
Abstract
Abstract
Background:
Robotic surgery was invented to overcome difficulties associated with conventional laparoscopic surgery. However, ways in which to improve the efficacy of such surgery have not yet been discussed. This report focuses on the role of a robotic third arm in maximizing the efficacy of lymph node dissection in robot-assisted gastrectomy.
Materials and Methods:
Thirty-five robotic gastrectomies were performed between April 2009 and December 2010. We evaluated our surgical procedures by reviewing video recordings of robotic operations and analyzed the steps involved in lymph node dissections frame by frame. Then, we analyzed the short-term clinical outcomes to look at the impact of standardized use of the third arm on clinical outcomes. The initial 15 cases (Group A) were compared with 20 later cases (Group B) in terms of postoperative inflammation and pancreatitis.
Results:
The clinicopathologic characteristics, including operation type, hospital stay, morbidity, and pathological features, were not different between the two groups. However, postoperative serum amylase levels as well as drain amylase levels were significantly lower in Group B than in Group A (P<.05). The incidence of postoperative pancreatic fistula was also lower in Group B (P<.05).
Conclusions:
Gastrectomy with extragastric lymph node dissection using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) can be performed safely and effectively with the appropriate and sophisticated use of a robotic third arm.
Introduction
Although patients benefit from laparoscopic surgery, this procedure is more stressful for operating surgeons than conventional open surgery. In an effort to overcome the disadvantages of laparoscopic surgery, the robotic surgery system was introduced as an innovative procedure.7,8 Because of its merits, such as acquisition of a three-dimensional surgical field and overcoming the tremulous handling of tools, robot-assisted surgery has been adopted in various fields of minimally invasive surgery; in particular, it is advantageous for complex procedures, such as prostate cancer and mitral valve replacement surgery.9,10
However, there has been a debate over the merits of robot-assisted gastrectomy (RAG) in gastric cancer patients. In particular, with the expenses of robotic surgery being triple the cost or more compared with laparoscopic surgery in gastric cancer patients, there is controversy over whether RAG provides outstanding benefits or technical merits over the laparoscopic gastrecotmy or not. But, considering that laparoscopy-assisted gastrectomy with lymphadenectomy is regarded as one of the most challenging procedures among gastrointestinal operations, many laparoscopic experts concurred that the robot surgical system has merits in performing delicate procedures such as lymph node dissection. Also, to maximize the efficacy of the RAG procedures, it is critical to use the third arm properly.
In the present study, we proposed the stepwise approach to dissection of radical lymph nodes in robotic gastrectomies and showed the impact of standardization on short-term clinical outcomes.
Materials and Methods
We have performed gastrectomy using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) since April 2009. Since then, a prospectively designed database has tracked all da Vinci Surgical System RAG with lymphadenectomy for gastric cancer. The 35 consecutive patients who were clinically diagnosed between April 2009 and December 2010 with gastric cancer underwent RAG. At least D1+β lymph node dissection was applied to early gastric cancer patients, and D2 lymph node dissection was done for advanced gastric cancer patients based on preoperative stage. We reviewed robotic gastrectomy procedures and analyzed the steps of lymph node dissections to focus on the role of a robotic third arm.
The following parameters were recorded prospectively: age, gender, body mass index, docking times, operative time, estimated blood loss, postoperative hospital stay, postoperative complications, and serum white blood cell counts, C-reactive protein level, and serum or drain amylase activity. The patient cohort was divided into two groups as follows: the first 15 cases (Group A) and the later 20 cases (Group B).
Robot surgical technique
Surgeon background
All the operations in the current study were performed by one surgeon (K.Y.S.), who had performed more than 350 laparoscopic gastrectomies and 35 RAGs with radical lymphadenectomy.
