
Abstract
Abstract
Cases of rare-earth magnet ingestions have been increasingly reported in the literature. However, these descriptions have focused on the severity of the injuries, rather than the clinical presentation and/or therapeutic approach. We report a series of eight children, ranging in age from 2 to 10 years, who ingested powerful rare-earth magnets. The rare-earth magnets were marketed in 2009 under the trade name Buckyballs® (Maxfield & Oberton, New York, NY). They are about 5 mm in size, spherical, and brightly colored, making them appealing for young children to play with and place in their mouths. Three children presented within hours of ingestion, and the magnets were successfully removed via endoscopy in two, whereas the third child required laparoscopy. No fistulas were found in these children. A fourth child presented 2 days after ingestion with evidence of bowel wall erosion, but without fistula formation; the magnets were removed via laparoscopy. A fifth child ingested nine magnets in a ring formation, which were removed via colonoscopy without evidence of injury or fistula formation. The three remaining children presented late (5–8 days after ingestion) and were found to have associated fistulas. They were treated successfully with a combination of endoscopy and laparoscopy with fluoroscopy. None of the children in our series required an open surgical procedure. All children were discharged home without complications. This case series highlights the potential dangers of rare-earth magnet ingestion in children. Our experience suggests that prompt intervention using minimally invasive approaches can lead to successful outcomes.
Introduction
Patients and Methods
We performed a medical record search of all children admitted to Kapiolani Medical Center for Women and Children, Honolulu, HI, with the diagnosis of magnet ingestion over an 18-month period from January 2011 to July 2012. In addition to medical records review, we supplemented our database with reports, clinical images (Figs. 1 and 2), and follow-up information from the pediatric surgeons and the pediatric gastroenterologist involved in the cases (S.M.J., R.K.W., and J.L.K.). This study was approved by Kapiolani Medical Center for Women and Children's Institutional Review Board, and informed consent was obtained from the parents of all of the children included in this case series.
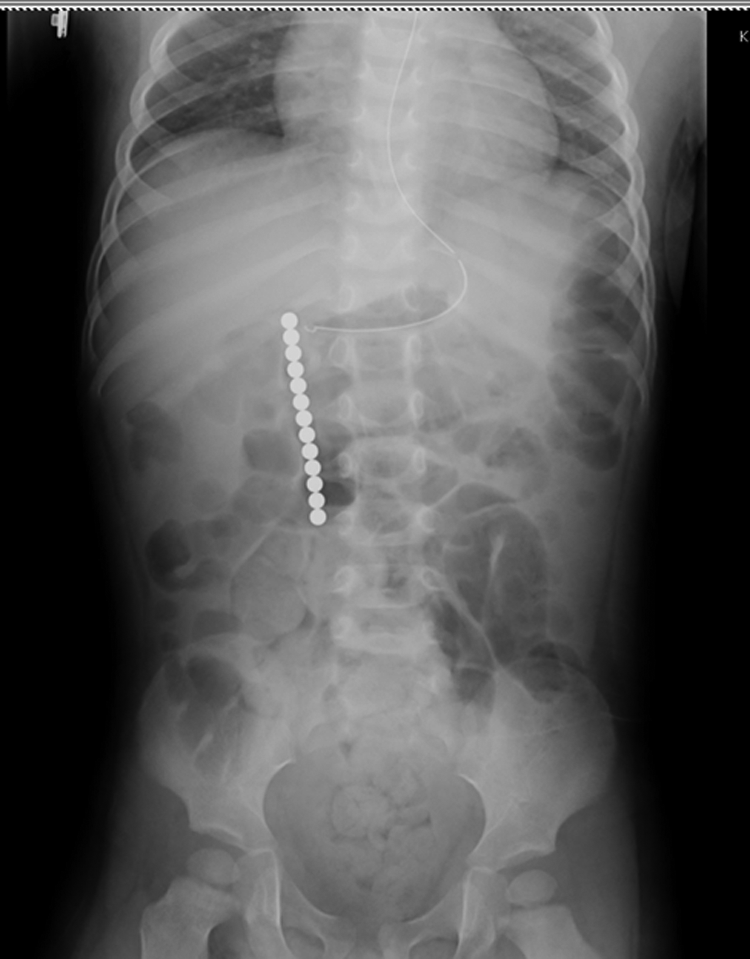
Case 3. Abdominal radiograph showing 13 magnets strung together in a chain just right of the midline.
