
Abstract
Abstract
Objective:
Extensive surgery is the mainstay of therapy for patients with gastrointestinal mesenchymal tumors (GIMTs) adjacent to the esophagogastric junction (EGJ). However, this modality is invasive and may interfere with anatomic consistency of the digestive tract. Therefore, we evaluated the feasibility, safety, and efficacy of endoscopic submucosal dissection (ESD) for GIMTs close to the EGJ and factors related to incomplete resection.
Patients and Methods:
For 39 GIMTs adjacent to the EGJ in 39 consecutive patients, the baseline information, complications, and therapeutic outcomes were recorded. Subsequently, risk factors, focusing on age, sex, tumor size, extent, shape, perforation presence/absence, and histopathology, were analyzed.
Results:
Complete removal of junctional GIMTs was achieved in 32 cases, giving an overall complete resection rate of 82%. The mean tumor size was 16.1±12.7 (median, 12; range, 4–50) mm. There were no major intra- and postoperative complications, but two small perforations were found. The final histopathologic diagnoses included 28 leiomyomas, 10 gastrointestinal stromal tumors, and 1 schwannoma. No local recurrence or distant metastasis was observed during a mean follow-up of 15.7±8.4 (median, 16; range, 6–35) months. Univariate analysis showed incomplete resection was associated with tumor shape and size. Multivariate regression analysis identified tumor irregularity (odds ratio=37.50, 95% confidence interval=4.253–330.627) as the single factor associated with incomplete resection.
Conclusions:
ESD is feasible and safe for well-selected patients with GIMTs adjacent to the EGJ. Irregular tumor shape should be considered as a technical difficulty while performing ESD. Oncologic outcomes need to be assessed with longer follow-up.
Introduction
Endoscopic submucosal dissection (ESD) has been introduced for both superficial and submucosal tumors (SMTs) in the vicinity of the EGJ. However, the utility and safety of ESD for GIMTs adjacent to the EGJ have not been fully understood, and investigation of factors in relation to incomplete resection is still lacking. Therefore, we aimed to determine the feasibility, efficacy, and safety of ESD for GIMTs adjacent to the EGJ and factors associated with incomplete resection.
Patients and Methods
Patients
We queried the electronic database and medical charts of patients who underwent ESD and identified 39 GIMTs adjacent to the EGJ from September 2008 to March 2012. It is of note that our study was performed retrospectively, but the patients eligible for ESD were at the discretion of the practitioners on index examination. Indication criteria were as follows: (1) an endophytic and intraluminal GIMT without ulceration, (2) maximal diameter ≤5 cm, (3) no evidence of lymph node involvement or distant metastasis, (4) blood platelet counting and coagulation within normal limits, and (5) written informed consent to accept ESD after detailed statement of both the advantages and drawbacks of this endoscopic intervention.
All patients had routine upper endoscopy to assess the location, extent, appearance, and motility of the lesions. Endoscopic ultrasonography (EUS) was performed with a 7.5–15 MHz catheter probe (model SP701; Fijinon, Omiya, Japan) to determine the size, echogenicity, and layer of origin of the tumors. EUS can also be used to exclude adenopathy or distant metastasis as well as computed tomography. EUS-guided fine needle aspiration was not adopted at our institution because of inconclusive necessity, elusive diagnostic certainty, and increased risk of hemorrhage and tumor dissemination.2,3
This study was carried out at the endoscopy center of Tianjin Medical University General Hospital, Tianjin, China, and was approved by the institutional ethical committee.
ESD procedure
Before ESD, all patients were asked to undergo a fasting period of at least 12 hours and water deprivation for 8 hours. The cardiopulmonary function was monitored by an anesthetist following endotracheal intubation in an endoscopy unit. The patients were generally anesthetized by intravenous injection of midazolam and/or propofol.
All ESD procedures were performed by three experts (Z.Z., B.W., and W.L.) and a beginner (T.W.). When the beginner performed ESD, an expert provided complete support as an assistant and replaced the beginner whenever needed. A single-channel endoscope (model GIF-Q260J; Olympus, Tokyo, Japan) and/or a double-channel endoscope (model GIF-2TQ260M; Olympus) was used. A transparent hood (model MH-593; Olympus) was attached to the tip of the endoscope for a good visualization. The electrosurgical current was applied using an electrosurgical generator (model ICC 200; Erbe, Tübingen, Germany).
