
Abstract
Abstract
Background:
Because of improvement in surgical technique and endocrine and exocrine insufficiency management, total pancreatectomy is being frequently performed, especially for benign or low-potential malignant diseases. The laparoscopic approach is rarely performed.
Subjects and Methods:
Our aim is to report two cases operated by the assisted laparoscopic approach and to describe a standardized surgical technique.
Results:
Two patients underwent laparoscopic total pancreatectomy with assisted minilaparotomy or the hand-assisted technique for degenerated intraductal papillary mucinous neoplasms (IPMNs) and neuroendocrine tumors with operative times of 270 and 360 minutes, estimated blood loss of 200 and 300 mL, and a hospital stay of 12 and 18 days, respectively. One patient was re-operated on postoperative Day 10 for bleeding from the hepaticojejunostomy probably related to an inadequate dose of antiproton inhibitors, necessitating refection of the anastomosis with an uneventful course. Pathological examination revealed degenerated IPMNs (T3N1R0) and well-differentiated neuroendocrine tumors (T2NOR0) with complete resection. After 6–10 months of follow-up, the diabetes is well controlled with insignificant episodes of hypoglycemia in 1 patient without any evidence of tumor relapse.
Conclusions:
In selected patients laparoscopic total pancreatectomy appears safe and had many advantages over the open and other laparoscopic pancreatic resection approaches, including first laparoscopic abdominal exploration and no pancreatic anastomosis. Oncological rules can be respected, but further larger studies are needed before drawing conclusions.
Introduction
In this article we describe 2 cases operated on according to a standardized surgical technique.
Patients and Methods
From January 2008 to February 2012, 87 patients underwent laparoscopic pancreatic resections at our Department of Hepatobiliary and Pancreatic Surgery. Data were collected prospectively and included 60 distal pancreatectomies, 11 PDs, 10 enucleations, 4 middle pancreatectomies, and 2 TPs. We began performing major laparoscopic pancreatic resection, requiring a phase of reconstruction, after gaining experience in more than 50 distal resections.
Results
Case 1
A 32-year-old male patient with a body mass index of 36 kg/m2 had MEN 1 with multiple neuroendocrine pancreatic tumors (gastrinoma) revealed by epigastric pain and diarrhea. Symptoms were completely controlled with antiproton inhibitors. An imaging study including computed tomography scan showed at least 14 lesions up to 35 mm in diameter involving the entire pancreatic parenchyma (Fig. 1). Complete radiological and scintigraphic evaluation excluded the presence of extrapancreatic disease. Because of the size of the biggest lesion (35 mm), TP with splenectomy was indicated. A laparoscopic approach with a hand-assisted technique was decided on because of the patient's obesity and to avoid a large subcostal incision. The hand assistance was inserted to free the retroportal tissue, the distal pancreas, and the spleen. Surgery lasted 360 minutes, and there was <300 mL blood loss with no transfusion. The postoperative course was uneventful with 12 days of hospital stay, and then he was transferred for diabetic re-education.
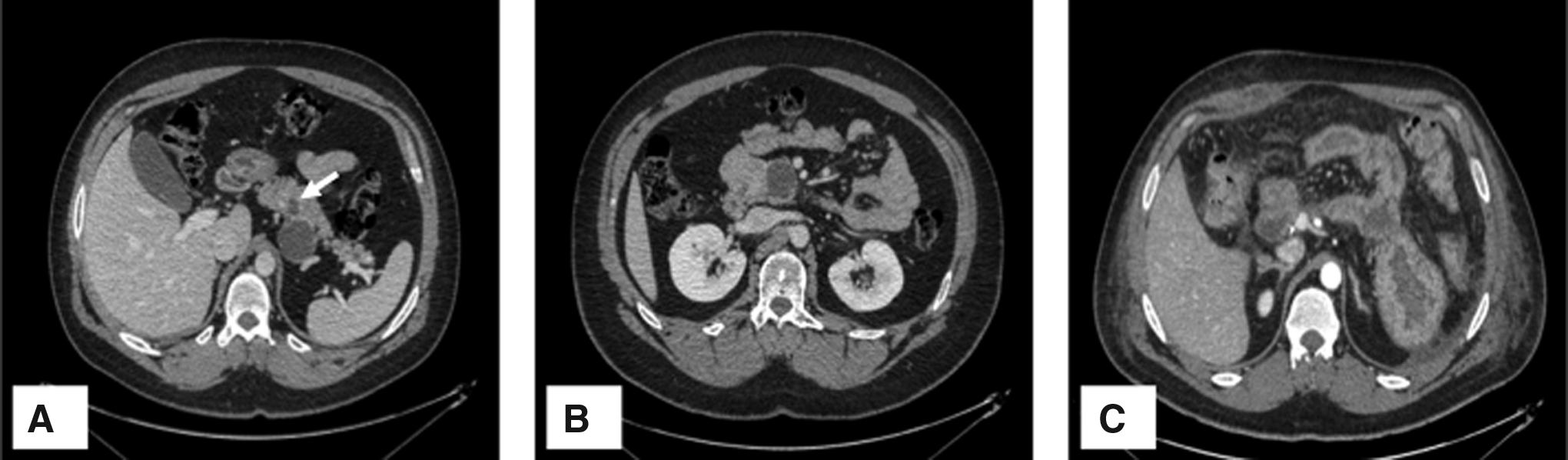
Case 1. Computed tomography scan showing multiple large and small (arrow) cystic neuroendocrine tumors in
Ten days later, he was re-admitted for bleeding from the jejunal loop, probably because the dose of antiproton inhibitors was inadequate for the patient's weight. Transfusion was necessary, and when endoscopic treatment failed, he underwent another laparotomy. At re-operation, the hepaticojejunostomy was healed and patent, the jejunal loop was partially resected, and the hepaticojejunostomy was redone. The postoperative course was uneventful, and the overall patient stay was 18 days.
