
Abstract
Abstract
Background:
The improvement in intracorporeal anastomotic techniques and the consequent switch from a laparo-assisted (LA) to a totally laparoscopic (TL) right colectomy seem to have overcome the initial concerns, giving rise to the widespread use of such a procedure. By comparing the LA and TL approaches, our study was aimed at verifying the possible advantages of the more recent technique, while also focusing on some technical implications for the surgeon.
Subjects and Methods:
We prospectively collected and matched data from 27 consecutive LA right colectomies and 28 consecutive TL right colectomies (TLRCs). Clinical, biochemical, pathological, and cosmetic parameters were examined. Operating times were recorded and analyzed, in order to evaluate the learning curve for the different phases of the procedure.
Results:
The LA and TL groups were homogeneous for demographic and pathological features. We had no mortality, and surgical complication rates were similar (3.6% versus 3.7%). The TLRC group presented a significantly shorter laparotomy (4.8 cm versus 7.2 cm, P=.002), whereas no significant difference was recorded for outcome parameters. Operating time for carrying out anastomosis was significantly longer for the TL group (55.6 minutes versus 20.6 minutes, P<.0001). A rapid decrease in anastomosis time throughout the series attests to a short learning curve for intracorporeal ileotransverse anastomosis.
Conclusions:
Further studies are needed to demonstrate possible clinical advantages of TLRC over the LA approach. The cosmetic benefit for patients along with safety and the prospective usefulness for surgeons (practice in intracorporeal suturing techniques) would seem to justify an inclination toward this technical development.
Introduction
Laparoscopic right colectomy was first developed as a laparo-assisted (LA) procedure: the necessity of performing an extracorporeal anastomosis implied the use of a service laparotomy, usually not much shorter than a standard laparotomy. As was somewhat predictable, the only studies that compared open and LA right colectomies (LARCs) failed to demonstrate clear advantages for the minimally invasive approach, or else they presented important flaws and bias.8,9 The development of intracorporeal suturing techniques, mainly related to the wide diffusion of bariatric procedures, led to renewed enthusiasm for laparoscopic right colectomy, as it was finally performable as a totally laparoscopic (TL) procedure.
Many studies comparing open right colectomies, LARCs, and TL right colectomies (TLRCs) have recently been published.10–14 As frequently happens with “appealing” technical innovations, most of the reports present a serious selection bias or “immature,” nonconclusive data. By presenting our preliminary experience of this technical switch, our aim is to focus also on what intracorporeal anastomosis has entailed for the surgeon, in anticipation of a definitive, or at least clearer, solution for the patient.
Subjects and Methods
We prospectively collected data from LARCs and TLRCs performed at our institution from January 2006 to July 2010. All the procedures were performed by the same surgical team, experienced in minimally invasive abdominal surgery. Urgent setting, previous midline laparotomies, T4 lesions, peritoneal carcinosis, American Society of Anesthesiologists score of 4, or severe general contraindication to pneumoperitoneum was considered as an exclusion criterion, and those patients were treated by an open procedure (Fig. 1). Since the first intracorporeal anastomosis was performed (February 2008), no further extracorporeal reconstruction has been carried out. Twenty-seven patients in the LA group and 28 in the TL group were ultimately enrolled for the statistical analysis. The study was approved by the Institutional Review Board, and informed consent was obtained from all participants.
