
Abstract
Abstract
Background:
Laparoscopic renal cyst decortication often uses three-port incisions or single-port incision with three or four channels (laparoendoscopic single-site surgery). This article introduces a modified laparoendoscopic single-site surgery for the treatment of simple renal cysts: single-channel retroperitoneal laparoscopic decortication (SCRL) of a simple renal cyst.
Patients and Methods:
From January 2008 to December 2011, either SCRL or standard three-port–incision retroperitoneal laparoscopic decortication (SRL) was performed for the treatment of a simple renal cyst. The SCRL procedure was as follows. The patients were placed in the lateral decubitus position. A 1.2-cm horizontal skin incision was made over the midaxillary line, 3 cm above the iliac crest. The retroperitoneum working space was established. A 10-mm operative laparoscope, which is similar to a nephroscope, was introduced into the retroperitoneum cavity through a 1.1-cm port. The cyst was exposed and then sutured to help to suspend the cyst wall so that the cyst could be decorticated easily. Perioperative and follow-up data from SCRL and SRL were collected retrospectively.
Results:
Based on the cyst location as the major selection criterion, 92 cases were enrolled for further analysis. Of these, 38 patients were treated with SCRL, and 54 patients were subjected to SRL. No SCRL was converted to SRL, and no SRL was converted to open surgery. The operation time and the drain tube removal time in these two approaches were similar (P>.05), but the average duration of hospital stay in the SCRL group was shorter (P=.02). Six months after the surgery, renal ultrasound results showed that the diameter of the cyst in these two groups also had no significant difference (P>.05).
Conclusions:
With appropriate selection of patients, the SCRL approach has the same efficacy with better cosmesis compared with SRL.
Introduction
A symptomatic renal cyst can be treated by the following strategies: percutaneous aspiration with or without sclerosants,4–6 surgical deroofing including open surgery, 2 percutaneous decortication, 7 and laparoscopic surgery,8–13 and other methods such as anterograde 14 or retrograde3,15 endoscopic marsupialization. More recently, laparoendoscopic single-site surgery (LESS)13,16,17 and even robotic-assisted laparoscopic decortication have also been applied in the treatment of simple renal cysts.
Currently, laparoscopic renal cyst decortication by the transperitoneal10,18 or retroperitoneal10,12,18 approach is the most preferred choice, but it still requires three- or four-port access. Although LESS can reduce the number of ports used for access and gain the same results as the standard laparoscopic procedure, it usually requires a special port and manipulating instruments and is more technically challenging for the surgeon.13,16,17
Here we report our initial experience and outcomes with a modified LESS technical single-channel retroperitoneal laparoscopic decortication (SCRL) for the treatment of a simple renal cyst. This modified LESS technology combined the conventional laparoscopic appliance together with the LESS technology, proved to have the same efficacy as standard three-port–incision retroperitoneal laparoscopic decortication (SRL) with improved cosmesis, and needed no other special equipment, and it can also be performed by any surgeon who has standard retroperitoneal laparoscopic experience.
Patients and Methods
From January 2008 to December 2011, 255 cases of simple renal cyst were treated with either SCRL or SRL at the authors' department. In order to compare the feasibility and outcomes of SCRL with SRL, we retrospectively collected the data according to the following criteria: (1) the operation was performed by one of two surgeons who can simultaneously perform SRL and SCRL (D.Y. and B.X.) so as to exclude the influence of the learning curve; (2) the cyst score is only Bosniak class 1–2; and (3) the location of the cyst is in the pole of the kidney or the lateral side. Surgery on those with a Bosniak class 3–4 renal cyst, a cyst located to the parapelvic region, or multiple cysts and obese patients was also performed by these two methods, but their results were excluded from analysis. All patients provided written informed patient consent and were evaluated with urine analysis, urine culture, renal ultrasound, and abdominal computed tomography.