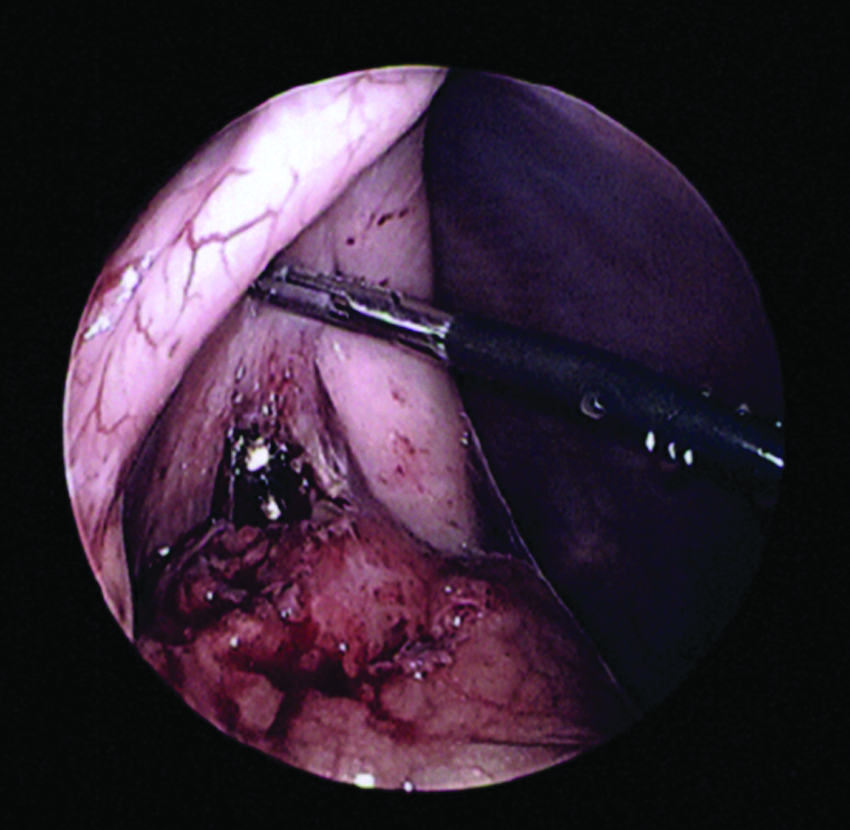
Case 7. Intraoperative laparoscopy demonstrates magnetic foreign body erosion through the posterior stomach wall and into the adjacent loop of the small bowel.
Results
We identified eight children admitted to Kapiolani Medical Center for Women and Children with rare-earth magnet ingestion during the 18-month period of the study. The children ranged in age from 2.5 years to 10 years, with a mean age of 5.5 years. None of the children had any significant previous medical history. It is important that there were no children with developmental delays or disabilities, factors that have been associated with foreign body ingestion. 3
Data from the eight children are summarized in Table 1. In addition, two of these children are described below as brief case summaries to highlight the spectrum of presenting signs and symptoms, treatment, and hospital stay. All of the children were treated successfully with minimally invasive surgical techniques, and all were discharged home without any complications. It is important that no child required a laparotomy as part of treatment.
Including decreased appetite, emesis (bilious or non-bilious), and/or abdominal pain.
C, colonoscopy; E, endoscopy; F, female; L, laparoscopic enterotomy; M, male.