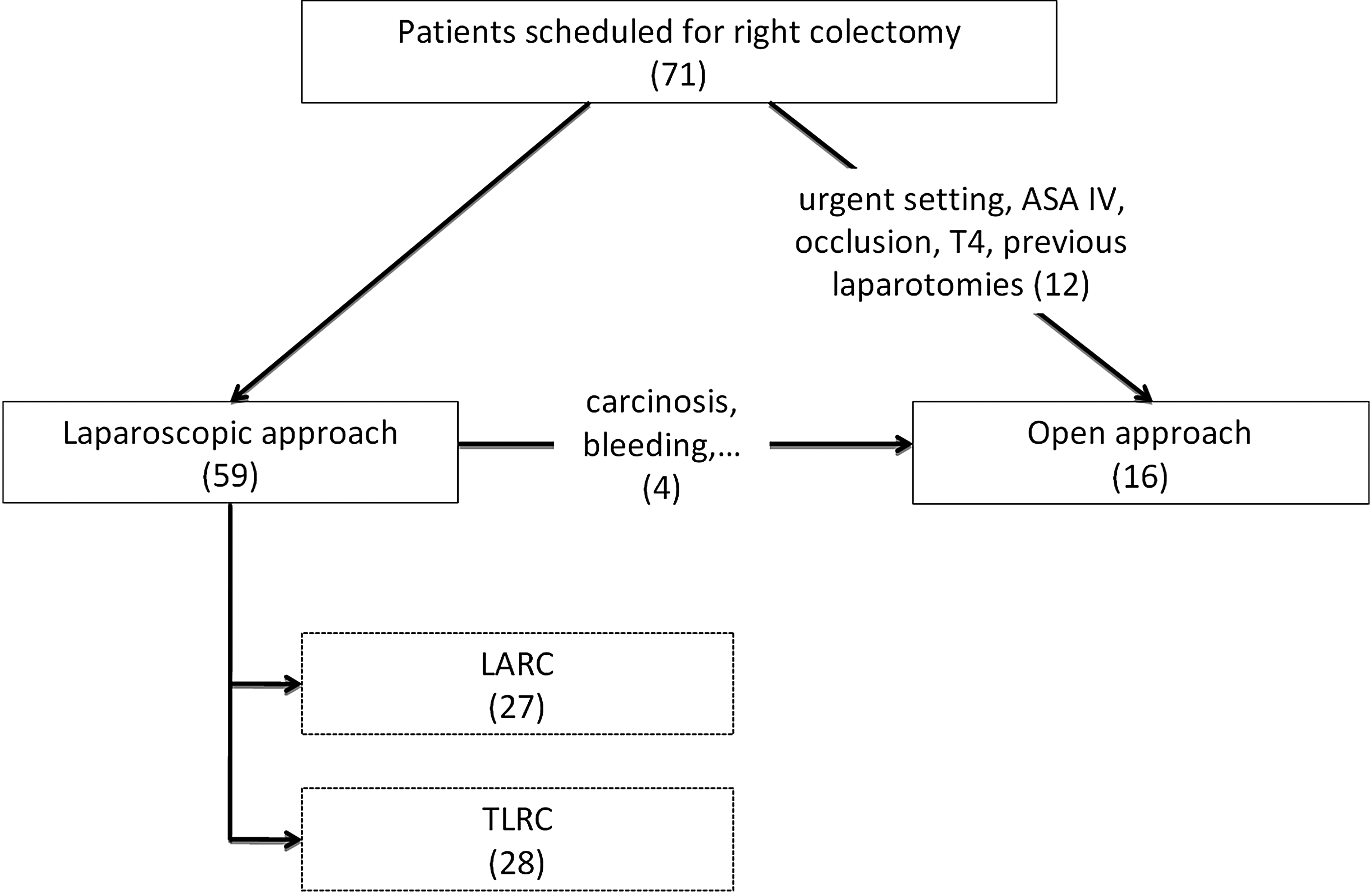
Patient selection. ASA, American Society of Anesthesiologists; LARC, laparo-assisted right colectomy; TLRC, totally laparoscopic right colectomy.
Preoperative study always included a thoraco-abdomino-pelvic computed tomography scan. All lesions located more than 5 cm distal to the ileocecal valve were endoscopically tattooed (with Indian ink), and the colonoscopy was repeated if the lesions were not marked at the time of biopsy. All the patients received intravenous antibiotic prophylaxis with 500 mg of metronidazole and 3 g of ampicillin/sulbactam and subcutaneous administration of low-molecular-weight heparin prior to surgery (dalteparin sodium, 35 IU/kg of body weight). A mechanical bowel preparation with macrogol (polyethylene glycol) was performed 2 days before surgery; symeticone (15–20 tablets) was administered the day before surgery, in order to possibly reduce bowel distension.