The procedure of ESD is illustrated in Figure 1. In brief, the tumor was marked with several dots around the lesion using argon plasma coagulation (APC) (model APC300; Erbe). Then a saline solution combined with epinephrine, glycerin fructose, and methylene blue was injected into the submucosa with an injection needle (model NET 2522-G4; Endo-Flex GmbH, Voerde, Germany). The injection was repeated in order to create a fluid cushion for separating the submucosa from the underlying proper muscle layer, limiting bleeding and preventing perforation. Subsequently, a circumferential incision was made along the margin of the targeted lesion with a hook knife (model KD-620LR; Olympus). We carefully dissected the surrounding tissue at the level of the deepest submucosal layer and shelled the connective muscular fibers and stalks along the capsule of the tumor with an insulated-tip knife (ITknife2 model KD-611L; Olympus), a hook knife, or a hybrid knife (JET2; Erbe) at the surgeon's preference. Once the tumor was completely exposed, it was cut off at the root using an electrosurgical knife. Sometimes a snare (model NOE 342217-G; Endo-Flex GmbH) was used to remove the tumor by capturing its base. Finally, the resection specimen was obtained through the mouth for pathologic evaluation, the endoscope was reinserted to confirm a clean margin of the incision site, and any macroscopic vessels on the wound surface were electrically coagulated by APC. The residual defect was closed using metallic clips (model HX-610-135L; Olympus) if needed.
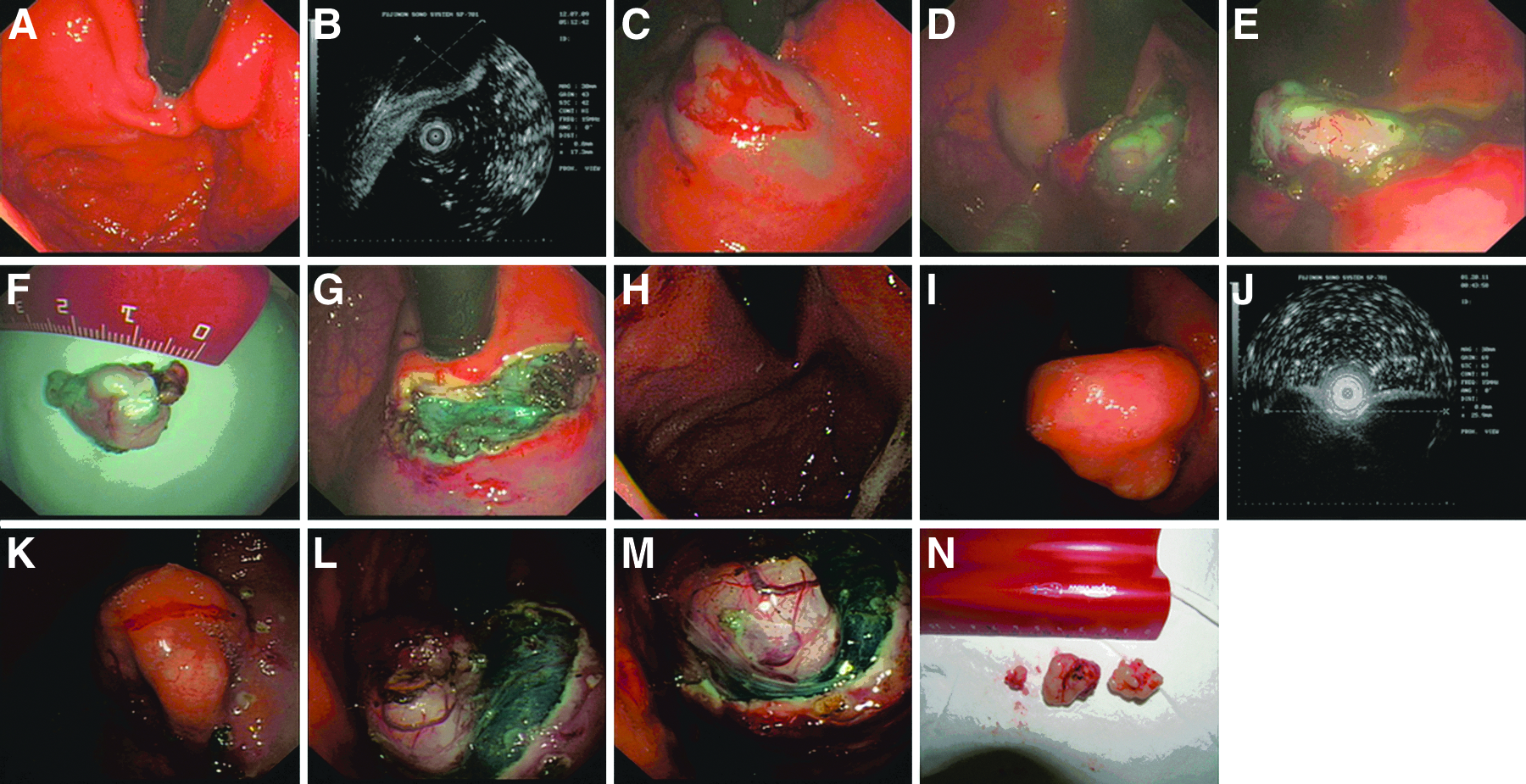
Endoscopic submucosal dissection procedure.