Case 2
A 2-year-9-month-old girl who was previously healthy began coughing while playing with magnets. She was taken to a nearby emergency department where she exhibited non-bloody, non-bilious emesis, as well as signs of mild abdominal pain. The abdominal radiograph revealed 13 magnets aligned in a linear formation. During esophagogastroduodenoscopy, all 13 were removed, and review of the distal esophagus revealed a region of mild injury characterized by erythema and areas of microhemorrhage, corresponding to the location of the first magnet. The stomach appeared normal. The child recovered in the postanesthesia care unit for several hours and was subsequently discharged home uneventfully on the same day.
Case 6
A 4-year-old previously healthy boy presented with acute onset of intense abdominal pain 5 days prior to admission. Additional history revealed multiple episodes of bilious emesis, decreased urine output, and decreased appetite. In the emergency department, an abdominal radiograph revealed three circular opacities stacked vertically in the left upper quadrant. The mother recalled the child and his older brother playing with magnets during a recent trip. As the child was able to tolerate oral fluids in the emergency department, he was scheduled for follow-up imaging the next day, which was unchanged from the original. At esophagogastroduodenoscopy, a crater-like ulcer with raised borders was found in the stomach. A metallic ball was deeply embedded within this lesion. Laparoscopy was performed and revealed that two additional magnets had perforated through the posterior wall of the stomach, through the transverse mesocolon, and into a small bowel loop. These were removed without complication, and the gastrotomy, small bowel enterotomy, and mesenteric defect were all successfully repaired. The first ball was removed by flexible endoscopy from the stomach with fluoroscopic guidance. The child did well postoperatively with resolution of a postoperative ileus within 36 hours and was discharged home on postoperative Day 3.
Discussion
To our knowledge, this article represents the largest single-institution case series of rare-earth magnet ingestion in the literature. It also highlights the success of treatment to discharge using minimally invasive techniques to remove the magnets and repair the fistulas in these eight children, thereby avoiding a more invasive surgical approach such as laparotomy.
Rare-earth magnets appeared on the market in 2003 as components of toys and building sets, with ingestion occurring after the magnets were dislodged from the toys. However, subsequent to a published warning from the Centers for Disease Control and Prevention in 2006, a large voluntary recall removed many of these toys from the market. 2 Later in 2009, rare-earth magnets were marketed as adult desk toys and packaged as multiple magnet units with trade names such as Buckyballs and Nanospheres. In 2011, the U.S. Consumer Product Safety Commission compiled a report reaffirming the risk of rare-earth magnet ingestions by documenting increasing numbers of ingestion reports. 4 Subsequently, the U.S. Consumer Product Safety Commission filed an administrative complaint in an effort to mandate that the company manufacturing Buckyballs notify the public of the hazards of these magnets and offer refunds to their customers. They also asked other manufacturers of rare-earth magnet toys to voluntary recall their products; 11 of 12 companies complied. 6
Magnet ingestions can result in significant bowel injury, inflammation, and even death.2,8,10–16 In 2009, Oestreich 3 reviewed 128 cases of magnet ingestion from 21 countries, including Asia, Europe, and North America, in a 20-year span between 1988 and 2008. Surgical findings reported in the series included intestinal perforation, obstruction, intussusception, ulceration, peritonitis, abscess formation, adhesions, fistulas, volvulus, internal hernia, mesenteric compression, and free magnets in the peritoneum. Surgical therapy and removal of the magnets invariably utilized a formal surgical laparotomy. Although some of the cases reported in this series involved rare-earth magnets (particularly those reported after 2003), no attempt was made to distinguish the effects and potential morbidities associated with different types of magnet ingestion. However, the review did document the frequent delays in referral and diagnosis.
