
Abstract
Abstract
Purpose:
Using barbed suture represents a novel technical modification in the performance of minimally invasive partial nephrectomy. Our purpose of this study was to evaluate the safety and efficacy of this suture for renorrhaphy during laparoscopic partial nephrectomy (LPN).
Patients and Methods:
Thirteen consecutive patients underwent LPN using V-Loc™ 180 (Covidien, Dublin, Ireland) suture, and a nonconsecutive control group of 24 patients, matched according to tumor size and R.E.N.A.L. nephrometry score, underwent LPN using absorbable polyglactin suture. All 37 patients underwent LPN performed by a single surgeon. Perioperative and postoperative indicators of morbidity, estimated blood loss, and warm ischemia time (WIT) were compared between the groups.
Results:
Baseline characteristics including age, body mass index, American Society of Anesthesiologists score, tumor size, laterality, and R.E.N.A.L nephrometry score were identical between the groups. On multivariable analysis, there were no significant differences between the two groups with regard to operative time, estimated blood loss, transfusion rates, rates of surgical complications, and length of hospital stay. However, mean WIT was significantly shorter in the V-Loc group compared with the control group (24.5±5.3 minutes versus 31.9±8.9 minutes, P=.01).
Conclusions:
The use of V-Loc sutures for renorrhaphy during LPN is safe and feasible and, in our series, significantly reduces WIT. Further studies are needed to corroborate these findings, but these results indicate a promising development in reducing WIT during minimally invasive partial nephrectomy.
Introduction
Unidirectional barbed suture is a novel suture material that resists backsliding, eliminating the need to maintain constant tension on the suture during renorrhaphy. Unidirectional barbed suture material has been used for the vesicourethral anastomosis during robotic-assisted radical prostatectomy, where its use has been reported to decrease time while maintaining integrity of closure. 6 The application of unidirectional barbed suture materials to renorrhaphy during partial nephrectomy has been recently reported, but these reports either introduce the technique without an evaluation of efficacy or involve robot-assisted partial nephrectomy, which is less technically difficult than conventional laparoscopic surgery, and thus the differences between using and not using a barbed suture may not be as noticeable.7–9
Therefore, the objective of this study is to evaluate the safety and efficacy of unidirectional barbed suture material for renorrhaphy during LPN through comparative analyses with conventional renorrhaphy using absorbable polyglactin.
Patients and Methods
In total, 37 patients who underwent a LPN performed by a single surgeon (B.I.C.) between May 2007 and December 2011 were enrolled in this study. Institutional review board approval was obtained before initiating the study. Exclusion criteria included unclamped partial, solitary kidney, multiple tumors, or those cases as part of a joint surgery.
A transperitoneal approach was used in all cases. An open-ended ureteral catheter was inserted and connected to a syringe filled with dilute indigo carmine for identification of the collecting system entry. Ports included a 12-mm camera port placed at the level of the umbilicus level along the lateral border of the rectus abdominis muscle and two additional 12-mm ports placed along the same line at the subcostal and lower quadrant level, respectively. For right-sided cases, another 5-mm port was placed at the subxiphoid area to retract the liver. Tumor identification and demarcation of tumor margin were based on intraoperative ultrasound performed by a radiologist in all cases, and the line of resection was scored on the kidney capsule with electrocautery. After instillation of 12.5 g of mannitol, clamping of the renal vessels was done by either laparoscopic bulldog clamps or a Satinsky clamp. Tumor excision was completed with cold scissors alone.