Trocar insertion
After induction of general anesthesia, the patient was placed supine. The camera port was inserted below the umbilicus with a 12-mm trocar, using the open technique. After pneumoperitoneum was established with an intra-abdominal pressure of 12 mm Hg, four ports (one 12 mm and three 8 mm in diameter) were placed under camera visualization. The 12-mm trocar was for the assistant, and the others were for the robot arms. An assistant port was used for introducing surgical gauze and an endo-linear stapler during the procedures. The required length of each trocar was at least 5 or 6 cm, and the robot arm motion functioned easily at 7 or 8 cm. 11 Before the robot was docked, the left lobe of the liver was pierced with a Prolene® (Ethicon, Somerville, NJ) 2-0 straight needle and pulled up toward the abdominal wall to expose the hepatoduodenal area and the lesser curvature of the stomach effectively and to maximize the visual field during the operation. 5
Robot docking
It is important that the central axis of the robot must be in line with the head-to-leg axis of the patient. When the docking process was completed properly, each robot arm must be paralleled with the patient's head-to-leg axis and facing its number front. Because the operating table cannot be changed once the robot has been docked, the height and slope of the operating table must be reconfirmed before the robot is docked. The two 8-mm ports in the right side of the patient were used for the Cadiere forceps and an ultrasonic shear, and one in the left side of the patient was used for a bipolar Maryland forceps (Fig. 1). A general view of the patient's position and the port sites is shown in Figure 2.
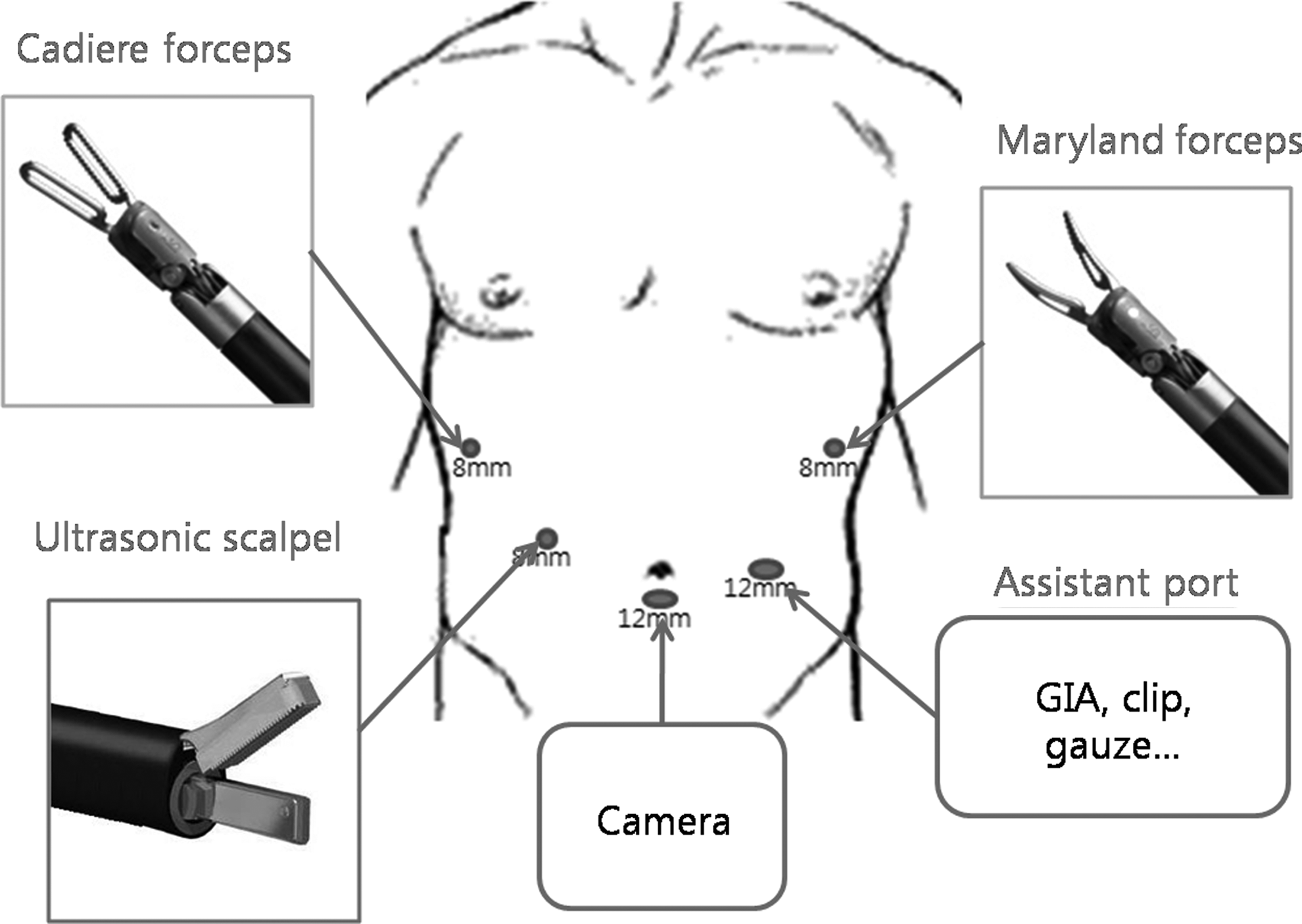
Each trocar's location and main device selection for trocars.