Operation procedure
SCRL
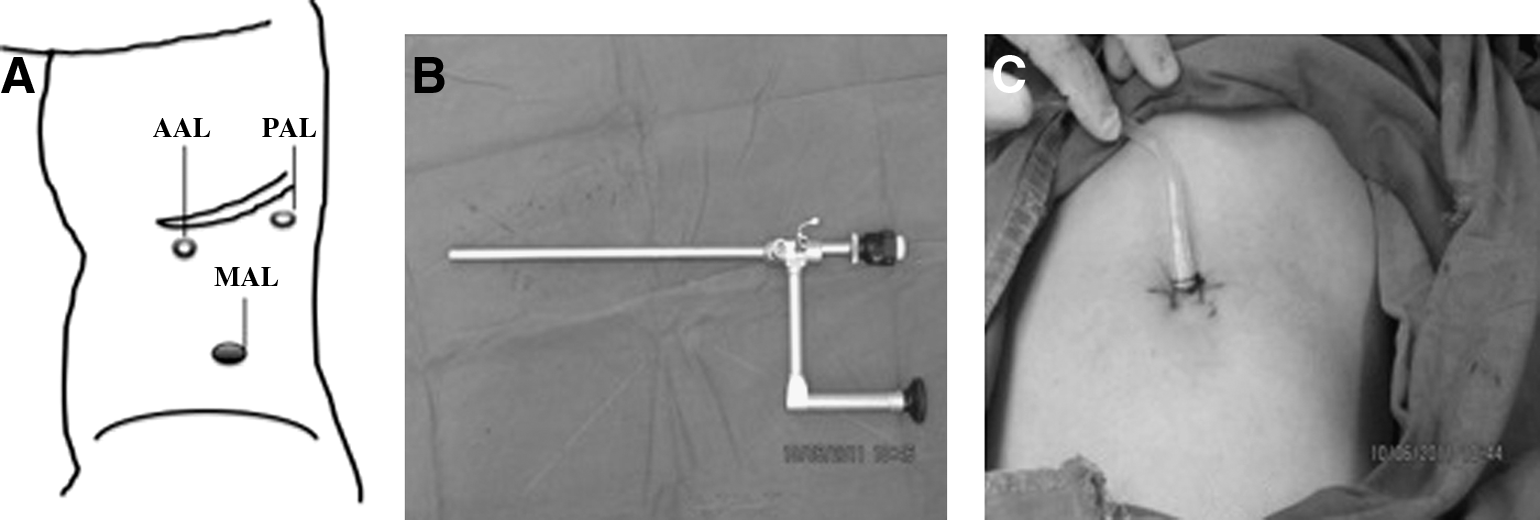
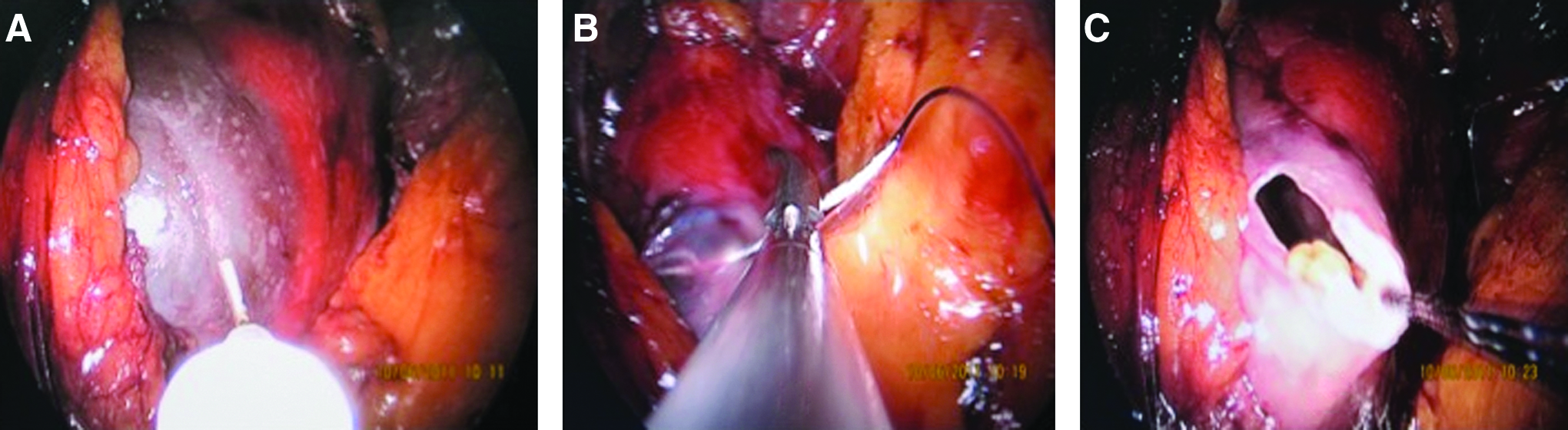
After the induction of general endotracheal anesthesia, the patient was placed in the lateral decubitus position and fixed on the operating table with all pressure points well padded. Then a 1.2-cm horizontal skin incision was made over the midaxillary line, 3 cm above the iliac crest (Fig. 1A). The underlying musculature was spared by blunt dissection with a hemostat. The retroperitoneum working spaces were established by blunt separation with a finger. Then a trocar 1.1 cm in diameter was inserted, and the incision was closed around the trocar using a suture to prevent gas leakage. A 10-mm operative laparoscope (Karl Storz, Tuttlingen, Germany) with a 6-mm working channel (Fig. 1B), which is similar to a nephroscope, was introduced through this trocar. A CO2 pneumoretroperitoneum of 12–15 mm Hg was obtained. A laparoscopic hook electrode or suction was inserted as needed. A combination of blunt and sharp dissection of the renal fascia was used until the cyst was recognized (Fig. 2A). Then two modified methods were used to help exploring and suspending the renal cyst. (A) A position in the posterior axillary line below the costal was selected to puncture a straight needle with 2-0 silk thread into the retroperitoneal cavity. The tail of the thread remained outside, then the cyst was sutured, and the needle was passed out through the cavity. The assistant surgeon pulled the thread to help expose the cyst wall. (B) The needle was inserted into the retroperitoneal cavity through the trocar channel, and the cyst was sutured (Fig. 2B). The needle was pulled out through the trocar to help suspend the cyst (Fig. 2C). The cyst was decorticated, and the cyst fluid was aspirated. The edges and base of the residual cyst wall were thoroughly examined and fulgurated. A 12 French closed drain was left in the retroperitoneal space through the trocar, and the skin incision was sutured (Fig. 1C). The entire cystic wall was subjected to histopathological examination to exclude malignancy.
SRL
The standard retroperitoneal laparoscopic procedure were performed as described elsewhere. 18 In brief, a 1.0-cm transverse skin incision was made over the midaxillary line, 1.5 cm above the iliac crest. The underlying musculature was spared by hemostat, and the retroperitoneal cavity was blunt-dilated. A Hasson trocar was inserted, and another two 5-mm trocars were inserted in the anterior and posterior axillary lines below the costal under laparoscopic direction (Fig. 1A). The renal fascia was dissected until the cyst was recognized. Then the cyst wall was punctured by electrocautery, the cyst fluid was aspirated, and the wall was resected with a laparoscopic hook electrode up to the limit of the normal renal parenchyma edges. The cystic cavity was thoroughly examined to exclude the presence of neoplastic changes. A drain tube was inserted through the trocar in the posterior axillary line incision.
