
Abstract
Abstract
Background:
Postoperative abdominal and shoulder pains after laparoscopic cholecystectomy (LC) are the most frequent complaints and are related to delayed recovery. There is a strong correlation between the residual gas volume and the severity of pain following various laparoscopic procedures. We aimed to investigate the effects of aspiration of residual gas on postoperative outcomes and pain following LC.
Subjects and Methods:
Patients were randomly assigned to either the active gas reduction group (Group 1, n=105) or the control group (Group 2, n=95). After completion of the operative procedures, residual gas was aspirated with a flexible cannula in Group 1. In Group 2, gas release from the abdomen was performed using the port site by opening the gas tap only. The demographic data, operation time, insufflated CO2 volume during the operation, hospitalization period, and time to return to daily activities were recorded. Postoperative shoulder and abdominal pain assessment was performed using a numerical pain intensity scale (NPIS) at 1 hour, 24 hours, 3 days, and 7 days postoperatively.
Results:
There was no statistically significant difference between the groups in terms of demographic data, operative findings, and clinical outcomes. NPIS scores for shoulder pain at 1 hour and 24 hours were significantly lower in Group 1 (P=.001 and P=.021, respectively). However, there were no significant differences in the NPIS scores for shoulder and abdominal pain following 24 hours. No differences were found in the hospitalization duration and time to return to daily activities data (P>.05).
Conclusions:
Active aspiration of the residual gas just before the removal of the trochars is a simple procedure and leads to a more comfortable hospital stay for patients.
Introduction
Early postoperative pain is the most common complaint reported following elective LC and is considered to be the major cause of delayed recovery.3,4 Most patients describe a transient and subjective pain in the shoulder, abdomen, or back. 5 It is thought that intra-abdominal pressure and retained intra-abdominal CO2 cause peritoneal stretching and diaphragmatic irritation. The latter is believed to be the cause of postoperative shoulder pain in approximately 30% of the patients undergoing LC. 6 It is also reported that there may be a strong correlation between the residual gas volume and the severity of pain following various laparoscopic procedures. 7 In our study, we aimed to investigate the effects of active gas aspiration on postoperative outcomes and pain following LC.
Subjects and Methods
This prospective randomized study was conducted in the Numune Training and Research Hospital, Adana, Turkey, between January 1, 2012 and August 1, 2012. Adult patients with symptomatic cholelithiasis who were eligible for LC were included in the study. Exclusion criteria were an American Society of Anesthesiologists score of 3 or 4, history of acute cholecystitis or pancreatitis, diabetes, and being on medication for chronic pain. In addition, patients who were converted to open cholecystectomy, required common bile duct exploration, or received any other perioperative additional procedures were excluded from the study. The trial protocol was approved by the institutional ethical committee, and written informed consent was obtained from all patients.
Patients were randomly assigned using the envelope method to either the active gas reduction group (Group 1) or the control group (Group 2) just before the operation.
The anesthesia technique was standardized in all patients. The patients were not premedicated. General anesthesia was induced with intravenous fentanyl (2 μg/kg) and propofol (2.0–2.5 mg/kg). Rocuronium (0.4–0.6 mg/kg) was given to facilitate intubation of the trachea.
Anesthesia was maintained with oxygen in air (1:1), remifentanyl (0.05–0.1 μg/kg), and sevofluarane (1%–2%). Ventilatory frequency was adjusted to maintain an end-tidal CO2 partial pressure of 4.5–5.5 kPa.
All patients underwent a standard LC with the North American four-port technique. The intra-abdominal gas pressure was set at a level of 12 mm Hg and monitored during the operation. After completion of the operative procedures and before the patients were placed in the supine position, residual gas was aspirated in Group 1. Aspiration was performed with a flexible cannula that is inserted through the most lateral accessory port and positioned in the subdiaphragmatic space. In Group 2, gas release from the abdomen was performed using the port site by opening the gas tap only without any additional effort for gas evacuation. No intra-abdominal drain was placed in any patients.
All patients were given a single use of antibiotic prophylaxis (cefuroxime, 750 mg) intravenously, and diclofenac sodium 75 mg was administered to all patients postoperatively.