Pathologic evaluation
The resection specimen was fixed in 10% formalin, then embedded in paraffin, and stained with hematoxylin–eosin. The immunohistochemical analysis was performed with smooth muscle antigen, desmin, S-100, CD117 (c-kit), CD34, and DOG1. The diagnosis of GISTs was based on positive staining for CD117 or DOG1 and CD34. The risk stratification of GISTs was determined in accordance with tumor size and mitotic index. A tumor that was positive for smooth muscle antigen and/or desmin was diagnosed as leiomyoma, and S-100 positivity was diagnosed as schwannoma.
Follow-up
Proton pump inhibitor and sucralfate were routinely administered for artificial ulcer healing. All patients received follow-up endoscopy at 1, 6, and 12 months after the initial ESD therapy during the first year and thereafter annually. Moreover, any suspicious postoperative complications, such as stenosis or reflux diseases, were recorded at follow-up visits.
Definitions and data analysis
GIMTs adjacent to the EGJ referred to tumors whose upper margin was ≤3 cm away from the gastric inlet. This perigastroesophageal junction was divided into cardia (≤1 cm) and subcardia (>1 cm) groups according to the distance between tumor margin and gastric inlet. Furthermore, the tumor was classified as regular or irregular by whether the shape of the lesion was round/oval or not (Fig. 2).
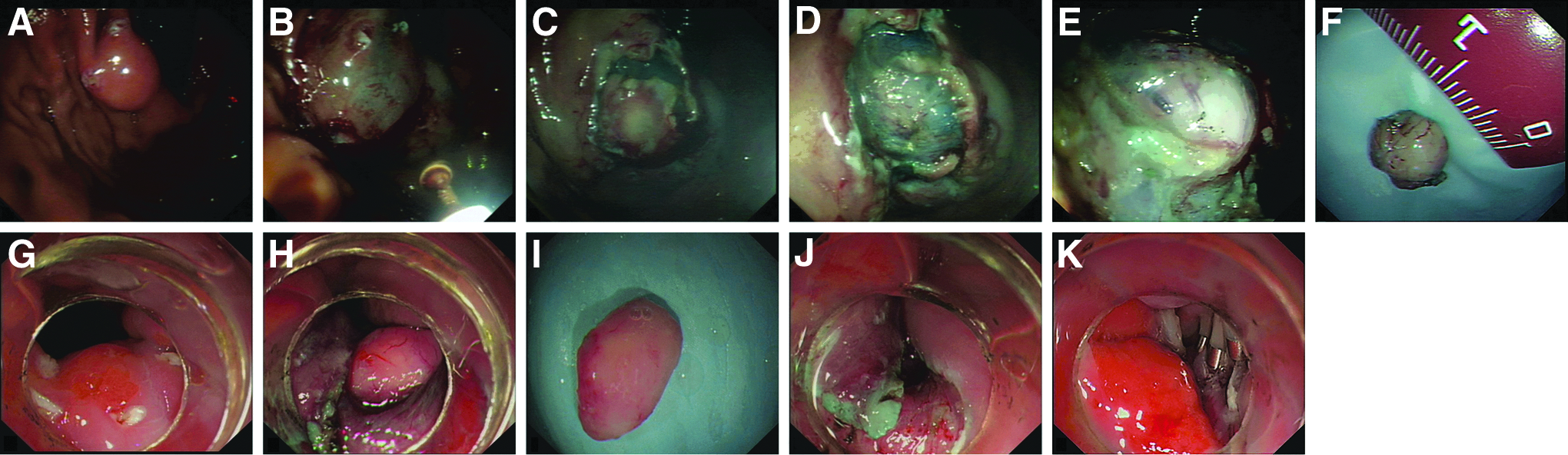
Examples of endoscopic submucosal dissection for regular gastrointestinal mesenchymal tumors adjacent to the esophagogastric junction.
