
Abstract
Abstract
Background and Purpose:
Since laparoscopic hernia repair was reported a few decades ago, many techniques have been developed. A simplified and safe procedure with a low recurrence rate and good cosmetic result is the main concern. In this study, we introduced a new method, transumbilical two-port laparoscopic percutaneous extraperitoneal closure (TTPLPEC), and evaluated the safety and feasibility of this method.
Patients and Methods:
Five hundred thirty-six patients who accepted the TTPLPEC procedure in our hospital from July 2008 to January 2012 were analyzed retrospectively. During the TTPLPEC procedure, a laparoscope was placed through a supraumbilical incision. A 3-mm grasping forceps was inserted into the peritoneal cavity through a 3-mm infraumbilical incision. Using a hooked needle, the hernia sac was closed extraperitoneally.
Results:
In total, 731 inguinal repairs were performed in 536 children with an age range from 3 months to 14 years. All operations were completed successfully by TTPLPEC. Contralateral patent processus vaginalis was found in 43.0%. For female patients, the mean operation time was 8.3 minutes for the unilateral procedure and 12.8 minutes for the bilateral procedure; for male patients, the mean operation time was 12.5 minutes and 18.6 minutes, respectively. At follow-up, there were two recurrences (0.37%) and 2 missed cases of contralateral patent processus vaginalis that developed a metachronous hernia. No other postoperative complication was noted. Six months after the operation, most patients had no obvious signs of a previous operation.
Conclusions:
The preliminary results showed satisfactory outcomes with TTPLPEC in the treatment of inguinal hernia in children. This technique for inguinal hernia repair in children appears to be safe and feasible, has good cosmetics, and has a low recurrence rate.
Introduction
Traditional laparoscopic inguinal repair operations need one or two working ports. To minimize the invasiveness of the traditional laparoscopic operation and to improve cosmesis, recently, some single-port laparoscopic surgeries have been developed.9–11 But, all these methods had some limitations. To overcome those limitations and preserve the cosmetic aim, we designed a new technique, transumbilical two-port LPEC (TTPLPEC), for treatment of inguinal hernias. This study aimed at evaluation of its technical feasibility, safety, and preliminary results.
Patients and Methods
In this study, we retrospectively analyzed 683 patients who accepted the TTPLPEC procedure in our hospital from July 2008 to January 2012. Diagnosis of an inguinal hernia was confirmed during a preoperative examination. The study included those patients who presented with a previously unrepaired inguinal hernia and returned for follow-up after at least half a year in the outpatient department after surgery. Thirty-nine cases were recurrence hernias, and 108 cases failed to come back for follow-up. Those 147 cases were then excluded from the series. So there were 536 cases that were included in this study. The patients accepted follow-up in the outpatient department by surgeons. Physical examinations were carried out on the patients to record the scar, recurrence, postoperative hydroceles, and testicular atrophy or ascent after operation. Data collection included demographics, laterality at presentation, operative findings, operative time, recurrence rate, and postoperative complications. Consent was obtained from the patients' parents and the ethical committee of the West China Hospital of Sichuan University to use these data in this project.
Surgical Procedure
After general anesthesia, patients were placed in the supine position. The viewing monitor was placed at the patient's feet. The operator stood on the opposite side to the inguinal hernia, and the camera assistant stood on the other side. A 5-mm supraumbilical skin incision was made. A Veress needle was then inserted into the abdomen, and pneumoperitoneum was established at 8–12 mm Hg. A 5-mm trocar was inserted through the supraumbilical incision, and a 4.5-mm 30° laparoscope was placed in position. A 3-mm infraumbilical skin incision was made, and a 3-mm grasping forceps was then introduced into the peritoneal cavity without a trocar (Fig. 1).

The laparoscope was placed through the supraumbilical incision, and a 3-mm grasping forceps was introduced into peritoneal cavity through an infraumbilical incision without a trocar. By this means, the transumbilical two-port laparoscopic percutaneous extraperitoneal closure procedure increased the distance between the laparoscope and the grasping forceps.