The demographic data, body mass index, educational status, operation time, insufflated CO2 volume during the operation, hospitalization period, and time to return to daily activities were recorded. Postoperative shoulder and abdominal pain assessment was performed using an 11-point numerical pain intensity scale (NPIS), in which a rating of 0 indicated “no pain” and a rating of 10 indicated the “worst imaginable pain.” Pain assessment was administered by F.K., E.M., M.A., and H.E. to all patients in person. In order to blind the scorer, one of the aforementioned authors who was not assigned in the operation room was tasked. Following surgery, pain assessments were measured by the patients' bed at the end of 1 hour and 24 hours. All patients were kept overnight in the hospital. After discharge, all patients were administered NPIS by the same authors at the outpatient clinic on Days 3 and 7.
In addition to NPIS, patients were evaluated for postoperative complications and time to return to daily activities data at Days 3, 7, and 30. Absentees were reached by telephone regarding the aforementioned data.
Statistical analysis was performed using SPSS version 16 for Windows (SPSS, Inc., Chicago, IL). Data are mean±standard deviation values. Student's t test was used for detection of difference between the two groups. Differences were considered significant when P<.05.
Results
In total, 220 patients were included in the study. The patients with postoperative bilioma (n=2), atelectasis (n=3), subhepatic hematoma (n=3), and surgical site infection (n=7) were excluded from the study. Patients (n=5) who did not show up for follow-up also were excluded. Finally, 200 patients (47 men and 153 women) were included in the statistical analysis. The mean age was 48 years (range, 21–70 years). Group 1 included 105 patients, and Group 2 included 95 patients. There was no statistically significant difference between the groups in terms of demographic data, operative findings, and clinical outcomes (Table 1).
NPIS scores for shoulder pain at 1 hour and 24 hours were significantly lower in Group 1 (P=.001 and P=.021, respectively) (Fig. 1). However, there were no significant differences in the NPIS scores for shoulder and abdominal pain following 24 hours. No differences were found in the hospitalization duration and time to return to daily activities data (P>.05).
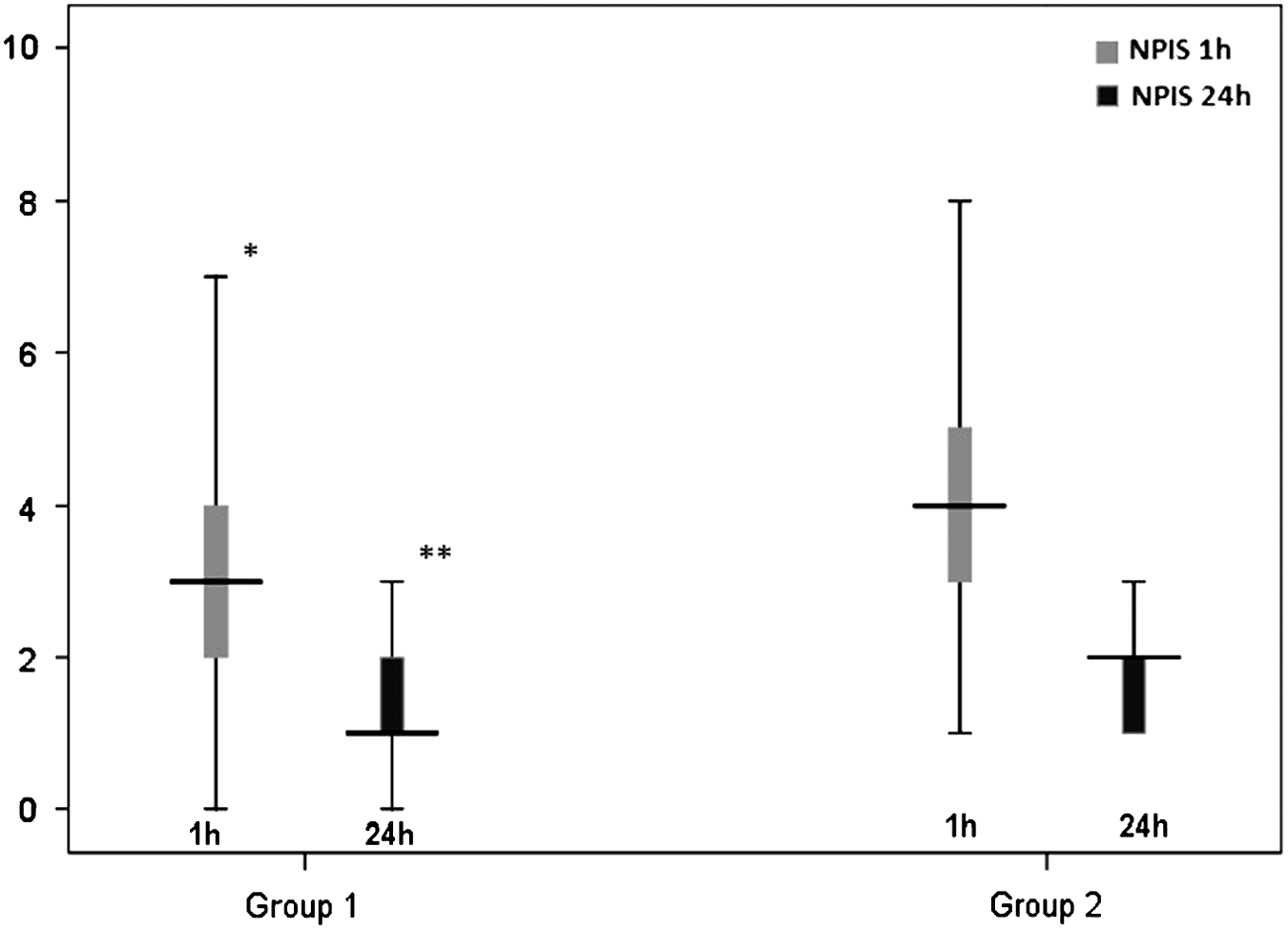
Differences in numerical pain intensity scale (NPIS) scores at 1 hour and 24 hours after laparoscopic cholecystectomy in the two patient groups. *P=.001, **P=.021.
Discussion