Major bleeding was defined as symptomatic bleeding with the need for blood transfusion or endoscopically uncontrollable bleeding with conversion to surgery. We endoscopically diagnosed perforation as a gross defect detected during ESD, with extraluminal organs, mesenteric fat, space visible through the lesion, and/or by the presence of free air on a plain radiograph just after dissection.
A complete resection referred to a tumor that had to be removed en bloc without rupture or spillage and the resection margin was proved to be tumor free microscopically.
A beginner referred to an endoscopist who started with firsthand observation and progressively performed an initial 30 cases of ESD for GIMTs under strict supervision by an experienced endoscopist. Furthermore, the beginner had previous experience and skill with various instruments, devices, and endoscopic procedures such as band ligation, polypectomy, endoscopic mucosal resection, and ESD for epithelial neoplasms.
We evaluated the associations between incomplete resection and the following factors: age, sex, tumor size, extent, shape, perforation presence/absence, and histopathology.
Statistical analysis
Data are given as mean±standard deviation (median, range) values or simple proportion as appropriate. Differences in the means of continuous data were compared by Student's t test. Categorical data were compared using the chi-squared test or Fisher's exact test. To identify significant parameters for incomplete resection of junctional GIMTs by ESD, risk factors with P values<.1 in the univariate analysis were included in a forward, stepwise multivariate logistic regression model. A P value<.05 was considered significant, and all tests were two-sided. SPSS software version 18.0 (SPSS Inc., Chicago, IL) was used for statistical analysis.
Results
Baseline characteristics of all patients and GIMTs
The baseline information is shown in Table 1. There were 39 GIMTs adjacent to the EGJ in 39 consecutive patients. All lesions originated in the muscularis propria with hypoechoic sonography on EUS (33 cases received EUS at our institution, 6 outside). Computed tomography scan was also performed on 14 patients. Accordingly, all recruited GIMTs presented with an endophytic and intramural growth pattern without adenopathy or distant metastasis. The majority of GIMTs were incidental findings (22/39 [56%]), and epigastric pain (7/39 [18%]) was the most common manifestation. The co-morbidities were hypertension, chronic hepatitis B, and diabetes mellitus in 6, 2, and 2 patients, respectively. All these concomitant situations were assessed and allowed for ESD with an anesthetist's supervision. Among the 3 patients with GISTs, an 8-mm tubular adenoma in the antrum, a 15-mm serrated adenoma, and a 5-mm GIST in the body of each case were found.
These data were expressed as mean±standard deviation values.
GIMT, gastrointestinal mesenchymal tumors.
Therapeutic outcomes and complications
The mean tumor size was 16.1±12.7 (median, 12.0; range, 4–50) mm. Fragments of resected specimen were retrieved in 6 cases (two to four pieces), and a positive deep resection margin was detected on pathologic examination in 1 case. Overall, the complete resection rate was 82% (32/39). Perforations occurred in 2 patients, and both were endoscopically repaired by clips. They experienced moderate abdominal distension without peritoneal irritation sign and fever and were given intravenous broad-spectrum antibiotics and continuous nasogastric depression. The final histopathologic diagnoses were 28 leiomyomas, 10 GISTs, and 1 schwannoma (Table 2). The GISTs cases included 7 at very low risk and 3 at low risk (Table 3). At this writing, all patients are uneventful during a mean follow-up of 15.7±8.4 (median, 16; range, 6–35) months. No gastrointestinal stricture or reflux disease was documented.
These data were expressed as mean±standard deviation values.
GIST, gastrointestinal stromal tumor.
Positively deep resection margin.
F, female; HPF, high-power field; M, male.