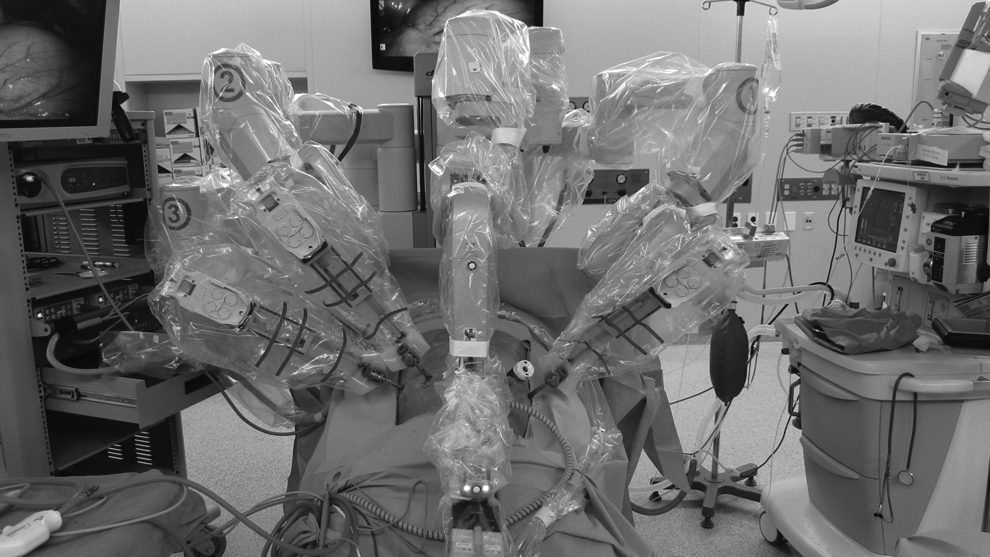
The robotic arm's positions after docking the da Vinci Surgical System for a robot-assisted gastrectomy.
Surgical procedures in general
The procedure itself is similar to the conventional laparoscopic procedures described earlier. 5 The greater omentum was first divided and dissected using ultrasonic shears toward the lower pole of the spleen. Division was then continued all the way to the short gastric vessels to dissect the left gastroepiploic vessels at their roots. The division of the gastrocolic ligament was then continued distally toward the pylorus, and the right gastroepiploic vessels were divided at their roots. Soft tissues attached to the duodenum were dissected. The lesser omentum was then opened, and the duodenum was transected 1 or 2 cm distal to the pylorus using an endoscopic stapling device by the assistant. After the duodenal stump was made by stapling, the lesser omentum was divided all the way up to the right side of the esophageal hiatus. The right gastric artery was exposed and divided at its origin, and then the soft tissues around the proper hepatic artery and medial side of the portal vein area were dissected. The left gastric vein was exposed and divided at the upper margin of the common hepatic artery or pancreas during dissection of lymph nodes bearing soft tissues (lymph node 8a) around the common hepatic artery. The left gastric artery was exposed and divided at its origin by lifting lymph nodes bearing soft tissues (lymph nodes 7 and 9) around the celiac trunks with the Cadiere forceps. Then the upper border of the pancreas was compressed by the Cadiere forceps, using the Maryland forceps and ultrasonic shears. The lymph nodes bearing soft tissues around the proximal and distal splenic vein (11p and 11d) were dissected. The retroperitoneal attachment of the stomach was detached up to the right diaphragmatic crus. Perigastric lymph nodes were dissected along the lesser curvature up to the esophagocardial junction. After full mobilization of the stomach, undocking of the robotic arms from the patient was done.