Pathological examination showed multiple well-differentiated grade 1 neuroendocine tumors (>20) varying in size from microadenomas to 4 cm with a Ki67 of <1%. No lymph nodes metastases were identified from the 20 retrieved nodes, and resection was R0 (pT2N0R0).
After 6 months of follow-up the patient was in excellent condition with well-controlled diabetes and small episodes of hypoglycemia with no evidence of tumor relapse.
Case 2
A 48-year-old male patient was admitted for diffuse degenerated IPMNs discovered after several attacks of acute pancreatitis. Imaging studies including magnetic resonance imaging showed diffuse involvement with endoluminal masses in the head and distal pancreas (Fig. 2). Endoscopic-guided ultrasound biopsy confirmed adenocarcinoma, and LTP with splenectomy was decided. The specimen was completely resected by the laparoscopic approach. Surgery lasted 270 minutes with blood loss <300 mL, and anastomoses were performed by a small 5-cm subcostal incision where the specimen was retrieved. The postoperative course included mild gastroparesia that resolved rapidly and an 18-day hospital stay.
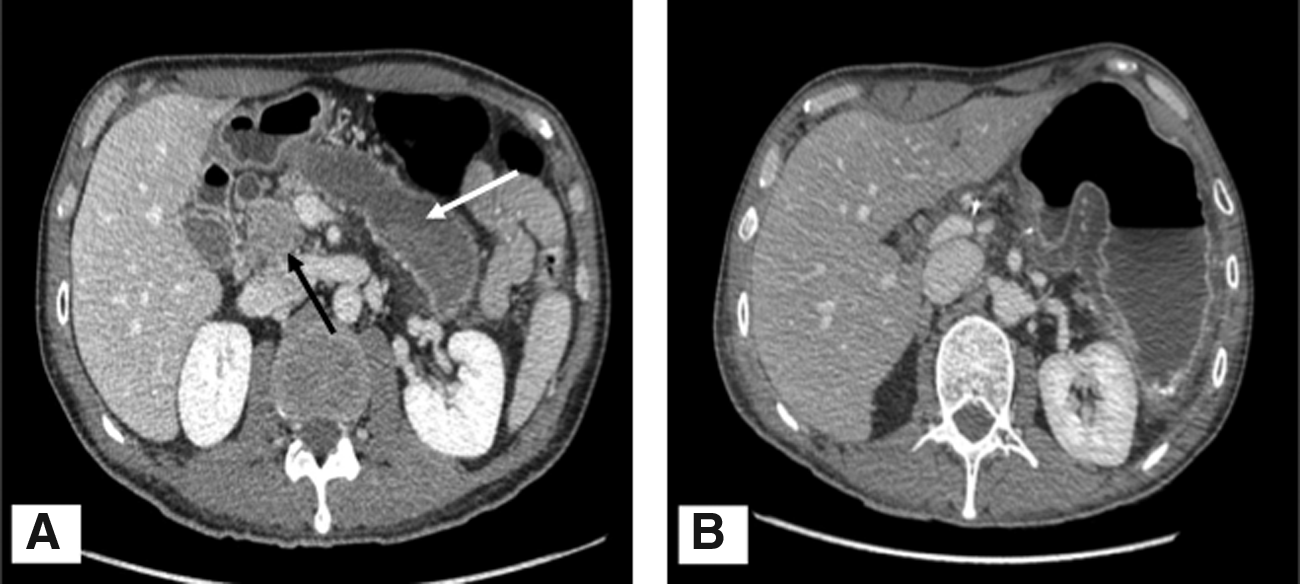
Case 2.