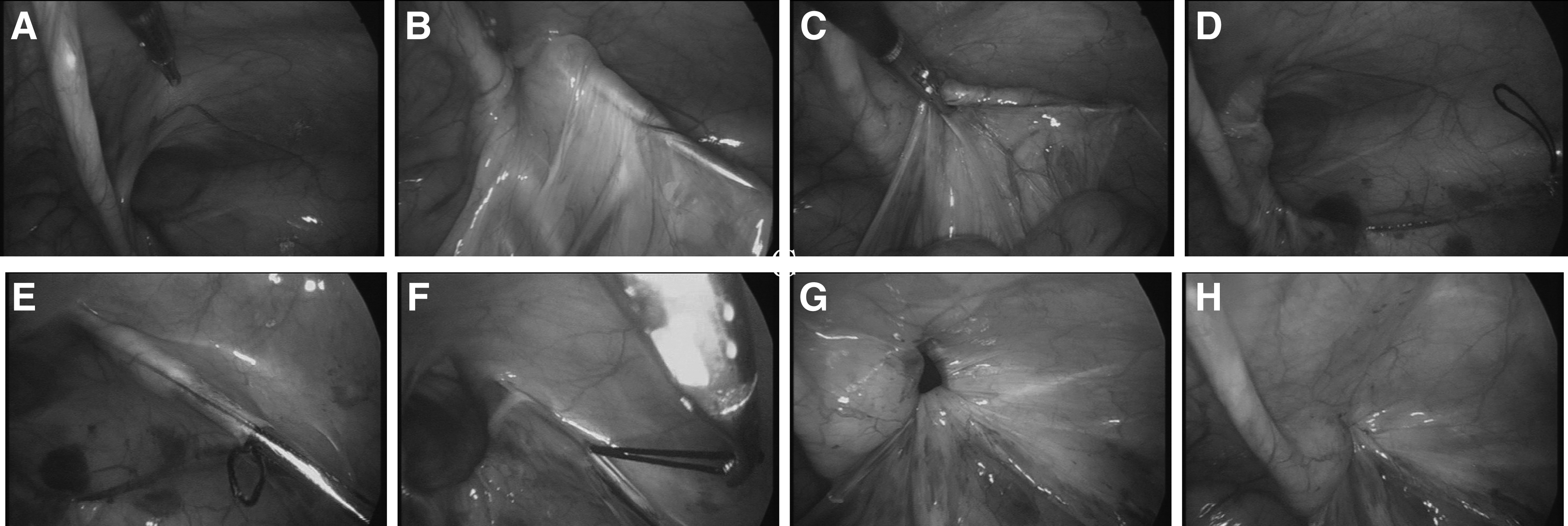
The following procedure was performed using a modified version of the method developed by Takehara et al. 8 A homemade hooked needle with 2-0 or 1-0 nonabsorbable suture material was inserted at the midpoint of the right or left inguinal line. Using the needle and with the aid of the grasper, the orifice of the hernia sac was closed extraperitoneally with circuit-suturing around the internal inguinal ring without any peritoneal gap. Care was taken to cross over the spermatic duct or the gonadal vessels to avoid causing injury (Fig. 2). When an asymptomatic contralateral PPV was observed, bilateral closure was performed. All wounds from the operation were closed with skin adhesive (Fig. 3).

Umbilical incisions and inguinal puncture wounds from the operation were closed with skin adhesive.
Results
From July 2008 to January 2012, 536 patients accepted the TTPLPEC procedure in our hospital. The ages ranged from 3 months to 14 years, with a mean age of 39 months. There were 447 boys and 89 girls, with a male:female ratio of 5:1. There were 454 patients who presented with a unilateral hernia: 337 patients (62.9%) on the right side and 117 patients (21.8%) on the left side. The other 82 patients (15.3%) presented with bilateral hernias. During the operation, among the 454 patients who presented with a unilateral hernia preoperatively, 195 patients (43.0%) were found to have contralateral PPV; thus a bilateral laparoscopic repair was performed during the same procedure. In the total of 536 patients, 731 hernia repairs were done for a primary inguinal hernia. They were all successfully treated by the TTPLPEC procedure, and no cases were converted to the open operation. For female patients, the mean operation time for unilateral cases was 8.3 minutes, and that for bilateral cases was 12.8 minutes; for male patients, the mean operation time was 12.5 minutes and 18.6 minutes, respectively. All patients were discharged on the first postoperative day. All patients accepted follow-up for at least half a year, and the average follow-up period was 20 months (range, 6–36 months). At follow-up, there were 2 patients (0.37%) who developed recurrent hernias. Another 2 patients, who had undergone unilateral laparoscopic hernia repair and were noted to have an obliterated processus vaginalis on the side contralateral to the initial operation, developed a contralateral inguinal hernia at follow-up. The TTPLPEC procedure was then performed on the contralateral side. No postoperative hydroceles, testicular atrophy, or ascent occurred after the operation. At follow-up, most patients had no obvious signs of a previous operation 6 months after operation (Fig. 4).

At follow-up, no visible scar was seen after the operation. The umbilical wound scars were hidden in the fold of the umbilicus, and the puncture wound from the needle was unnoticeable.