Remaining procedures, such as (a) removal of the specimen through the infraumbilical 3-cm incision and (b) gastrointestinal anasotomosis and reinforcement sutures over the endoscopic stapler line, were performed totally laparoscopically.
Recommendation for the role of a robotic third arm
Step I was the approach to the common hepatic artery and portal vein (Fig. 3A):

A. Used as a third arm in this view, the Cadiere forceps grasped the soft tissues around the hepatic artery and constantly maintained traction toward the right side of the patients.
B. Using the Maryland forceps, the operating surgeon held medially located soft tissues of the portal vein and used the forceps for maintaining the dissection plane, and a Harmonic® scalpel (Ethicon) was used in the approach to dissect lymph nodes around the common hepatic artery (lymph node 8a) and celiac artery (lymph node 9).
Step II is the approach to the root of the left gastric artery (Fig. 3B):
A. As a third arm, the Cadiere forceps was used for holding soft tissues around the left gastric artery upwardly. B. The operating surgeon controlled the Maryland forceps and Harmonic scalpel at the same time, and by this control, the effectiveness and efficacy of the procedure could be enhanced. C. In this manner, the operating surgeon could gain total control of the operating field.
Step III is the approach to the proximal and distal splenic arteries (Fig. 3C):
A. As a third arm, the Cadiere forceps was used to constantly compress the upper border of the pancreas. B. The operating surgeon held soft tissues around the proximal splenic artery with the Maryland forceps and, at the same time, dissected the lymph nodes (11p or 11d) along the splenic artery with the Harmonic scalpel. C. With constant compression of the third arm in this view, the operating surgeon could minimize the damage to the pancreas and acquire an effective field of operation.
Definition of pancreatic fistula
The serum or drain amylase level was checked on postoperative Day 3 and rechecked later if suspicious for pancreatic fistula. Postoperative pancreatic fistula was defined according to the definition of the International Study Group on Pancreatic Fistula: output, via an operatively implanted drain, of any measurable volume of drain fluid on or after postoperative Day 3, with an amylase content greater than three times the upper normal serum value. 12 In the case of patients who had no drain or whose drain was removed before postoperative Day 3, fever (>38°C), leukocytosis, or peripancreatic fluid detected by computed tomography or ultrasonography was diagnostic of postoperative pancreatic fistula. The postoperative pancreatic fistula grading system used was as follows: grade A, “transient fistula” with no significant impact on postoperative course; grade B, change in management or clinical pathway required; or grade C, significant change in management or clinical pathway required, even aggressive intervention considered. In this study, grade B or C was regarded as significant.
Statistical analysis
All data are expressed as mean with range. The parameters related to operative outcomes and complications between the groups were analyzed using Student's t test or the Mann–Whitney U test, and P<.05 was considered significant. Statistical analyses were performed using SPSS version 13.0 software (SPSS, Inc., Chicago, IL).
Results
No patient was converted to open or laparoscopic surgery. The mean operation time was 260.5±24.5 minutes for total gastrectomy and 217.3±35.6 minutes for subtotal gastrectomy, including 13.8±4.5 minutes for docking time of the da Vinci Surgical System. Most of the patients were discharged from the hospital within 7 days without any postoperative complications. Only 1 patient had to be admitted for 20 days because of anastomosis site leakage after robot-assisted total gastrectomy, and this subject recovered after conservative management with endoscopic stent insertion (Table 1).
BMI, body mass index; F, female; M, male.
The clinicopathologic characteristics, including operation type, hospital stay, morbidity, or pathological features, were not different between the two groups. However, postoperative serum amylase levels as well as drain amylase levels were significantly lower in Group B than in Group A (P<.05) (Fig. 4). The incidence of postoperative pancreatic fistula was also lower in Group B (P<.05) (Table 2).