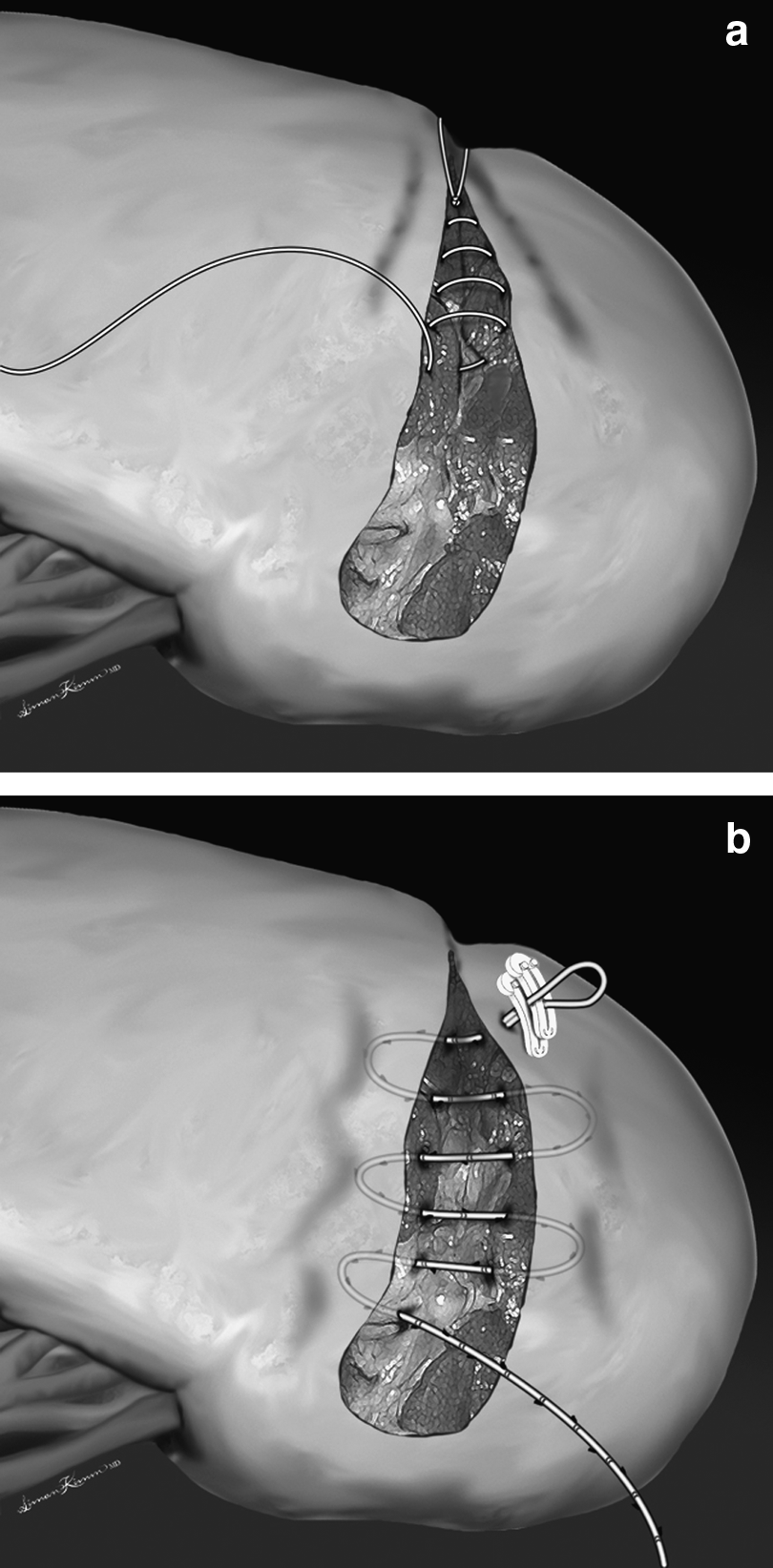
The patients were divided into two groups based on the renorrhaphy technique. In Group 1, one or more 15-cm-long running 0-polyglactin sutures on a CT needle were used to repair the parenchyma resection defect and, when necessary, the collecting system. An additional running or interrupted 0-polyglactin or 1-polyglactin suture was used for any additional hemostasis. In Group 2, a 15 cm-long V-Loc™ 180 (Covidien, Dublin, Ireland) suture anchored with two Hem-o-Lok clips (Weck® Surgical Instruments, Teleflex Medical, Durham, NC) at the tail end was used to hemostatically suture the parenchymal cut edge (Fig. 1). The initial suture was started on the outside of the kidney, through the capsule, and came out on the inside of the parenchyma; this suture was run from top to bottom throughout the tumor bed, and the last throw exited the capsule and parenchyma and was secured by two Hem-o-Lok clips (Fig. 2). A second outer layer was run in the same fashion continuously through and through the parenchyma with the same V-Loc 180 suture material, with each stitch exiting the parenchyma on both sides. The purpose of this stitch is to fold over the parenchyma onto the defect. Dilute indigo carmine solution was injected retrograde in both groups to identify the collecting system entry, allowing watertight suture closure, prior to completion of the renorrhaphy. A biological hemostatic agent was applied as an adjunctive hemostatic measure. The vascular clamp was removed, and both hemostasis and global kidney perfusion were confirmed.
