
Abstract
Abstract
Aim:
To evaluate the safety of en bloc stapler ligation of the renal vascular pedicle during laparoscopic radical nephrectomy for renal cell carcinoma.
Subjects and Methods:
Clinical data were collected prospectively from 70 patients who underwent either en bloc stapling of the renal hilum (n=35) (Group A) or the separate ligation method (n=35) (Group B) to treat renal cell carcinoma. To evaluate the incidence of arteriovenous fistula (AVF), blood pressure and heart rate were measured, and abdominal auscultation was performed at 1 month, 3 months, 6 months, and 12 months post-surgery. Abdominal computed tomography was also performed at 6 and 12 months post-surgery. In addition, preoperative characteristics and postoperative outcomes (such as operation time and estimated blood loss [EBL]) were examined.
Results:
Both operation time and EBL were lower for Group A: operative time, Group A versus Group B, 60.26±10.94 minutes versus 67.51±10.49 minutes (P=.007); EBL, Group A versus Group B, 33.53±13.46 mL versus 49.14±32.21 mL (P=.011). No statistically significant differences were noted in either of the postoperative variables (blood pressure and heart rate), and there was no clinical evidence of bruit or AVF at 12 months post-surgery.
Conclusions:
No AVF was observed after en bloc ligation upon clinical follow-up or on radiological evaluation.
Introduction
An alternative method, known as the en bloc stapling technique, involves stapling the artery and vein together; however, this method is also associated with complications such as arteriovenous fistula (AVF). 4 Recently, Schatloff et al. 5 showed that en bloc stapling did not increase the incidence of AVF during laparoscopic nephrectomy. However, to date, no prospective randomized controlled trials examining the incidence of AVF after en bloc stapling during LRN for RCC have been performed. Therefore, the present study compared en bloc stapling of the renal hilum during LRN with a technique that involves dissecting out the artery and vein and ligating them separately. The postoperative stability of the en bloc ligation technique was then examined.
Patients and Methods
Patients and study design
In total, 70 patients who were clinically diagnosed with RCC between May 2008 and September 2010 and who satisfied the inclusion and exclusion criteria were recruited to the study. The study was approved by the local Institutional Review Board.
Patients who (1) were radiologically diagnosed with RCC≤T2N0M0, (2) were able to move around freely and perform activities of daily living, and (3) were willing and able to participate in the study were included. The following patients were excluded: (1) patients who could be treated with nephron-sparing surgery (assessed as “low risk” according to the 2007 European Association of Urology RCC guidelines 6 ), (2) patients assessed as “intermediate risk,” who elected to undergo nephron-sparing surgery, (3) patients who had previously undergone laparotomy, (4) patients with a history of ipsilateral renal surgery, and (5) patients with suspected, or with a history of, perinephric inflammation.
The patients were informed about the advantages and disadvantages of each technique. Informed consent was obtained from each patient, along with an agreement to enter the randomization process. Thus patients who met the inclusion criteria were randomized by simple block randomization and underwent either en bloc ligation (n=35) (Group A) or separate ligation (n=35) (Group B).
Surgical technique
For both groups, laparoscopic nephrectomy was performed by a single surgeon using a transperitoneal approach. En bloc stapling was performed by identifying the renal hilum (with no dissection of the fibrolymphatic tissue). The renal artery and vein were then stapled simultaneously using an endovascular GIA™ stapler (Echelon Flex™ 60 mm, 2.5 load Endocutters; Ethicon Endo-Surgery, Cincinnati, OH). For the control group, the renal artery and vein were dissected, separated, and ligated individually; the renal artery was ligated using clips, and the renal vein was ligated using staples (Fig. 1).

En bloc ligation of the renal artery (a) and vein (v) during laparoscopic radical nephrectomy.
Assessment of efficacy and safety
The primary end point was the occurrence of AVF at 1 year post-surgery. The secondary end points were operative time, estimated blood loss (EBL), and complications.