Risk factors in relation to incomplete resection
There were 32 patients with complete resection versus 7 cases with incomplete resection. The results of univariate analysis are displayed in Table 4. There was no statistical significance in age, sex, perforation presence/absence, and histopathology. There was a trend toward cardiac GIMTs in the incomplete resection group, with 5 of 16 in comparison with 2 of 23 subcardiac tumors. However, this did not meet statistical significance (P=.101). In contrast, the incomplete resection of ESD for GIMTs adjacent to the EGJ was influenced by tumor size and shape. The tumor size were significantly larger in the incomplete resection group, with a mean size of 26.7±14.9 mm compared with 13.7±11.1 mm (P=.012). When stratified by size, the complete resection rate with size <10 mm, 10–20 mm, and >20 mm was 100%, 73%, and 63%, respectively. Lesions with irregularity had a significantly higher rate of being in incomplete resection group (P=.001). Multivariate logistic regression analysis identified irregular tumor shape (odds ratio=37.50, 95% confidence interval=4.253–330.627) as an independent risk factor correlated with incomplete resection (Table 5).
Data are n (%).
These data were expressed as mean±standard deviation values.
GIST, gastrointestinal stromal tumor.
Discussion
Originally, GIMTs poorly located at the EGJ, especially for GISTs, are always recommended for total/proximal gastrectomy with concerns of the operative risks and anticipated recovery against oncologic benefits. 1 However, such major surgery entails the risk of overtreatment and diminishes postoperative life quality. 4 It may result in deformity of the EGJ and lower esophageal sphincter, consequently violate the integrity and function of this area, and give rise to suffering morbidity such as anastomotic stenosis or reflux disease.5–8
More recently, various types of laparoscopy have been developed as alternatives to perigastroesophageal junctional GIMTs. They comprise laparoscopic partial resection,5,9–15 enucleation,4,15 and endoscopic–laparoscopic hybrid surgery.16,17 However, several shortcomings of these methods should not be ignored as follows: some techniques require a high level of expertise and competence; it is tedious to precisely localize the tumors and to confirm the cutting lines, particularly in small lesions on the posterior wall or showing mainly an endophytic growth pattern; and there is a risk of intraperitoneal contamination with gastric juices while performing gastrotomy and possibility of port-site infection.
ESD, a newly developed technique, has been introduced as a standard treatment for early gastric cancer in Asian countries. Recently, ESD has spread to both superficial tumors and SMTs in notoriously difficult locations such as the EGJ and duodenum with promising results.18–22
Li et al. 20 performed endoscopic resection in 143 cases, which was to our knowledge the only study naturally designed for evaluating the feasibility of ESD for tumors originating in the muscularis propria at the EGJ. In 8 patients, the specimens were partly resected, giving a complete resection rate of 94%. Perforations occurred in 6 cases with a rate of 4%. However, other ESD-derived modalities were also used in that study, which would have positively affected the resectability of the standard ESD procedure, and factors associated with incomplete resection were not identified. Moreover, the authors also stated inevitable bias because their institution is the main center of treating SMTs of digestive tract in China. Considering this, we believe that our practice is able to add some basic knowledge and information in an area that has a paucity of available data in the current literature.
In this study, we applied ESD in 39 GIMTs adjacent to the EGJ and obtained an overall complete resection rate of 82%. In contrast, six leiomyomas were removed in pieces, and one GIST was confirmed with a positively deep resection margin. Our complete resection rate was 87% (27/31) and 63% (5/8) for tumors with size ≤20 mm and >20 mm, respectively. This is lower compared with previous studies as well as a recent report by Liu et al. 23 but matches the results from a Western group. 24 In the latter series, they achieved a complete resection rate of 60% in five cardiac SMTs and speculated that only about 65% of SMTs arising from the muscularis propria could be successfully removed. The discrepancy in these results may be due to the small number of available patients, selection bias, and retrospective design.
One ongoing criticism regarding the treatment of potentially malignant pathology by minimally invasive approaches is whether these methods provide an oncologic adequacy. More recently, Lee et al. 25 reported an analysis of 151 consecutive gastric SMTs in accordance with tumor location. It is interesting that they found leiomyoma was the most frequent neoplasm in the cardia/EGJ and that cardiac SMTs mainly presented with an endophytic growth pattern and smaller size. Furthermore, the proportion of GISTs with very low and low risk was higher in the cardia than any other site despite statistical insignificance. GISTs, stratified from very low to low risk, were diagnosed in 26% of our study population, and all except one were removed en bloc with a negative margin. Taken together, our results suggest that patients with GIMTs adjacent to the EGJ, especially for leiomyomas and relatively “benign” GISTs, could be spared total/partial gastrectomy so that the gastrointestinal continuity is preserved, so as to avoid overtreatment and to obtain better postoperative recovery.