Pathology revealed a mixed-type tubulopapillary intraductal tumor with microinvasive high-grade dysplasia throughout the entire pancreatic parenchyma with three invasive adenocarcinomas, 6, 15, and 20 mm in diameter. Resection was complete (R0) with 1 positive lymph node among 51 retrieved (T3N1R0). The patient received adjuvant chemotherapy.
At 10 months of follow-up, he had well-controlled diabetes without hypoglycemia or evidence of tumor relapse.
Surgical technique
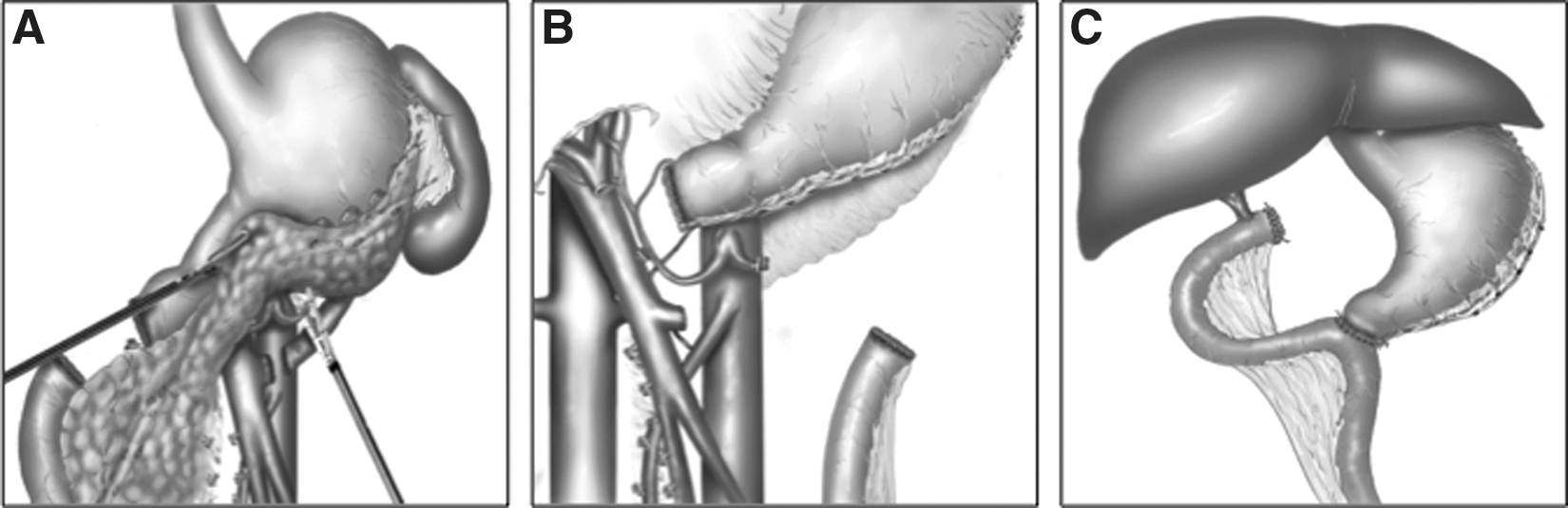
The patient is placed under general anesthesia in the supine position with the legs spread apart and the right arm along the body. Open coelioscopy is performed. Four or five trocars are necessary for this procedure. A 10-mm operator trocar is inserted below the umbilicus or in the lower left quadrant, a 10-mm trocar in the right hypochondrium (lateral, optic), and two 5-mm trocars in the right hypochondrium (medial) and the right subcostal area, respectively. Two other 5-mm trocars can be inserted in the left hypochondrium for a second assistant or in the epigastric area for the stomach if necessary (Fig. 3). The surgeon is positioned between the patient's legs, and the first assistant is on the patient's right (Fig. 3). A Harmonic® scalpel (Ethicon Endo-Surgery, Blue Ash, OH) and a bipolar coagulation device are needed. Once exploration has been completed, the gastrocolic ligament and short gastric vessels (if a splenectomy is planned) are divided, the right mesocolon is freed from the anterior pancreatic head, and the right colonic angle is pushed down. A Kocher maneuver is performed up to the anterior part of the aorta. The inferior pancreatic border is liberated, the superior mesenteric vein is identified, and the gastroepiploic vein of Henley can be divided by ligation or clips to avoid tearing and bleeding when the mesocolon or the pancreatic head is being moved. The third duodenum is completely liberated from the mesocolon, and the ligament of Treitz is sectioned from the right. A cholecystectomy is performed. The right gastric pedicle must absolutely be preserved unless for oncological risk (invasive neoplasm in the head) in order to maintain at least one among the three essential gastric pedicles because the other two pedicles (left gastric and splenic vessels) can accidentally be injured and scarified during the dissection phase or resected for oncological reasons. The bile duct is divided, and a right border lymphadenectomy of the pedicle is performed. Then the first duodenum is sectioned with a stapler after the right