Patients were screened before enrollment to determine whether they met the inclusion or exclusion criteria. Information regarding past medical history was also collected. A physical examination, routine hematologic examinations, and renal function tests were also performed. Blood pressure and heart rate were measured, and abdominal auscultation was performed at each visit (at the pre-enrollment screening and 1 month, 3 months, 6 months, and 12 months postoperatively) to diagnose AVF. In addition, abdominal computed tomography (CT) was performed at 6 and 12 months postoperatively. Operative time, EBL, pathologic findings, and complications were also documented to compare the surgical outcome between the two groups.
Statistical analysis
Statistical analysis was performed using intent-to-treat analysis. Operative time and EBL during the operation were assessed using Student's t test. In addition, the location of the renal mass, the clinical stage, postoperative pathologic findings, and complications were compared using the chi-squared test. SPSS version 18.0 software (SPSS, Inc., Chicago, IL) was used for all statistical analyses, and a P value of <.05 was considered statistically significant.
Results
One subject from Group A was lost to follow-up and therefore excluded. Data collected from the medical records of the 34 and 35 patients in the en bloc ligation and separate ligation groups, respectively, who completed the study were analyzed (Fig. 2).
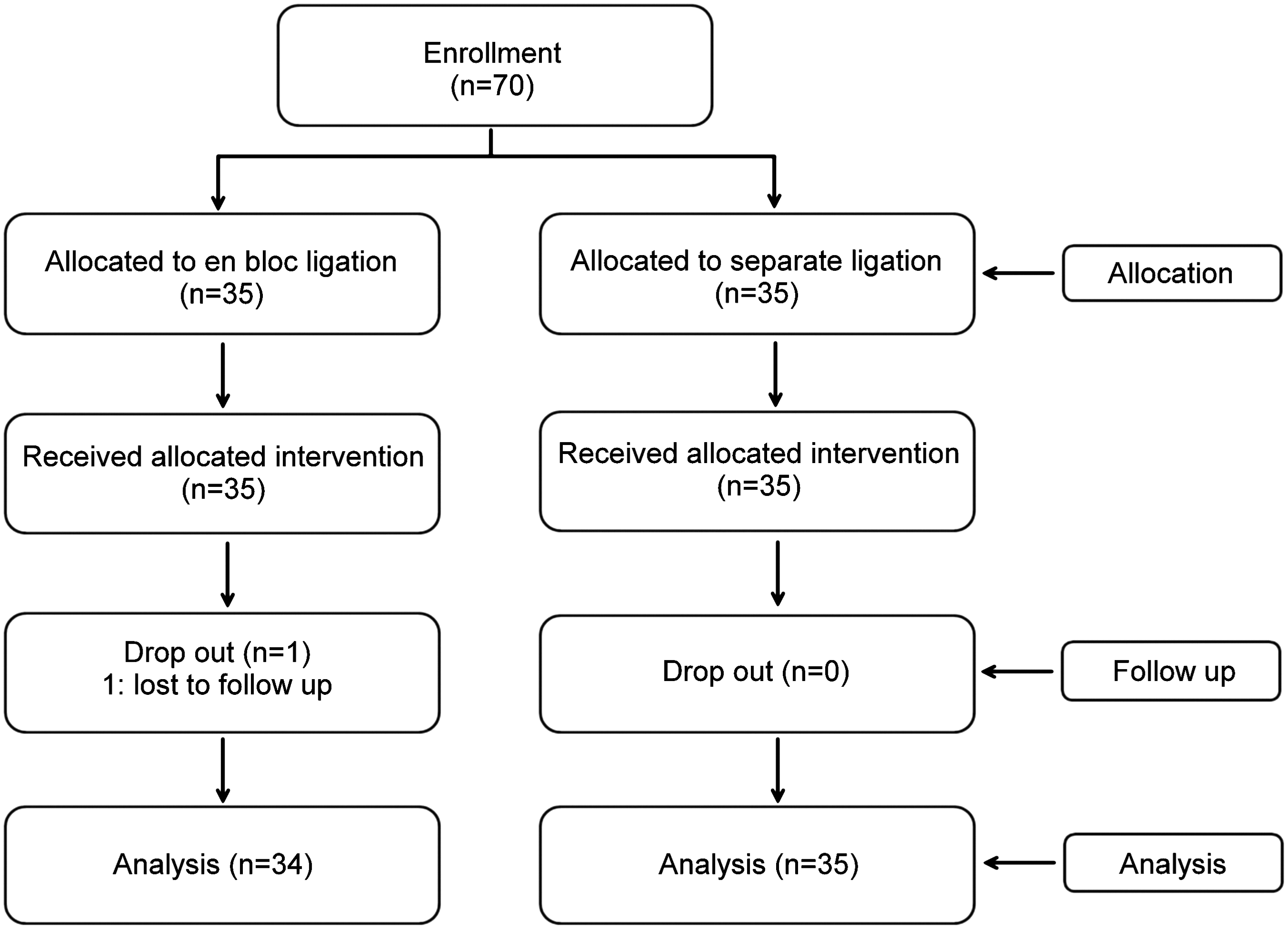
Participation flowchart.
There were no statistically significant differences in preoperative characteristics between the two groups. The size of the renal mass in Group A was 6.24±1.87 cm, and that in Group B was 6.52±1.52 cm (P=.498). There was no significant difference in preoperative clinical stage between the two groups (P=.263) or in the side (left or right) presenting with RCC (P=.536) (Table 1). Two patients in Group B experienced renal vein injury during dissection to separate the artery and vein, and one required conversion to an open procedure. The operation time was 60.26±10.94 minutes for Group A and 67.51±10.49 minutes for Group B (P=.007). EBL was 33.53±13.46 mL for Group A and 49.14±32.21 mL for Group B (P=.011). Upon postoperative histopathologic examination, 32 patients in Group A were diagnosed with RCC, 1 with cystic nephroma, and 1 with oncocytoma. In Group B, 33 patients were diagnosed with RCC, 1 with angiomyolipoma, and 1 with oncocytoma. Three patients in Group A and 2 patients in Group B required a blood transfusion on post-surgical Day 1 (Table 2). No patient was diagnosed with AVF upon abdominal CT performed at 6 and 12 months postoperatively (Fig. 3). In addition, no bruit was heard on abdominal auscultation, and there were no significant differences in blood pressure or heart between the two groups. There was no evidence of AVF in either group at 1, 3, 6, or 12 months postoperatively (Table 3).