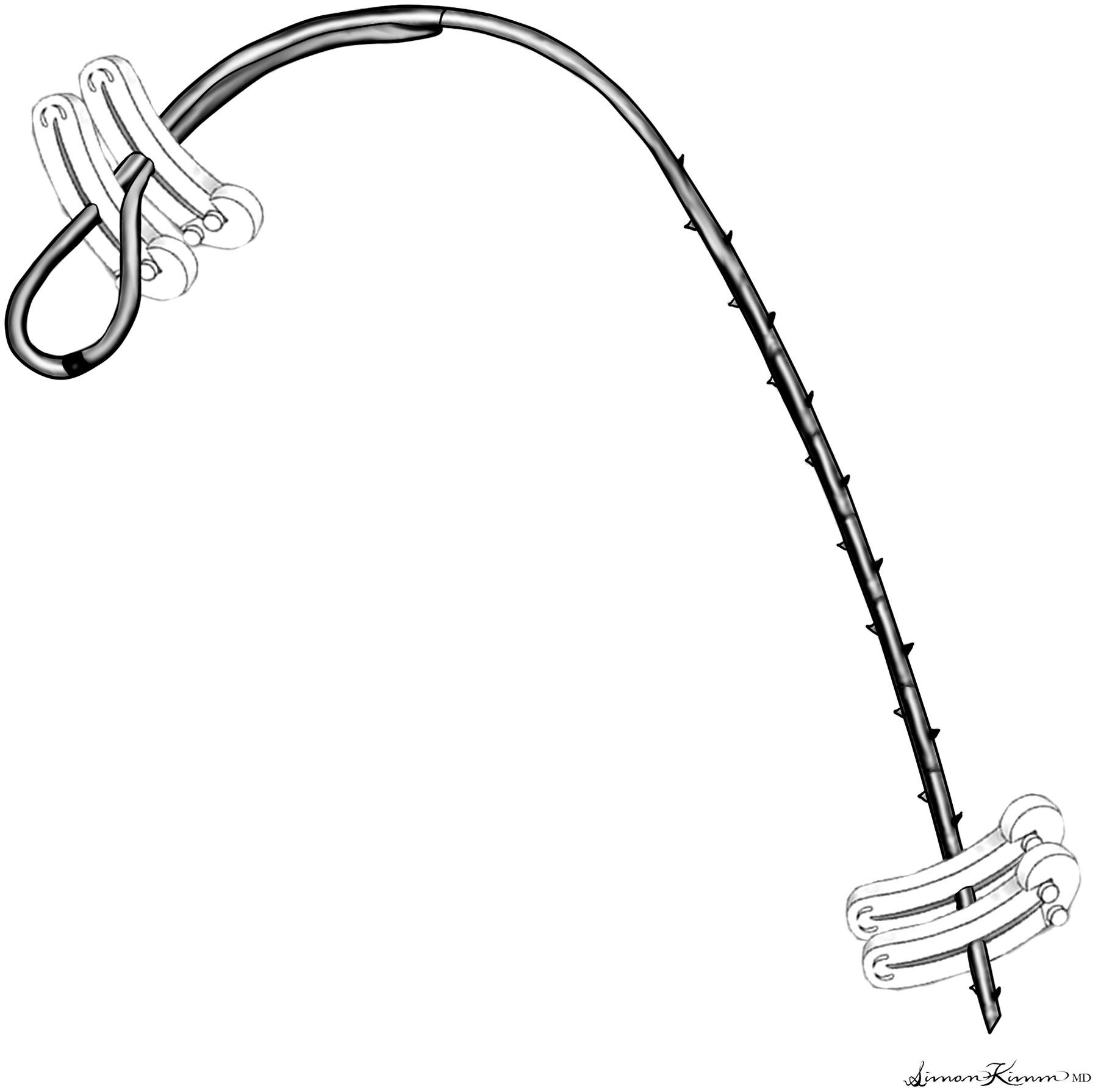
Hem-o-lok clip placement locations on the V-Loc suture. One clip goes through the loop, and the second is placed where the loop becomes a single strand. The suture is secured at the other end with two Hem-o-lok clips to prevent any slippage.
Patient baseline demographic characteristics, tumor size, estimated blood loss, WIT, and postoperative morbidity were compared between the two groups. Also, to evaluate and compare the baseline difficulty of each case, we used the R.E.N.A.L nephrometry scoring system, 10 as well as the presence of entry into the collecting system and vascular complexity, the latter of which is determined by the number of renal hilar vessels. Continuous variables were compared using Student's t test, and categorical variables were compared using the chi-squared test. A P value of <.05 was used to determine statistical significance for all comparisons. Analyses were done using the SPSS version 18.0 statistical software package (SPSS Inc., Chicago, IL).
Results
Group 1 comprised a nonconsecutive control group of 24 patients undergoing standard LPN renorrhaphy matched by body mass index, American Society of Anesthesiologists score, tumor size, laterality, and R.E.N.A.L nephrometry score to Group 2, which consisted of 13 consecutive patients who underwent LPN with renorrhaphy completed with barbed suture (V-Loc 180 suture) (Table 1). Intraoperative and postoperative outcomes are shown in Table 2. There were no significant differences between the two groups regarding mean operative time, estimated blood loss, transfusion rates, renal vascular complexity, collecting system entry, surgical complications, and hospital stay. However, mean WIT was significantly shorter in Group 2 compared with Group 1 (24.5±5.3 minutes versus 31.9±8.9 minutes, P=.01). There was 1 case of margin positivity in Group 2, but it was a case of benign angiomyolipoma, diagnosed on frozen section, and no additional treatment was required. Table 3 lists the postoperative surgical complications, which showed no significant difference in overall rates. Postoperative urine extravasation was managed conservatively in all cases. No case required a return to the operating room or loss of a renal unit.