Postoperative amylase changes. D-amy1 and D-amy3, drain amylase on postoperative Day 1 and Day 3, respectively; S-amy1 and S-amy3, serum amylase on postoperative Day 1 and Day 3, respectively.
Group A consisted of the first 15 patients, whereas Group B consisted of the later 20 patients.
CRP1 and CRP3, C-reactive protein on postoperative Day 1 and Day 3, respectively; D-amy1 and D-amy3, drain amylase on postoperative Day 1 and Day 3, respectively; POPF, postoperative pancreatic fistula; S-amy1 and S-amy3, serum amylase on postoperative Day 1 and Day 3, respectively; WBC1 and WBC3, white blood cell count on postoperative Day 1 and Day 3, respectively.
Discussion
With the advent and steady refinement of new technologies, there has been much development in the field of various cancer surgeries. Minimally invasive surgery, such as laparoscopic and robotic, has become popular. Laparoscopic gastrectomy has been adopted as a routine surgical procedure to date, especially in Korea and Japan. 5 The robotic da Vinci Surgical System has been developed a step further toward overcoming drawbacks of the laparoscopic procedures. However, there are only a few reports regarding the technical feasibility of robotic gastrectomy compared with conventional laparoscopic or open gastrectomies.13–15 Song et al. 13 reported that RAG could be adopted easily by experienced laparoscopic surgeons. The rapid adaptation for robotic-assisted surgical procedures has been suggested in many fields of surgery.16,17 It has been thought that the merits of the da Vinci Surgical System, such as 360° degrees of freedom, three-dimensional views, and tremor filtering of the scope, offer improved dexterity of the surgical procedures and adaptability of the operating surgeons.
However, the delicacy of the robotic gastrectomy is not fully represented by comparing general operative parameters, such as operation time and estimated blood loss. Also, reports on the role of a third arm in robotic gastrectomy are rare. Herein, we first described the procedures in general and then defined the role of the third arm by pointing out the critical steps of gastrectomy. We tried to make stepwise comparisons in critical steps of extragastric lymph node dissections in robotic and laparoscopic gastrectomies. If the robotic third arm was inappropriately positioned, then it could not only conflict with the other active arms, but also be useless during the procedures. This may be the reason why in the early stage, most robotic gastrectomy was performed as a so-called “hybrid of robotic gastrectomy,” which was partly dependent on the surgical assistant during the procedures. Many laparoscopic experts have agreed that the effective control of a robotic third arm is essential to maximize the efficacy of robotic gastrectomy.
In laparoscopic gastrectomy, the operating surgeon could not expect consistent and effective function of an assistant in the critical steps during the procedures until the assistant has overcome the learning curve, such as countertraction of lymph node-bearing tissues around the common hepatic artery or medial side of the portal vein and gentle and delicate compression of the upper border of the pancreas to expose the splenic artery or vein. In the da Vinci Surgical System, the robot arms are totally under the control of the operating surgeon. We believe this is a true merit of the da Vinci Surgical System because the surgeon doesn't have to be dependent on the assistant and can have his or her own controlled field of operation easily.
In our study, we showed the objective difference of short-term clinical outcomes between the initial cases and later cases. For the first 15 cases, we did not have standardized protocols for using the third arm, which was critical for the successful operation during robotic gastrectomy. After those cases, we developed the way of how to use the third arm during the suprapancreatic lymph node dissection and followed it strictly. Although most of the clinical factors were not statistically different, postoperative pancreatitis or pancreatic fistula was less common in later cases. We believe that this means standardized use of the third arm makes the operation be safe at least in terms of pancreatitis, which is common after gastrectomy.
In conclusion, gastrectomy with extragastric lymph node dissection using the da Vinci Surgical System can be performed safely and effectively by appropriate and sophisticated use of a third arm. In the future, more plausible ways of using the robotic third arm to improve the surgical quality and the effectiveness of the robotic gastrectomy should be discussed.
Footnotes
Disclosure Statement
No competing financial interests exist.