LARC
All the patients were approached from the left side. Pneumoperitoneum was induced by a Veress needle in the left subcostal space and kept at 12 mm Hg. A 12-mm optic trocar was then inserted in the left hemiabdomen, approximately 5 cm laterally from the midline and 8 cm cranially to the umbilicus. A second one was then inserted on the same line as the first at the level of the umbilicus. Two more 5-mm trocars were inserted on the McBurney's point and on the midline, 8 cm caudally to the umbilicus (Fig. 2). The patient was initially placed in a 10–20° anti-Trendelenburg position, with 20–30° left flank rotation. Dissection started laterally from the hepatic flexure, using a Harmonic® scalpel (Ethicon Endo-Surgery, Blue Ash, OH). Once the duodenum was completely freed, up to the third portion, a gauze was left as a landmark for the medial dissection. Medial dissection started after the exposure of the ileocolic pedicle. The patient was placed in a 10–20° Trendelenburg position. A complete lymphoadenectomy of the ileocolic, right colic (when present), and right branch of the middle colic pedicle was performed. After mesotransverse and mesentery dissection, the ileum and the proximal transverse colon were resected intracorporeally using an endoscopic 45-mm linear stapler with a blue and green cartridge, respectively. The specimen was then extracted by a subcostal incision, protected by a wall protector, and a manual, isoperistaltic, side-to-side anastomosis was performed extracorporeally, with a double layer of continuous absorbable suture (polyglactin 3-0). Mechanical sutures of the ileum and colon stump were previously oversewn by an interrupted suture. No suture of the mesenteric defect was performed. A drain was placed in the right flank, in accordance with our policy for all abdominal major procedures.
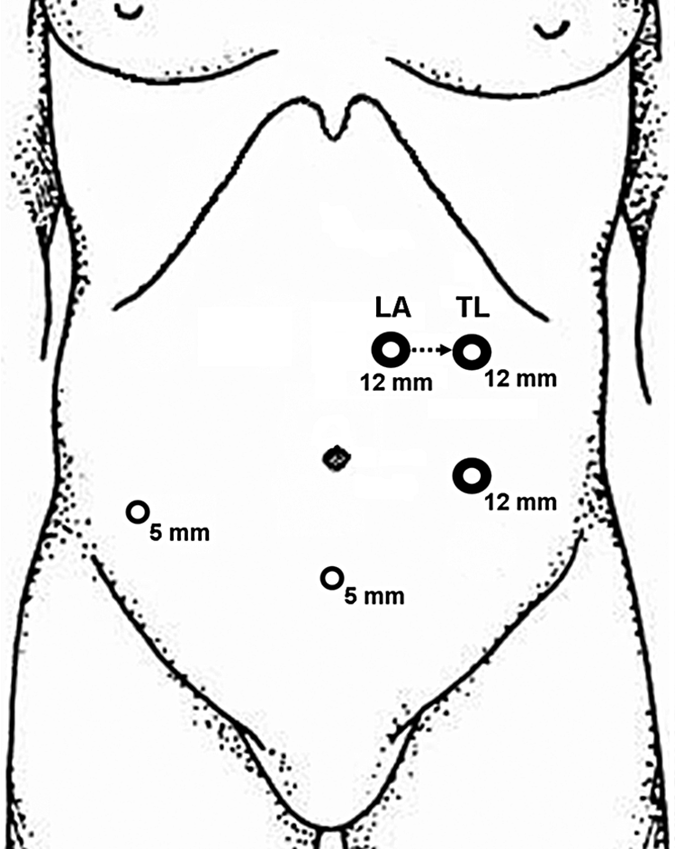
Trocar positions. The position of the upper left 12-mm trocar varies between the laparo-assisted (LA) and totally laparoscopic (TL) procedures.
TLRC
Patient placement and dissection technique did not differ from those of the LA procedure. The first 12-mm trocar was placed more laterally, 8 cm from the midline (Fig. 2). Colon and ileum dissection was performed using a white and blue cartridge, respectively. The specimen was then placed on the liver surface, and an isoperistaltic mechanical ileotransverse anastomosis was performed. The bowels were approached by two exposure stitches; a 45-mm endoscopic linear stapler with a blue cartridge was then inserted through two small enterotomies. The enterotomy was then closed by a double layer of manual intracorporeal suture using polygalactin 2-0 stitches, the first layer continuous and the second interrupted. Two stitches were normally used to close the mesenteric defect, as it is more easily accessible than in LARC. The specimen was finally extracted by a minimal enlargement of the hypogastric trocar, protected by a wall protector. A drain was finally placed through the right trocar port.