ASA, American Society of Anesthesiologists; BMI, body mass index; L, left; R, right.
EBL, estimated blood loss; WIT, warm ischemia time.
Data are number of patients (%).
Discussion
Open partial nephrectomy has become the gold standard treatment for small localized renal cell carcinoma by providing oncologic outcomes comparable to radical nephrectomy while preserving renal function and minimizing cardiovascular morbidity.11,12 LPN is a newer technical modification that has shown comparable oncologic outcome while providing the minimally invasive benefits such as a shorter hospital stay, decreased convalescence, and improved cosmesis. 13 However, unlike laparoscopic radical nephrectomy, adoption of LPN has been slowed in large part by the very high level of technical expertise needed to perform the procedure, 14 especially sufficient facility in intracorporeal suturing to accomplish secure hemostasis and renal reconstruction within an acceptable WIT. A recent report comparing 1800 contemporary patients undergoing open partial nephrectomy and LPN from an experienced cohort of surgeons showed a 10-minute longer WIT in the LPN group, underscoring the inherent difficulty of the procedure. 15 Furthermore, unlike total operative time, which decreases with increasing experience, WIT does not experience a decrease 16 but is correlated with multiple factors such as case complexity and suture methodology as well as proficiency. It can be challenging and time-consuming even for an experienced laparoscopic surgeon to manipulate the needle and proceed with reconstruction with one hand while maintaining the suture tension with the nondominant hand throughout the procedure. Robot-assisted LPN (RPN) is a newer minimally invasive option to overcome the technical difficulties of LPN, namely, intracorporeal suturing, but RPN has been criticized for an excessive dependence on the bedside assistant and cost. 17
Barbed suture material has been introduced to obviate the need for knots by incorporating tiny barbs spaced evenly in a helical array on the suture, creating a self-anchoring knotless suture. 18 It is reported that the use of barbed suture material in LPN or RPN can shorten WIT by 19.5%–25.1%.8,19 In our study, the decrease in WIT shown was 7.4 minutes (23.2%). There are likely several reasons for this, including eliminating the need for both knot tying and maintaining constant tension on the nonbarbed suture, freeing up both hands for intracorporeal suturing. In light of the criticisms of increased cost of RPN, 17 it is possible that the shorter WIT with barbed suture material could potentially mitigate this cost issue.
The safety and efficacy of barbed suture LPN have been sparsely reported in the literature. In the porcine model, with regard to hemostasis or integrity of collecting system closure, there appeared to be no benefit of barbed suture compared with conventional absorbable suture in the performance of polar partial nephrectomy or with suturing the ureteropelvic and urethrovesical anastomoses.9,20 In contrast, Olweny et al. 19 reported that the proportion of patients who experienced clinically significant bleeding after partial nephrectomy in the barbed suture group was fivefold lower than for the polyglactin group. One of the noteworthy findings of our study is that there was not a single instance of postoperative urine leakage in Group 2, whereas 12.5% of the patients in Group 1 had urine leakage postoperatively, despite both groups having had similar rates of collecting system entry (Table 2). This may be due to the ability to better fold the parenchyma over the defect with the barbed suture. Unlike the study from Olweny et al., 19 we did not find any significant difference in terms of postoperative hemorrhage between the two groups.
A few limitations in this study deserve comment. First, it is a retrospective nonrandomized study; however, cases and controls were matched and did not include cases early in the surgeon's career, to control for the learning curve. Also, it is possible that eliminating the knot tying was solely responsible for decreasing the WIT, and as the method of reconstruction between the barbed and non-barbed cohorts was not identical, a direct comparison cannot be made. However, considering that it takes about 1½ minutes to tie four knots (intraparenchymal top and end and parenchymal top and end, each 20 seconds in Group 1), the potential decrease in WIT is notable but unlikely to result by itself in the mean 7-minute decrease in WIT. However, in a nonbarbed suture sliding clip renorrhaphy, tension would still need to be maintained to the suture throughout the renorrhaphy, often necessitating single-handed needle manipulation, adding additional time.
Conclusions
The use of V-Loc sutures for renorrhaphy during LPN is safe and feasible and significantly reduces WIT. The use of V-Loc sutures did not increase postoperative morbidity after partial nephrectomy in our series. Further studies are needed to corroborate these findings, but the present results indicate a promising development in reducing WIT during minimally invasive partial nephrectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.