gastroepiploic pedicle has been divided and the nasogastric tube has been removed. Lymphadenectomy of the hepatic artery and the left side of the pedicle is completed, and the portal vein is liberated. This maneuver facilitates identification of the gastroduodenal artery, which can be divided by ligation with clips. The superior pancreatic border is liberated, and the hepatic artery is identified. The proximal jejunal loop is sectioned with a stapler, and the mesentery is divided with a Harmonic scalpel. The proximal jejunal loop is pulled from the left to the right of the mesenteric axis (Fig. 4A). The retroperitoneal pancreatic tissue is sectioned after the mesentericoportal vein has been freed from the pancreatic head and the right border of the superior mesenteric artery has been identified. Clips can be placed on the small collaterals of both superior mesenteric vein and superior mesenteric artery (Fig. 4B). Once the pancreaticoduodenal block has been completely freed from the hepatic pedicle and superior mesenteric vessels, it is retracted to the left, thus exposing the splenic vessels. When no invasive component is suspected on the distal pancreas, the spleen may also be preserved with its vessels, with progressive centrifugal dissection of the splenic vessels (Fig. 4B) until removal of the specimen (Fig. 4C). Ligation and division of their small collaterals are facilitated by the use of the Harmonic scalpel and small clips. Otherwise, the splenic artery and vein can be stapled or ligated (Fig. 5A and B), and right-to-left dissection can be performed to free the left pancreas and the spleen from any peritoneal and retroperitoneal adhesions (Fig. 5B). At the same time, sectioning of remnant posterior or short gastric vessels is completed. At any stage of the procedure, a hand-assisted device can be inserted into the right subcostal area for removal or retrieval of the specimen and manual anastomoses (Fig. 5C). The specimen can also be retrieved through an old abdominal or suprapubic incision, and laparoscopic anastomoses can be performed. A drain is left behind the biliary anastomosis and pulled out by the 10-mm trocar of the right hypochondrium.
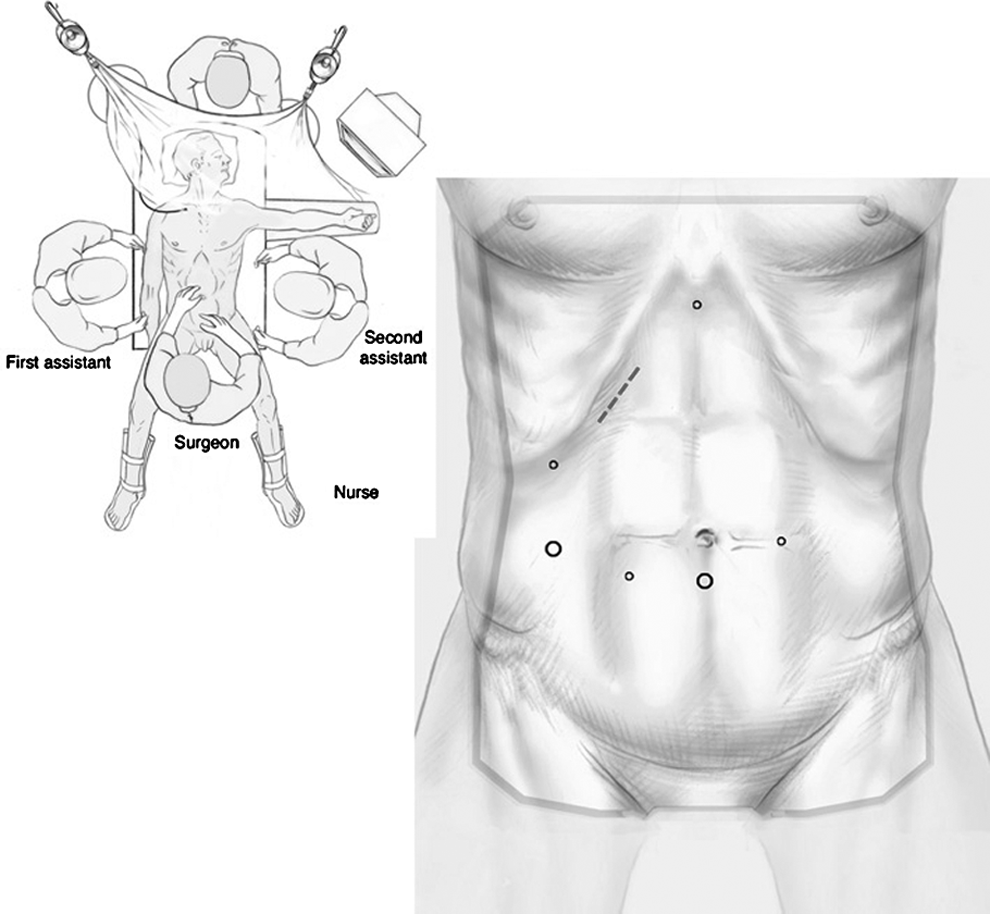
Positions of trocars. Two 10-mm trocars are below the umbilicus and the right hypochondrium for the operator and the optic trocars. The epigastric trocar can be used to tract the stomach if needed, and the other 5-mm trocars can be used for apprehension and exposition. The subcostal incision can serve for the hand-assisted approach and for manual anastomoses.