Follow-up and outcomes
The urinary catheter and nasogastric tube were normally removed the day after the procedure.
Intravenous ketoprofen (100-mg vials) was used for postoperative pain control. Hospital discharge was scheduled after full recovery from postoperative ileus, resumption of solid diet, and the achievement of a good level of self-sufficiency.
For each procedure the total operating time and the time taken to perform the anastomosis were recorded; the time taken for the other steps of the procedure (defined as resection time) was obtained by subtracting anastomosis time from total operating time. Total operating time, anastomosis time, and resection time were analyzed to compare the techniques and to evaluate the learning curve.
The number of lymph nodes harvested and the length of minilaparotomy were compared and considered as an additional surgical quality marker.
Analgesic administration (number of vials), time of first flatus, time of first bowel movement, complications, transfusions, and length of hospital stay were considered as outcome criteria.
Serum variations of hemoglobin, nitrogen, albumin, and leukocytes on the second postoperative day were also evaluated to compare the outcomes. The Clavien–Dindo classification 15 was adopted for surgical complications.
Statistics
Statistical analysis was performed using software package SPSS version 18.0 (SPSS Inc., IBM, Armonk, NY). The Kolgomorov–Smirnov, and, when appropriate, t test and analysis of variance were used for preliminary data evaluation of continuous variables. Kaplan–Meier statistics were used to analyze discharge temporal curves; significance value was determined by the Mantel–Cox log-rank test. Dichotomic variable association was studied by determining the significance value of the chi-squared distribution. A difference with P<.05 was considered statistically significant. Graphpad (San Diego, CA) Prism® version 5.0 software was used for graphics.
Results
During the study period 59 patients were referred for laparoscopic right colectomy at our institution. Four patients were excluded from the study: 1 for the presence of massive carcinosis (intraoperatively diagnosed) and 3 (5%) for the conversion to open procedure before the anastomosis was performed. Among the 55 patients finally enrolled, 27 were operated on by a LA approach and 28 by a TL approach (Fig. 1).
No conversion to the open approach was required because of technical problems during the execution of the anastomosis.
Patient demographics, body mass index, and American Society of Anesthesiologists status (Table 1) were not significantly different between the groups.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiologists; BMI, body mass index; Hgb, hemoglobin; LARC, laparo-assisted right colectomy; MALT, mucosa-associated lymphoid tissue; ND, not determined; TLRC, totally laparoscopic right colectomy; WBC, white blood cells.
No significant differences were observed in neoplasm site and pathological features (histology and American Joint Committee on Cancer stage) or in preoperative hemoglobin, nitrogen, albumin, or leukocyte values (Table 1).
Operative data are reported in Table 2. The TL approach required a longer surgical time (205.8 minutes versus 186.8 minutes), although the difference was not significant. As shown in Figure 3, the difference depends on anastomosis time (55.6 minutes versus 20.6 minutes, P<.0001). Figure 4 shows operating time variations throughout the series: anastomosis time reduction is fast, whereas a continuous, slow reduction in resection time is reported during the entire series period (LA before and TL after). As a result of that, if we analyze separately the last 10 TLRCs, after a minimal learning curve period, the resultant total operating time was even shorter than for LA (161 minutes versus 186.8 minutes).
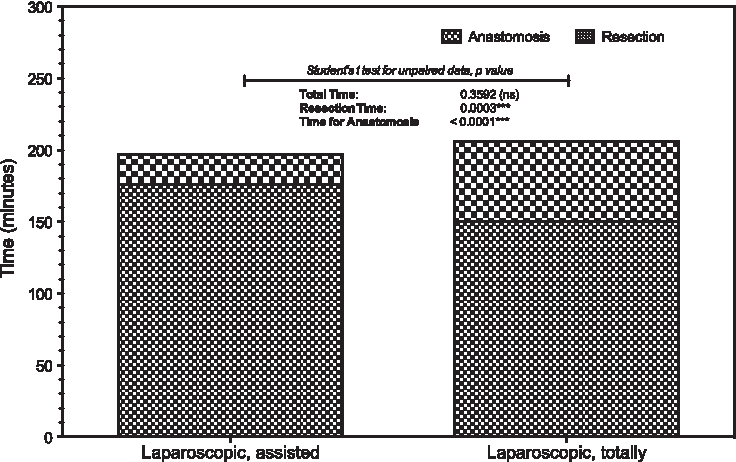
Operating times.