All the patients were followed up in the outpatient clinical at regular intervals, and the pre- and postoperative symptoms were evaluated. The cyst was examined by ultrasonography after 6 months.
Statistical analysis
Clinical characteristics were recorded and compared between the SCRL and SRL groups. All the data were analyzed with GraphPad (San Diego, CA) Prism® version 6.0 software by using an unpaired t test. A value of P<.05 was considered to indicate statistical significance.
Results
According to the selection criteria, 92 cases were included for further analysis. Of these, 59 patients complained flank pain, 8 patients had hematuria, 15 patients had renal obstruction, and 10 patients had recurrent urinary infection. Thirty-eight patients were treated with SCRL, and 54 patients were subjected to SRL (Table 1). There was no significance difference between the patients' age in these two groups, but the average cyst diameter in the SCRL group was larger than that in the SRL group (7.58±0.33 versus 6. 52±0.18; P=.003).
The single-channel retroperitoneal laparoscopic decortication (SCRL) and standard three-port–incision retroperitoneal laparoscopic decortication (SRL) values are statistically significantly different (P<.05).
No SCRL was converted to SRL, and no SRL was converted to open surgery. The pathologic results revealed benign renal cysts.
The perioperative data of these two groups are also shown in Table 1. The mean operation time and the mean drain tube removal time are similar (P>.05). No obvious complications in these two groups were observed. The average duration of hospital stay in the SCRL group was shorter than that in the SRL group (3.76±0.12 days versus 4.20±0.13 days, respectively; P=.02). Six months after the surgery, the symptoms had all disappeared, and renal ultrasonography results showed that the diameter of the cyst in these two groups (SCRL versus SRL) to be 1.2±0.04 cm and 1.3±0.05 cm, respectively, which are not significantly different (P>.05).
Discussion
The main target for the treatment of symptomatic simple renal cysts is to excise the cyst wall and evacuate its fluid contents so as to decompress the renal parenchyma subjected to the enlargement of the cyst. Before the 1980s, open renal cyst ablation was the only choice. 3 This method requires a large flank or abdominal incision and is eventually replaced by less or minimally invasive therapeutic approaches.
