
Abstract
Abstract
Background and Study Aims:
The study of lymph as a biofluid is lacking because of absence of a safe site and technique for lymph acquisition. Injury to the thoracic duct during surgery is known to cause chylothorax. The aim of this interventional study was to puncture the thoracic duct under endoscopic ultrasound (EUS) guidance and observe for complications in a swine model.
Subjects and Methods:
Three female Yorkshire pigs underwent EUS. The thoracic duct was identified by the previously described technique, punctured, and confirmed with a lymphangiogram. Postoperatively, animals were fed and monitored closely for any complications or signs of abnormal behavior indicating pain and/or disease. The animals were euthanized at 1 week, and necropsy was performed per protocol. Main outcome measurements included complications (chylothorax, mediastinitis, perforation, and hemorrhage) during the post–EUS-guided thoracic duct puncture period.
Results:
No animals developed any complications during the survival period. The thoracic duct was identified and punctured in all animals. A lymphangiogram was additionally obtained to confirm ductal access. No chylothorax, mediastinitis, hematoma, abscess, or fistula formation was identified in any animal on necropsy.
Conclusions:
EUS-guided transesophageal thoracic duct puncture is safe as demonstrated by this survival study.
Introduction
The thoracic duct is difficult to access. Access usually is obtained via a “surgical cutdown” in the neck at the left jugulosubclavian angle. 4 Percutaneous transabdominal thoracic duct access has also been described.5,6 However, these techniques are invasive, time consuming, and cumbersome. Therefore, the lack of an easy access technique has limited the study of the lymphatic system. As the thoracic duct transports various cells and cellular components, including cancer cells, the analysis of lymph obtained by thoracic duct puncture may potentially offer clues with regard to the early spread of malignancies. Furthermore, repeated serial sampling of lymph over time may contribute knowledge of the functional, morphologic, and immunologic dynamics of the lymphatic system and various systemic disorders. 7
Recently, progress has been made for a reliable access of the thoracic duct. This began with description and identification of the thoracic duct by endoscopic ultrasound (EUS). 8 The thoracic duct has been punctured under EUS guidance in animals. The feasibility of lymph sampling by EUS-guided puncture of the thoracic duct has been established as a proof of concept. 9 Injury to the thoracic duct during surgery is known to cause chylothorax, but it is not known if EUS-guided puncture of the thoracic duct for lymph sampling would cause complications such as chylothorax, mediastinitis, perforation, and hemorrhage. Animal survival studies are therefore needed to evaluate these potential complications before initiating human trials.
The aims of the present study were to puncture the thoracic duct under EUS guidance, to perform a lymphangiogram to confirm the access, and to observe any complications in a swine model for the study period of 1 week.
Materials and Methods
The study was approved by the Institutional Animal Care and Use Committee of the Uniformed Services University. Research was conducted in compliance with the Animal Welfare Act and other federal statutes and regulations relating to animals and experiments involving animals and adhered to principles stated in the “Guide for the Care and Use of Laboratory Animals.” 10
Three female Yorkshire pigs (median weight, 60 kg) underwent EUS. The pigs were anesthetized by intramuscular injections of ketamine (20 mg/kg), xylazine (3 mg/kg), and glycopyrrolate (0.01 mg/kg). The animals were intubated; anesthesia was maintained with 2% isoflurane and oxygen. Each animal was fed 50 mL of corn oil 3 hours before the study to increase the thoracic ductal inflow. EUS was performed with a linear echoendoscope (model GF-UC 30P; Olympus America Corp., Melville, NY). The thoracic duct was identified by the previously described technique, 8 with the difference that no contrast medium was injected for fluoroscopic localization of thoracic duct and that it was done using EUS alone. A 25-gauge needle (Echotip Cook Medical Inc., Winston Salem, NC) was used to puncture the thoracic duct. Contrast medium (Ethiodol®; Savage Laboratories, Melville) (2–5 mL) was then injected to obtain a lymphangiogram and to confirm the access into the thoracic duct.
After the procedures, the animals were fed and monitored closely for any complications or any signs of abnormal behavior indicating pain and/or disease by a veterinarian. The animals were kept alive for 1 week and then euthanized, and a necropsy was performed per protocol.
Results
The thoracic duct was identified and punctured in all three animals. The aspirated fluid was sent for microbiological analysis of basic characteristics like cell count, lymphocyte count, and protein, to differentiate it from plasma.