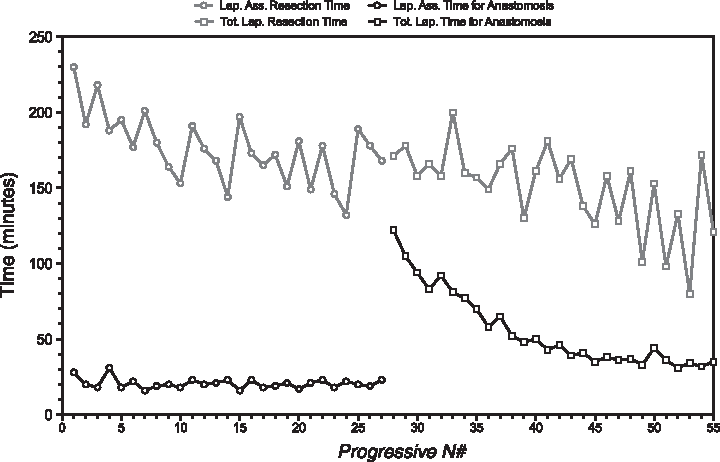
Operating time variations within the series. Lap. Ass., laparo-assisted; Tot. Lap., totally laparoscopic.
Hgb, hemoglobin; LARC, laparo-assisted right colectomy; TLRC, totally laparoscopic right colectomy.
The TL approach allowed for a greater lymph node harvest (20.9 vs. 17.3), albeit not significantly different (P=.176), and a smaller incision length (4.8 cm versus 7.2 cm, P=.002).
No intraoperative or postoperative mortality was observed in the study groups.
Complications are reported in Table 3. One patient in each group was subjected to surgical revision, for a protracted ileus and fever (nothing was found at laparoscopic exploration) and for a duodenal perforation, respectively. No statistically significant difference was found in complication rate (10.7% for TL group and 18.5% for LA group, P=.412) or after Clavien–Dindo stratification. 15
LARC, laparo-assisted right colectomy; TLRC, totally laparoscopic right colectomy).
Patients subjected to the TL approach presented an earlier recovery of flatus and bowel movements (Table 2), although the difference was not significant.
No significant difference was recorded between the groups in terms of postoperative pain, analgesic use, fever, blood transfusions (Table 2), or laboratory values. Mean hospital stay was not significantly different (8.36 days for TL versus 9.26 days for LA); however, the TL group showed a significantly (by Mantel–Cox log-rank test) shorter temporal curve (Fig. 5).
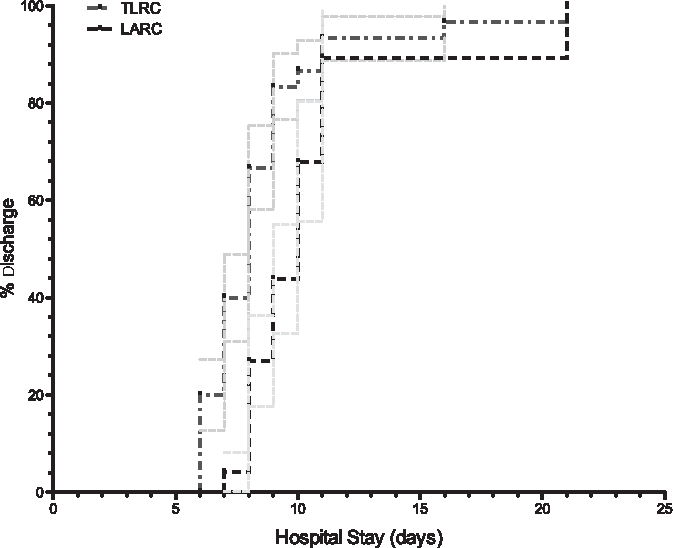
Hospital stay temporal curve. LARC, laparo-assisted right colectomy; TLRC, totally laparoscopic right colectomy.
Statistical analysis did not reveal any correlation between preoperative parameters and hospital stay, with surgical technique being the only variable correlated (P=.0037). Correlation with American Society of Anesthesiologists score showed a tendency to statistical significance (P=.068).