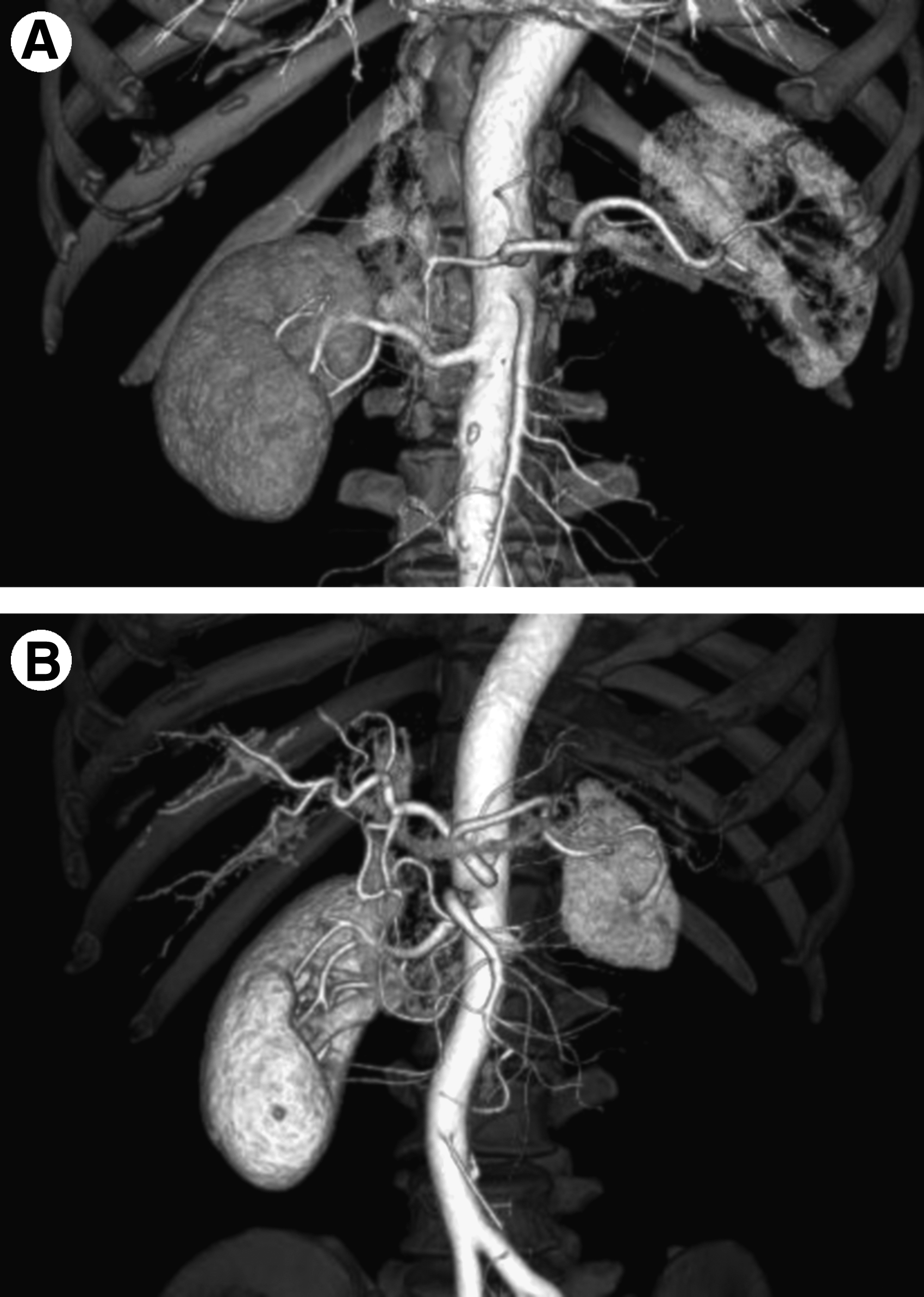
Reconstructed computerized tomographic arteriographs obtained post-surgery:
Group A received en bloc ligation; Group B underwent the separate method.
P values were calculated by Student's t-test unless designated otherwise.
By chi-squared test.
BMI, body mass index.
Group A received en bloc ligation; Group B underwent the separate method.
P values were calculated by Mann–Whitney test unless designated otherwise.
By chi-squared test.
AML, angiomyolipoma; AVF, arteriovenous fistula.
Group A received en bloc ligation; Group B underwent the separate method.
P values were calculated by Student's t-test unless designated otherwise.
Discussion
En bloc ligation of the renal hilum during laparoscopic nephrectomy did not carry a higher risk of complications than separate ligation. In addition, the operating time was shorter than that for the separate ligation method.
Post-nephrectomy AVF is a rare complication. According to a literature review by Lacombe, 7 approximately 60 cases were reported in 40 years (from 1934); however, en bloc stapling appeared to increase the risk of AVF. AVF results in increased venous congestion and can cause tachycardia or rapid cardiopulmonary decompensation. It may even cause severe cardiac failure and death. 8 Thus en bloc stapling of the renal hilum during nephrectomy has been avoided.