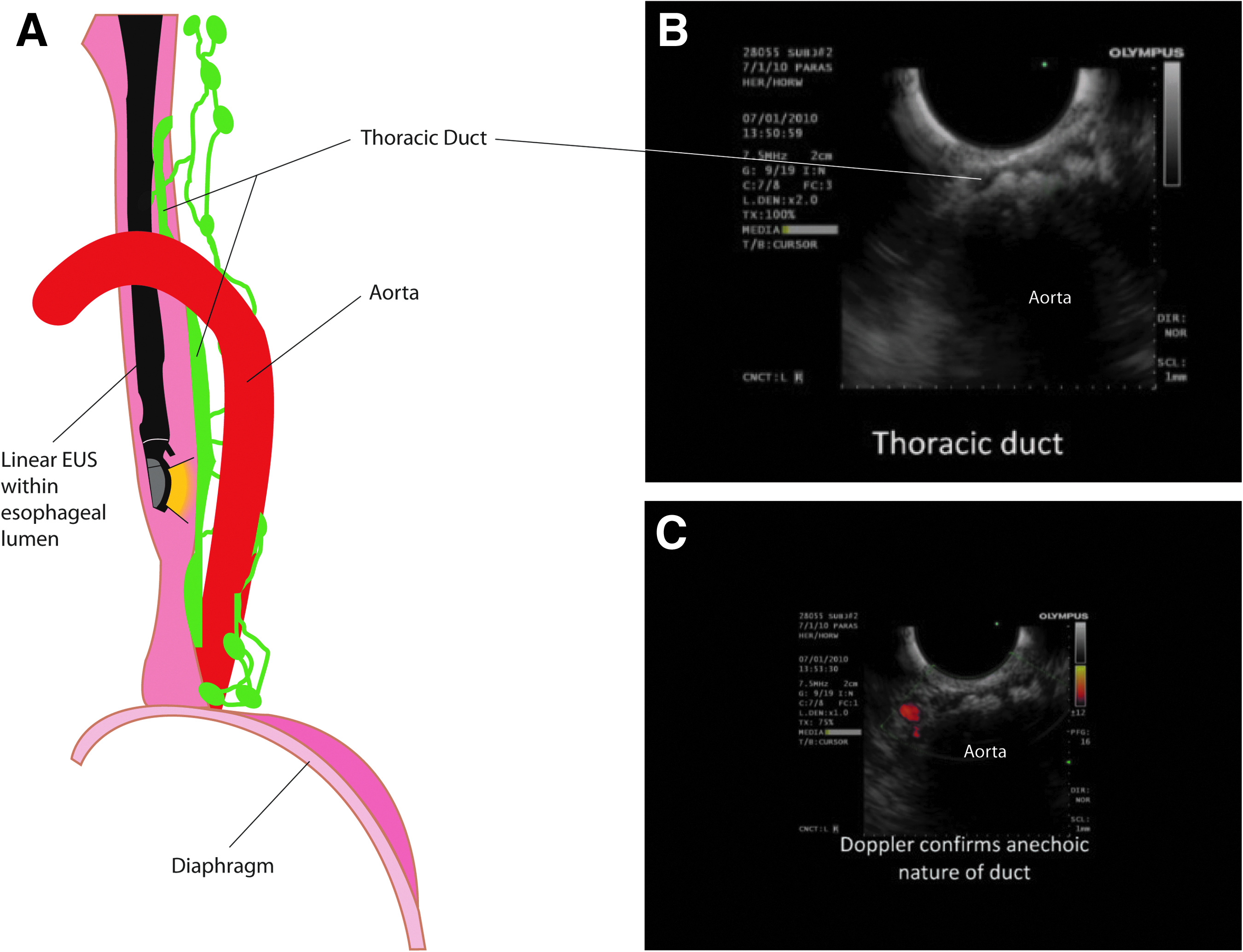
Figure 1A is an anatomic illustration defining the location of the echoendoscope within the esophagus and its position to localize the thoracic duct. Figure 1 also describes the relationship of the thoracic duct to nearby structures as seen by the echoendoscope. Figure 1B depicts the image of localization of thoracic duct by EUS. The thoracic duct was identified by EUS at the level of the 10th thoracic vertebrae as a small, tubular, anechoic structure lying between the aorta and the esophagus that exhibited no evidence of flow by color Doppler ultrasound (Fig. 1C). Puncture of the thoracic duct was confirmed by a lymphangiogram obtained by injecting approximately 2–5 mL of contrast medium.
None of the three animals developed any complications during the survival period. No chylothorax, mediastinitis, hematoma/hemorrhage, perforation, abscess, or fistula formation was identified in any animal during the necropsy.