Discussion
This study, like others, confirms that LTP is feasible and safe.14–17 In selected patients, a short operative time (270 and 360 minutes) and minimal blood loss (200 and 300 mL) can be obtained and are comparable and even lower than with an open approach.10,18 Although many lagers reports on laparoscopic PD had been published,19,20 this technique is still not used extensively because of the complexity of both dissection but especially the reconstruction phase. This technique is applied to selected patients because the median body mass index was 26 (17–40) kg/m2, 19 only 28%–50% had adenocarcinoma,19,20 and 16% had been converted. 20 The median operative time was 568 (536–629) minutes with robot-assisted PD. 20 Besides the general advantages of rapid recovery, esthetics, and pain control, postoperative morbidity and mortality are at least the same, and randomized studies are needed to select the subgroup of patients who can benefit from this approach. On the other hand, laparoscopic left pancreatic resections are more frequent, and larger series on the subject have been reported.21,22 Distal resections are easier to perform, anastomoses are not necessary, and the hospital stay has been shown to be shorter, although no improvement in complications has been demonstrated. 22
Theoretically, LTP could have numerous advantages over the open and other laparoscopic pancreatic resection approaches. Besides the general advantages of laparoscopy, complete exploration can be performed by this approach to exclude any contraindications to resection in patients with advanced or multifocal disease, especially adenocarcinoma, thus avoiding the large subcostal or midline incision needed to thoroughly explore the pancreatic gland and the abdominal cavity by the open approach. The integrity of the abdominal wall must be preserved in these patients especially because this procedure, as in our patients, is performed for benign or low-potential malignant disease with a very good long-term prognosis. Compared with PD, there is no pancreatic anastomosis, which is the Achilles heel of this operation even when a small subcostal incision is used during assisted laparoscopic resection as suggested by some authors. Technically, biliary and duodenal anastomoses are not complicated during TP and can be performed by a pure laparoscopic approach or easily under optimal conditions through a small subcostal or midline incision (5–7 cm). Carcinological rules can be respected because this technique is proposed in a subgroup of selected patients with benign or low-potential malignant disease without suspected mesenteric or celiac vessels involvement. Moreover, in our experience resection was complete (R0) in both cases, and the mean number of retrieved lymph nodes was 20 and 51, respectively. In the case of PD, R0 resection was achieved in 89% of cases,19,20 and the mean number of retrieved lymph nodes was 15–18,19,20 compared with the open approach. 23 In a retrospective comparative study for distal resection for pancreatic adenocarcinoma, short- and long-term oncological results were comparable between the open and laparoscopic approaches. 24 The most reported series on LTP are summarized in Table 1. We conclude from these data that only a few cases were done and that IPMNs represent the first indication for this approach.14–17 In all cases a hand-assisted or assisted minilaparotomy was needed, but a standardized laparoscopic surgical technique that respects the same vascular and carcinological rules as for the open approach and able to provide the same results than open approach has not been described.
IMPN, intraductal papillary mucinous neoplasms; NET, neuroendocrine tumors.
Conclusions
This study confirms that the laparoscopic approach appears safe for TP, which we feel can be very interesting in selected patients and which means that the pool of patients who can benefit from major pancreatic resection by laparoscopy can be extended. Of course, further larger studies are needed before drawing any conclusion on surgical and oncological safety.
Footnotes
Disclosure Statement
No competing financial interests exist.