Discussion
Right colonic resection undoubtedly represents a separate chapter of colonic cancer surgery. The reasons for such a peculiarity are mainly technical, related to anatomical differences, and are even more evident if we consider the laparoscopic approach. It is therefore somewhat surprising that the main trials comparing open and laparoscopic colonic resections2–4 did not distinguish between right and left hemicolectomies. Short-term benefits of the laparoscopic approach 5 are indeed much clearer for left colectomies than for right colectomies, as is deducible from the few studies on the matter8,9 as well as from common surgical practice. There are two main anatomical features that make laparoscopy more advantageous for left colectomies than for right colectomies: a wider dissection field, with the chance to spare the longer laparotomy of the open approach, and an endoscopic access to perform the anastomosis (transanal), avoiding the need for the wider access of laparoscopic right colectomies.
In fact, the above reasons have contributed to initially confining minimally invasive right colectomy to a “shadow area”: the strong empirical rather than scientific 9 evidence of a poor clinical and even cosmetic advantage for the laparoscopic approach, performed as an LA procedure, prompted most surgeons performing laparoscopic left colectomies to prefer an open approach for right colectomies. With the development of the TL approach during the last few years, any resistance or doubt seems to have rapidly disappeared, and the minimally invasive right colectomy has regained its role and uniqueness in the field of colonic surgery. However, as in the recent case of single-port techniques, the rapid spread of any technique imposes serious reflection on the underlying reasons for its popularity, in order to prevent dangerous consequences and ambiguities.
In fact, we are facing empirical evidence that TLRC could yield some advantages over a LA approach: a cosmetic benefit, because a shorter laparotomy in a more “aesthetic” site is required, a potentially more precise visceral alignment and mesenteric defect suture, possibly resulting in a lower risk of anastomotic twisting or internal hernias, and a global reduction in visceral pulling and manipulation, possibly resulting in a faster postoperative recovery. Indeed, the only theoretical disadvantage of a TL approach is the technical skill needed for an intracorporeal suture, with the localizing problem for small lesions being easily overcome by a preoperative endoscopic tattooing.
However, what seems evident to us is still not evident when we look at patient outcome. Our work, like that of many others,10–13 failed to demonstrate an overall, statistically significant advantage concerning postoperative recovery for intracorporeal anastomosis. An earlier, nonsignificant recovery of flatus and bowel movement, as reported by other authors,11–14 does not in itself constitute a sufficient parameter of preference, while a tendency to a shorter hospital stay could surely be biased by a policy that is not rendered completely objective. On the other hand, a single case of anastomotic bleeding in the TLRC group could prompt us to consider the mechanical anastomosis as being less hemostatic than the manual procedure, even though the rarity of such a complication and its mild severity (no transfusion required) do not allow for drawing definite conclusions.
Up to now, the article by Fabozzi et al. 14 is the only one that appears to attest to a significant advantage for intracorporeal reconstruction; however, the peculiar biometrical patient characteristics (mean body mass index, 21.49 kg/m2) and surgical skill (mean surgical time, 78 minutes) surely render the series hardly reproducible. It is predictable that we would need very large trials to attest to a significant short-term recovery benefit for TLRC compared with the LA approach or even compared with the open approach, unless we strictly focused on some particular subpopulation (e.g., obese patients). 10
On the other hand, as our study also shows, TLRC surely entails a cosmetic advantage, being equally as safe as the LA and open procedures: in our opinion this is a sufficient reason to prefer it, albeit probably not the main reason for its recent popularity.
Intracorporeal suturing techniques are nowadays an important prerequisite for laparoscopic surgical skill. The ileotransverse anastomosis surely represents an optimal “training field” on account of its anatomical features (wide viscera) and topography (middle abdomen). Our data show (Fig. 4) that for an experienced laparoscopic surgeon the learning curve for an ileotransverse intracorporeal anastomosis is short and that it can be performed safely even during the first procedures. For many surgeons, to perform an intracorporeal ileotransverse anastomosis could represent the first step toward more complicated reconstructive laparoscopic procedures, whereas for others it simply constitutes a satisfactory surgical achievement.
We are therefore convinced that TLRC could reasonably represent a safe compromise between patients' and surgeons' expectations.
Footnotes
Disclosure Statement
No competing financial interests exist.