Discussion
The lymphatic drainage system is a highly complex network of vessels. It is a major route for transport of excess fluid, protein, and waste products from the tissue spaces into the circulatory system. Besides containing protein, lipids, and vitamins, the thoracic duct lymph also carries neoplastic cells, bilirubin, and bacteria.2,3 Access to the thoracic duct can be obtained by surgical cutdown or transabdominal percutaneous puncture.4–6 The thoracic duct has been punctured under EUS guidance in animals, and the viability of lymph sampling has been demonstrated. 6 Theoretically, there is a potential concern about complications arising from puncture of thoracic duct, namely, chylothorax, mediastinitis, perforation, and hemorrhage. Animal survival studies are therefore needed to evaluate these potential complications before initiating human trials.
The present survival study establishes the safety of EUS-guided thoracic duct puncture in a swine model. Our study demonstrates that none of the three animals developed any complications during the 1-week post-procedure period. After the procedure, no animals developed any abnormal behavior indicating pain and/or disease, as monitored closely by a veterinarian. The animals were kept alive for 1 week and then euthanized, and a necropsy was performed per protocol. There was no evidence of chylothorax or other complications on necropsy such as mediastinitis, hemorrhage, and/or perforation. Available literature was reviewed before deciding to observe animals for 1 week for possible complications—this includes all three major complications of thoracic duct injury, namely, chylothorax, chylous fistula, and mediastinitis. We have not come across any significant report of thoracic duct injury and complications beyond 1 week of intervention or any de novo manifestation beyond that period. Most of these complications of thoracic duct injury, in fact, occur intraoperatively and on some occasions were noticed immediately postoperatively. For these reasons, we believe 1 week of follow-up was adequate.
This current study carries forward a concept earlier proposed by our group8,9 but differs from the earlier experiments because of the use of EUS alone (without contrast injections into lymphatic system) to localize the thoracic duct, use of a 25-gauge needle to puncture, and later monitoring animals for complications, in order to establish safety of this procedure. One of the theoretical hurdles in application of this technique in human subjects may be that aspiration of lymph is a very difficult process (in both animals and humans) because of the low basal flow rate of lymph in the thoracic duct (0.93 mL/minute in a human fistula study 11 ). Our group is currently working on this problem and has demonstrated increased thoracic duct diameter from baseline, as well as increased lymph flow through the thoracic duct after intraduodenal instillation of 20% intralipid. 12 This step would make aspiration of lymph easier in human subjects.
Lack of access techniques has contributed to inadequate study of lymph as a biofluid in humans. Once standardized, the EUS-guided thoracic duct puncture and lymph analysis may be helpful in studying the pathophysiology of the lymphatic system in humans. 7 Besides the dynamics of the lymphatic system, EUS-guided access to the thoracic duct may play an important role in studying T-cell lymphopoiesis, 13 immunosuppression by lymphocyte depletion in studies of patients with autoimmune diseases, renal transplant rejection, rheumatoid arthritis, multiple organ dysfunction syndrome, and acute pancreatitis.14–17 Furthermore, sampling of thoracic duct lymph might be used to study cholesterol metabolism absorption and transport, which is quintessential for atherosclerosis and coronary artery disease research. 18 Also, because lymph is composed of various cells and cellular components, including cancer cells,2,3 the analysis of lymph obtained by thoracic duct puncture may potentially offer clues with regard to the early spread of malignancies. EUS-guided thoracic duct puncture and lymph analysis may also allow proteomic profiling of lymph for potential biomarkers for malignancy. 19 Improving access to the thoracic duct may open a new source for emerging molecular studies on EUS–fine needle aspirate material, which in the future may provide diagnostic and prognostic information that is beyond routine conventional cytology. 20
These findings of our survival study indicate that EUS-guided transesophageal thoracic duct puncture is a safe procedure. Further studies that use animal models will be needed to standardize the technique of EUS-guided transesophageal puncture of the thoracic duct.
Footnotes
Acknowledgments
The authors are grateful to the staff of the Surgery Department, Division of Veterinary Medicine, Uniformed Services University, for their expert care of the animals during this study. The authors also wish to thank Sudhir K. Dutta, MD, FACP, MACG, Professor of Medicine, University of Maryland School of Medicine and Director of Division of Gastroenterology, Sinai Hospital of Baltimore, Maryland; and Rayburn F. Rego, MD, Associate Professor of Medicine, Division of Gastroenterology and Hepatology, University of Arkansas for Medical Sciences, Little Rock, Arkansas, for their critical opinions in refining this manuscript.
Author Contributions
M.G. performed analysis and interpretation of data, manuscript preparation, and revisions. J.D.H. performed concept and design and critical revision of manuscript. T.L.S. performed concept and design, supervision of animals during the study, and critical revision of manuscript. V.K.P. performed concept and design and manuscript critical revision, was the procedural gastroenterologist, and gave final approval.
Disclosure Statement
No competing financial interests exist.