Percutaneous aspiration with sclerosant was another choice. 6 Compared with open surgery, percutaneous aspiration with sclerosant is much less invasive. However, the results of simple aspiration are associated with very high recurrence rates (up to 90%). Although many different sclerosant agents have reportedly been used for this purpose, this technology still has a high rate of cyst recurrence (54%) and the risk of collecting system strictures, which are caused by severe perirenal inflammation secondary to extravasation or inadvertent instillation of the sclerosant into the retroperitoneum.1–6
Other percutaneous marsupialization, either by creating a directly percutaneous access to the cyst (percutaneous decortication) 7 or by creating an indirect nephrostomy tract through a nearby calyx and approaching the cyst from inside the collecting system, has also been described. Percutaneous decortication also uses fulguration at the base of the cyst and incises the dome of the cyst, which is theoretically similar to the method used in open surgery or laparoscopy. This method is more suitable for posterior cysts with large lateral margins instead of the anterior–medial cysts without compromising the renal parenchyma. As the percutaneous incision proceeds, however, the collapsing cyst impairs visibility, and this may lead to difficulty in management of the bleeding, inefficient incision, or inadvertent injury of the collecting system. 7
Indirect percutaneous access,2,3 which is similar to retrograde ureteroscopic marsupialization, was first reported in 1991. In these two procedures, the cyst wall is incised to create communication between the cyst and the collecting system. Compared with retrograde ureteroscopic marsupialization, antegrade percutaneous nephroscopy needed an additional percutaneous access, which can increase the risk of puncturing injury. The advantage of retrograde ureteroscopic marsupialization is when you combine the flexible ureteroscope with the holmium laser, it can help to gain access to almost all areas of the collecting system under direct vision. 3 However, antegrade access is more suitable for large lateral margin posterior cysts, and the retrograde approach is particularly suitable for those simple renal cysts that are adjacent to the collecting system, especially those with extrinsic compression causing them to protrude into the collecting system.
Laparoscopic decortication of a symptomatic renal cyst 19 was first described in 1993. This technology has eventually become the first choice for the treatment of a simple renal cyst. Compared with open surgery and percutaneous aspiration and sclerotherapy, laparoscopic decortication duplicates almost all the steps of the open procedure, but it is less invasive and safer than open surgery; however, it is a little more invasive than percutaneous decortication or aspiration because it requires three or even four incisions for trocar insertion.2,9,10,11 However, it can be more effective when multiple, peripelvic or bilateral renal cysts exist. The recurrence rate for this technique was about 19%, as determined by analysis of follow-up data covering 67.2 months, 20 which is far lower than that of percutaneous aspiration with sclerosant (54%) and percutaneous decortication. 7
Recently, there has been immense interest in both the LESS and the natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and the Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) approaches to minimize invasive urological surgery.13,16,17,21 The single undisputed benefit of LESS and NOTES is improved cosmesis by the single-access port. However, the overall length of the incision for the port is almost 4–5 cm long, which is almost equal to that of the standard laparoscopic procedure. On the other hand, LESS and NOTES require a specially designed single port, such as the R-Port™, Quadriport™ (both from Advanced Surgical Concepts Ltd., Bray, County Wicklow, Ireland), or the Uni-X™ (PNavel Systems, Cleveland, OH) 17 and special articulating or prebent laparoscopic instruments to reduce intracorporeal instrument collision caused by the spatial constraints of single-port access.13,16,17
On the basis of our experience with the retroperitoneal approach and inspired by LESS technology, we applied a 10-mm operative laparoscope with only a 6-mm working channel to perform SCRL. This modified LESS technology needs no extra specific flexible instruments because all the marsupialization was done in turns instead of simultaneously. This is the key point to prevent instrument collision, which is the main drawback of LESS. From the best cosmetic point of view, we also used the transperitoneal approach. However, this approach has to violate the peritoneal cavity and mobilize the colon, which could contribute to adhesion formation because there have been reports indicating that adhesion rates as high as 22.2% occurred after an initial transperitoneal urologic laparoscopic procedure. 22 So we prefer the retroperitoneal approach to perform SCRL.
However, when the cyst located at the anterior–medial portion of the kidney, the procedure is time consuming. Currently, no matter where the cyst location is, we perform SCRL as a standard surgical strategy for simple renal cysts, most of which are not suited for percutaneous or retrograde marsupialization. However, SCRL still has a limited operative field compared with SRL and requires the surgeon having more skillful experiences with SRL.
In conclusion, this modified LESS technology, which we termed SCRL, is feasible, safe, effective, and minimally invasive. It is recommended for consideration before other minimally invasive laparoscopic or open surgical approaches are applied.
Footnotes
Disclosure Statement
No competing financial interests exist.