However, Baptista-Silva et al. 9 showed that inflammation and remnant tumor fragments increased the risk of post-nephrectomy AVF. The studies showing that en bloc stapling increases the incidence of AVF all included patients undergoing nephrectomy due to infection and trauma; this may have affected the outcomes, leading to the erroneous suggestion that en bloc stapling increases the risk of AVF. 10 When en bloc stapling is performed, the presence of inflammation (caused by infection or trauma) or the suture material (which acts as a foreign body and can cause tissue erosion) can increase the risk of AVF. 11 The present study excluded patients with evidence of perinephric inflammation or untreated pyuria on preoperative CT scans and urine analysis to avoid inflammation-induced AVF.
Other reports have retrospectively evaluated patients who underwent en bloc stapling during nephrectomy and found no evidence of AVF (Table 4). These studies were performed exclusively in patients with RCC, but included those undergoing nephroureterectomy to treat urothelial cell carcinoma and those undergoing simple nephrectomy to remove a benign mass or a nonfunctional kidney. The present study is the first randomized controlled trial of the en bloc stapling method for LRN in patients with RCC. Similar to previous studies, the present study found no evidence of AVF on CT scans performed 6 months and 12 months postoperatively or on careful abdominal auscultation and observation of vital signs at each follow-up visit.
AVF, arteriovenous fistula; EBL, estimated blood loss; HALS, hand-assisted laparoscopic surgery; NR, not reported.
The removal of the renal hilum during laparoscopic nephrectomy is very difficult because it contains major blood vessels such as the renal artery and vein and the vena cava, which are surrounded by fibrolymphatic tissue. In addition, laparoscopic surgery carries the risk of massive bleeding due to damage caused to the major vessels, which may then require conversion to an open procedure. On the other hand, en bloc stapling does not involve as much hilar dissection as other methods that involve ligating the renal artery and vein separately. In the present study, renal vein injury occurred in 2 patients in the control group, one of whom required conversion to an open procedure. Also, blunt dissection was used to separate the perihilar tissues, and, unlike the separate ligation method, no dissection was performed inside the renal hilum. Significant differences in EBL (due to bleeding resulting from the dissection process or by injury to the major vessels) were observed between the two groups. Stapling is one of the safest ways to ligate blood vessels, and the failure rate is less than 0.5% (if cases of inappropriate use are excluded). 12 To ensure appropriate stapling, the instrument must be in good condition before the procedure. The surgeon should also confirm the absence of solid material (such as clips) from the tissues. In addition, there must be plenty of space between the great vessels and the kidney. All of the tissues to be stapled must be positioned correctly between both jaws. If device failure occurs, then clips and an endosuction device are placed into the peritoneal cavity; the jammed staple should then be released using the emergent release button. Additional clips should be used at incompletely ligated sites. However, clipping of the renal artery requires sufficient dissection and much caution because there is a risk of vessel injury should the clip slip. 3
Using a stapler during radical nephrectomy is more expansive than using Hem-o-lok® (Weck Surgical Instruments, Teleflex Medical, Durham, NC) clips or other clips. However, we found that en bloc stapling resulted in shorter operation times and a lower risk of bleeding, which may reduce the overall cost of the procedure. Thus, en bloc stapling may be an appropriate alternative to separation ligation.
The present study has several limitations. The follow-up period was relatively short, and the sample number was small. In addition, ligation of the renal artery and vein using a stapler would be a more suitable design for the control group. Despite these limitations, this is the first randomized controlled study conducted to evaluate the safety of en bloc stapling of the renal hilum during LRN and to examine its effects on the incidence of AVF. Further long-term follow-up studies involving a larger sample number are required to confirm these results.
Conclusions
En bloc stapler ligation of the renal vascular pedicle during LRN for RCC appears to be safe, and the results are comparable with those obtained when the vessels are ligated separately.
Footnotes
Acknowledgment
This study was supported by Dong-A University Academic Fund.
Disclosure Statement
No competing financial interests exist.