD group underwent T-tube insertion through the transected LHD orifice because of a complicated bile duct condition. The LHD group had a significantly shorter operative time than the CBD group (221.4±58.6 minutes versus 171.2±63.5 minutes; P<.05) (Table 2).
Data are number (%) or mean±standard deviation values as indicated.
One conversion to open surgery because of the unexpected stricture of the right hepatic duct orifice.
CBD, common bile duct; IOC, intraoperative cholangioscopy; LHD, left hepatic duct; OD, operative duration; SD, standard deviation.
Postoperative complications
No clinically significant adverse events occurred in either group, except for 1 patient in the CBD group who experienced bile leakage in the absence of T-tube placement. In this patient, MRCP identified small residual gallstones in the CBD, which resolved with ERCP-integrated endoscopic nasobiliary drainage on postoperative Day 10. The postoperative duration of hospitalization was significantly shorter in the LHD group than in the CBD group (7.5±2.2 days versus 4.2±1.9 days; P<.05) (Table 2).
Follow-up outcomes
All patients were followed up for a mean period of 42 months (range, 18–113 months); no patient was lost to follow-up. No patient showed any recurrence of gallstones or cholangitis. For the majority of patients (36/41, 87.8%), biliary symptoms were resolved completely, and they returned to normal work and daily activities. Five (12.2%) patients were initially symptomatic but recovered with medical treatment. The two groups were comparable in overall treatment outcome, which was determined to be excellent or good in all patients.
Discussion
For most cases of left hepatolithiasis without a left hilar stricture, left lateral hepatectomy is the safest and most effective treatment. 21 Laparoscopic hepatectomy is preferred for the surgical treatment of LSH. 8 However, in the case of LSH complicated with extrahepatic gallstones, the assistance of other endoscopic interventions is usually required. ERCP with sphincterotomy is a minimally invasive technique compared with cholangioscopy via choledochotomy, and it has been widely used in the treatment of choledocholithiasis. ERCP is suitable for the removal of gallstones less than 1 cm in diameter and located in the CBD. These stones are usually composed of cholesterol and are rigid and solitary. However, the patient cohort in this study suffered primarily from hepatolithiasis with complicating choledocholithiasis. These patients often had a large number of gallstones that were relatively large in size, composed of pigments, and fragile in texture. The application of ERCP in these patients requires sphincterotomy and the use of delicate lithotripsy instruments. The operative time is expected to be longer, and the patients are subject to a higher risk of recurrent cholangitis, iatrogenic pancreatitis, and residual gallstone disease compared with cholangioscopy.22,23 In contrast, choledochotomy with cholangioscopy preserving Oddi's sphincter is preferred by most surgeons for removal of potential residual gallstones or the identification of biliary stricture. 14 However, choledochotomy is technically challenging in the context of laparoscopy, and it prolongs the operative duration and requires the insertion of a T-tube. Cholangioscopy along the pathway of LHD is basically an antegrade choledochoscopy, in contrast to ERCP. 17 Because of the minimal interference with the CBD itself, the insertion of a T-tube is rarely required in most patients undergoing intraoperative cholangioscopy via the LHD orifice, as shown in our study. Such a benefit contributed to the shortened operative duration and length of hospitalization observed in our study.
Anatomically, the path of the cholangioscope via the LHD orifice into the CBD and right hepatic duct does not make a sharp angle. Such a technique is easily manipulated, as few blind spots are present. 17 The entire major biliary tree can be visualized in a direct manner. Our results showed that cholangioscopy via the LHD orifice is comparable to conventional choledochotomy in terms of identifying any concomitant lesions, such as secondary intra- or extrahepatic gallstones and biliary stenosis. It should be noted that both procedures resulted in minimal recurrence of gallstones and cholangitis, whereas the T-tube insertion was less frequent in patients undergoing LHD cholangioscopy. This advantage contributes primarily to the shorter operative time of the LHD approach compared with that of the CBD approach. Furthermore, the insertion of the cholangioscope via the CBD requires dissection of the CBD, whereas this procedure can be easily completed through the preexisting bile duct stump in the LHD approach. This fact also results in reduced operative time of the LHD approach and may decrease the procedural complications associated with CBD dissection. In terms of other common complications, however, the two procedures of intraoperative cholangioscopy were comparable.
Accurate preoperative imaging evaluation is the prerequisite to laparoscopic cholangioscopy through the LHD orifice. 24 The applicability of such a procedure depends on the intra-/extrahepatic biliary architecture and the site of stenosis. First, the LHD orifice should be free of any marked stricture. Second, in the case of concomitant cholelithiasis, choledocholithiasis, or right-sided hepatolithiasis, the right liver parenchyma should not show any atrophy and should not require resection of the right lobe. Last, the lower segment of the CBD should remain patent, and no biliary enteric anastomosis should be required to reconstruct the biliary outflow.
It should be noted that laparoscopic cholangioscopy through the LHD orifice has some limitations. In the case of a fine or strictured LHD orifice, insertion of the cholangioscope through the LHD orifice cannot reach the CBD smoothly. Additionally, a large-size extrahepatic gallstone cannot be removed through the LHD stump. Concomitant cholangitis and pancreatitis contraindicate the use of this technique because of the risks of aggravated and disseminated infections. The absence of a T-tube may well require a repeated choledochotomy, although residual gallstones rarely are present. Thus, we recommend that a T-tube should be inserted in the case of excessive right-sided hepatolithiasis. Bile leakage from the stump is likely to occur in the case of lower CBD stricture in the absence of a T-tube, which is a definitive modality of biliary decompression.
In conclusion, cholangioscopy via the LHD orifice is more technically feasible in comparison with conventional choledochotomy for the laparoscopic treatment of LSH. This technique significantly decreases the operative duration but does not require T-tube insertion in most cases. Patients benefit mainly from an accelerated recovery and a shortened length of hospitalization. As an effective and safe technique that is comparable to choledochotomy, LHD cholangioscopy is a preferred alternative to choledochotomy in the laparoscopic treatment of LSH. A prospective randomized controlled trial is being planned to justify the use of intraoperative cholangioscopy via the LHD approach in LSH patients undergoing laparoscopic hepatectomy in order to minimize the occurrence of residual gallstone disease and the requirement of T-tube placement.
Footnotes
Acknowledgments
We acknowledge Medjaden Bioscience Ltd. and Prof. Duo Li from Aerospace Central Hospital for their valuable lingual assistance in the preparation of this manuscript.
Disclosure Statement
No competing financial interests exist.