More recent literature has focused specifically on rare-earth magnet ingestions. The North American Society of Pediatric Gastroenterology, Hepatology and Nutrition collected data on the prevalence of rare-earth magnet ingestions through an informal survey of pediatric gastroenterologists throughout the United States. 6 Eighty cases of rare-earth magnet ingestion were identified. From the data collected, a proposed algorithm for management of children with rare-earth magnet ingestions was developed. The algorithm detailed a management approach based on presenting symptoms and magnet location including observation, endoscopy, and surgical intervention. Finally, two recent reports in the literature described 3 cases of magnet ingestion in which all three children underwent open laparotomy.7,8 Endoscopy and laparoscopy were not attempted in these cases.
In our series, three children presented early after they were suspected of magnet ingestion when they were observed playing with the magnets, and medical care was sought promptly. Two of these children were asymptomatic, and one was mildly symptomatic. Removal was accomplished without delay via endoscopy in two, whereas laparoscopy was used in the third child to retrieve magnets that had passed into the proximal small bowel. One of these early-presentation children who had minimal symptoms demonstrated mucosal injury on endoscopy. A fourth child presented late after ingesting nine magnets bound together in the shape of a ring but, probably because of this anomaly, did not suffer fistula formation or mucosal injury as the ring-shaped magnet complex was successfully removed during colonoscopy. The fifth case involved a child who notified his parents of his ingestion 2 days following the ingestion after developing symptoms of abdominal pain and decreased appetite. He was found to demonstrate bowel wall erosion, with early signs of fistula formation. Three of the remaining children presented 5–8 days after ingestion. These children had a variety of symptoms that included abdominal pain, vomiting, and changes in appetite. They were treated successfully with a combination of endoscopy and laparoscopy guided by fluoroscopy. In addition to removing the magnets, all three had associated fistulas, which were successfully closed. Finally, the eight children in this series were all discharged home uneventfully and without complication.
Our institutional experience adds to growing literature that documents the dangers of rare-earth magnet ingestion. We speculate from our experience that prompt intervention may reduce the potential risk of complications such as fistula formation. Strong attractive magnetic forces possessed by rare-earth magnets, when apposed to one another after multiple magnet ingestion, increase the risk of mucosal tissue entrapment, tissue compression, and ultimately fistula formation. Based on the experience gained in this series, we believe that complications occur in a time-dependent fashion, with fistula formation occurring sometime between 2 and 5 days, and that prompt intervention can prevent or reduce impending tissue damage and injury. Moreover, our case series suggests that other factors are also important in determining injury because one of the children who presented within hours of ingestion had evidence of mucosal injury and microhemorrhage, whereas the late-presenting child who ingested the ring-shaped magnet complex had none.
It is important to emphasize that none of the eight children in our series required an open abdominal procedure, as commonly reported in the literature.2,4,7,8,12,13,16 They were treated successfully with a minimally invasive approach consisting of endoscopy, laparoscopy with the option of fluoroscopy, and colonoscopy. It is interesting that metallic laparoscopic and endoscopic instruments aided in removal because of their strong attractive forces with the rare-earth magnets. In cases of magnet groups located in different areas of the abdomen, fluoroscopy aided rapid localization of additional magnets. In all cases requiring laparoscopic removal, intraoperative radiographs were used to confirm complete removal of the magnets.
Finally, we recommend that primary healthcare providers, emergency department physicians, and pediatric hospitalists who encounter children suspected of magnet ingestion involve their pediatric gastroenterologists and surgeons early and consider using this menu of minimally invasive surgical approaches as initial therapy before resorting to laparotomy. We also suggest that intervention be initiated early and without delay to avoid the risk of progressive tissue damage, fistula formation, and other more serious morbidities and mortality.
Footnotes
Acknowledgments
We are grateful to Dr. David Easa for his countless revisions, suggestions, and guidance during the process of writing this case report. We would also like to thank Dr. Kate Powers for her assistance with this project.
Disclosure Statement
J.L.K. is a consultant for Nutricia. J.S.K., S.M.J., G.G., and R.K.W. declare no competing financial interests exist.