Currently LC is the gold standard for the treatment of symptomatic cholelithiasis. The main advantages of the procedure are less postoperative pain, shorter hospitalization duration, earlier return to daily activity or work, and better cosmetic results.1,2 Although LC has generally beneficial results, some unexpected adverse effects may occur because of the increase in intra-abdominal pressure or metabolic changes during CO2 pneumoperitoneum. These parameters have more significant effects on the cardiovascular and respiratory systems.8,9 They are usually self-limited and do not cause severe morbidity or mortality. 10 In addition to these effects, comfort of the patients in the postoperative period still constitutes an important area needing improvement. The pain following a minimally invasive procedure is an important problem for the patient.
Postoperative abdominal and shoulder pains after LC are the most frequent complaints and are related to delayed recovery.6,11 The mechanism of pain is believed to involve diaphragmatic stretching during pneumoperitoneum, 12 the volume of gas insufflation, 13 and the temperature of the gas. 14 It is reported that the major causes of shoulder pain are related to stimulation of intraperitoneal nerve endings due to the increase in intra-abdominal pressure, temperature of the gas, and acidification due to carbonic acid, which results from CO2. 15
Jackson et al. 7 analyzed the relation between post-laparoscopy pain and residual CO2 before discharge. In the study, abdominal X-ray studies were analyzed for measurements of the volume of the gas bubble on the right subdiaphragmatic area. They reported statistically significant correlations between the volume of gas bubble and the pain score and stated that residual gas could be a major cause of post-laparoscopy pain. 7 Atak et al. 16 showed that active aspiration at the end of the laparoscopy effectively reduced residual CO2 volume, the frequency of shoulder pain, and the need for postoperative analgesics at the end of 24 hours. Nursal et al. 17 studied the effects of subdiaphragmatic gas drain, which is expected to decrease the residual gas volume on postoperative pain, nausea, and vomiting after LC in a prospective randomized study; however, they observed that evacuation of gas after surgery did not necessarily decrease the pain and vomiting in their limited number of patients. Unlike the above-mentioned studies, in our study, patients were followed up for a week and researched for positive effects of gas aspiration on pain perception. The positive effect detected within the first 24 hours was not observed in the following days, and there were no difference regarding return to daily activities.
In conclusion, we found that the postoperative shoulder pain was significantly lower in the aspirated patient group in the first 24 hours. Therefore, we suggest that active aspiration of the residual gas just before the removal of the trochars is a simple procedure and leads to a more comfortable hospital stay for patients.
Footnotes
Disclosure Statement
No competing financial interests exist.