Discussion
Laparoscopic inguinal hernia repair has become more and more popular in pediatric surgery for its clear advantage compared with the conventional open operation. Conventionally, the combination of suturing and tying knots intracorporeally to closing the hernia orifice is one of the most popular laparoscopic methods. However, this procedure is not easily performed, and a high recurrence rate was the main concern.4,5 One of the main challenges to prevent recurrence is to obtain a complete circumferential closure of the sac at the level of the internal ring without injury to the adjacent vas deferens or spermatic vessels. Recurrence may be related to the skipped areas during placement of purse-string sutures as well as the tension resulting from intracorporeal knotting, particularly in closure of large defects. LPEC for childhood inguinal hernia was first introduced by Takehara et al. 8 By using this method, ligation of the hernia defect without a peritoneal gap can easily acquired, and the ligature was performed extracorporeally as in the open method. Then this method became popular for its simple procedure, complete enclosure, reliable ligation, and low rate of recurrence and complications. In this study, all patients accepted the LPEC procedure, and the results confirmed the advantages of this method.
Traditional laparoscopic inguinal repair operation, including LPEC procedure, needs one or two working ports. To minimize the invasiveness of traditional laparoscopic operation and to improve cosmesis, some single-port laparoscopic surgeries have recently been developed.9–11 Transumbilical endoscopic surgery is a single-port laparoscopic hernia repair method reported by Zhou et al. 9 In this method two trocars are inserted through the umbilicus incision: one for the laparoscope and the other for needle-holding. Then the hernia opening is sutured by needle-holding under laparoscopy. Like the conventional suturing method, this method also has difficulty in obtaining a complete circumferential closure of the hernia and knot tying intracorporeally. Moreover, using this method, the operation is even more difficult to perform for its single-port procedure and the reduction of the working ports from two to one.
Another single-port operation was reported by Chang et al.11,12 Under laparoscopic guidance, the hernia defect was enclosed by a homemade hook-pin through a needle puncture wound with a nonabsorbable suture, and knot tying was performed extracorporeally. This method is similar to the LPEC procedure. But without a working port, some disadvantages might arise. According to our experience, the working port introducing a grasping forceps is necessary for the laparoscopic hernia repair. On the one hand, the grasping forceps can facilitate the dissection of the spermatic vessels and the vas deferens to secure the enclosing of the hernia defect without a peritoneal gap and to prevent the adjacent vas deferens and spermatic vessels from injury. On the other hand, the grasping forceps can make the detection of the contralateral PPV more precise. It is well known that contralateral PPV detection is one of the most important merits of laparoscopic hernia repair. But sometimes, the hernia orifice is covered by a small peritoneal fold and cannot be noted without a grasping forceps. So the grasping forceps is necessary to lift the peritoneal fold and then to detect whether there is a contralateral PPV precisely (Fig. 5). In this study, there were 195 patients (43.0%) who were found to have contralateral PPV, and the rate was much higher than in other previous studies.13–15 However, there were still 2 patients with missed contralateral PPV during the laparoscopic examination. Some studies also reported false-negative examination.15,16 But, few studies have explained the reason for this phenomenon. In our viewpoint, the concealment of a contralateral PPV might responsible for this false-negative finding. To avoid this result, we suggest that more careful examination with the grasping forceps should be performed to prevent the metachronous hernia in the future.

To overcome these limitations and preserve the cosmetic aim, we designed the TTPLPEC method. By using this method, we preserved the working port and transferred it to the umbilicus. It is known to all that single-incision laparoscopic surgery has the difficulty that the camera and instruments are all operated in-line. It makes the visualization and tissue manipulation more difficult and is time consuming. To minimize the disadvantages, the laparoscope was introduced into the abdomen through a supraumbilical incision, and the grasping forceps was inserted through another infraumbilical skin incision. By this means, the TTPLPEC procedure increases the distance between the laparoscope and the grasping forceps and gains good exposure and operating spaces. In this study, all patients were successfully treated by the TTPLPEC procedure, and no cases were converted to the open operation. Compared with other reports, the operating mean time was short, and the complication rate was low. The TTPLPEC procedure results in two umbilical edge wounds and one or two puncture wounds from the hooked needle. The umbilical wound scars from the laparoscope and forceps are hidden in the fold of the umbilicus, and the puncture wounds from the hooked needle are practically unnoticeable. At follow-up, most patients have no obvious signs of a previous operation after 6 months. Like the other single-port laparoscopic operation, TTPLPEC can also obtain similar scarless result on the abdomen.
The present data suggest that TTPLPEC preserved the advantages of the LPEC procedure and produced excellent cosmetic results. Compared with the current other laparoscopic techniques, this method is safe, feasible, and reliable, has good cosmetics, and has a low recurrence rate. More extensive, prospective, comparative trials and longer follow-up should be done to test the comparative advantages and disadvantages of this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.