Given that almost one-fifth of all cases (7/39) were incompletely resected in our study and a definite pathologic diagnosis of GIMTs before or even during intervention remains difficult, the oncologic outcomes should be extrapolated with caution in the short term. As mentioned in the NCCN guidelines, 1 all GISTs, based on their size and mitotic index, may have malignant potential. In this regard, different postoperative strategies should be performed. It is fair enough to adopt EUS-based follow-up investigation for leiomyomas and schwannomas, whereas we need to do more for incompletely resected GISTs.
The patient in our series with a positively deep resection margin had a low-risk GIST (2.5 cm in diameter and 0–1 mitoses/50 high-power fields). He refused additional open surgery and currently remains disease free after a 26-month follow-up. This is consistent with the results of a recent study conducted by Kim et al. 26 In that series of 136 primary gastric GISTs ≤5 cm, none of 14 patients with a microscopically positive resection margin showed recurrence during a median follow-up of 32 months, and they concluded that high mitotic indices and abnormal p53 expression were only predictors of recurrence. However, if spillage on a higher-risk GIST resulted from the ESD procedure, more intensive postoperative surveillance or adjuvant therapy should be considered.
Imatinib, a tyrosine kinase inhibitor, has been approved for postoperative treatment of GISTs by the Food and Drug Administration and for patients at a high risk of recurrence after complete resection in Europe. Although the optimum duration has not been determined, a recent trial demonstrated that 1 year of imatinib at 400 mg/day prolonged recurrence-free survival after resection of GISTs. 27 The NCCN 1 also recommends postoperative imatinib for intermediate- to high-risk GISTs for at least 12 months; moreover, longer adjuvant therapy may be required for higher-risk patients. In 2008, a modified risk classification of GISTs was advocated, and tumor rupture was considered an independent factor of relapse. 28 From the oncologic point of view, we believe that patients with GISTs undergoing spillage or rupture are candidates for adjuvant imatinib with permission.
Upon univariate analysis, our results underscored the importance of tumor size and shape relevant to incomplete resection. The complete resection rate declined with increased size and irregular tumor shape. However, the current study was underpowered to adequately assess the association between tumor extent and incomplete resection. Although it may be intuitive that the manipulation would be harder for cardiac tumors owing to the narrow lumen, sharp angle, and retroflexion of the endoscope, this study did not demonstrate a clear association. One possible mechanism is that the muscle layer of the cardia is thicker than that of the subcardic area because of the constitution of the lower esophageal sphincter, which may facilitate endoscopic management. 20 Despite lacking statistical significance, a trend toward cardiac GIMTs in the incomplete resection group (P=.101) was of note. In this context, this trend merits attention when an endoscopist attempts to perform ESD for cardiac GIMTs. In addition, Omae et al. 19 studied 44 cases of early EGJ cancer, and the curative resection was not influenced by circumferential locations, namely, the anterior wall, greater curvature, posterior wall, and lesser curvature. Multivariate logistic regression analysis revealed tumor shape was the only independent factor. We speculated it was owing to difficulties in stably positioning the electrosurgical knifes at precise direction and depth, verifying the cutting margin, and dissecting along the tumor edge, especially for irregular lesions.
Perforations occurred in 2 patients, and both were successfully repaired by the endoscopic application of clips, with a rate of 5% comparable to previous reports.20,24 No perioperative bleeding was encountered. In terms of our expertise, minor oozing and grossly feeding vessels can be directly occluded using electric hot biopsy forceps or APC after the wound is washed with icy saline solution combined with 8% norepinephrine. Metallic clips were used for hemostasis when the abovementioned methods were ineffective or more gushing bleeding happened. After complete resection, it was necessary to occlude all exposed vessels on a resected defect with APC or clips. Administration of proton pump inhibitor, an intravenous drip of 40 mg of omeprazole twice daily, was routinely used from the day of ESD to at least 48 hours after the procedure at our institution. Next, regular intake of 20 mg of esomeprazole was continued daily for approximate 1 month to improve ulcer healing.
No gastrointestinal stenosis was observed in our series. An extent of the mucosal defect of more than three-quarters circumferentially or >5 cm longitudinally was a significant risk factor for occurrence of post-ESD stenosis in cardiac resection. 29 All patients in our study had less than three-quarters circumferential and <5 cm longitudinal extent of the mucosal defect after ESD. This discrepancy of included patients can explain the difference with regard to the rate of cardiac stenosis. In addition, resection of the EGJ area, and thus the lower esophageal sphincter, may result in a situation of acid and bilirubin reflux, consequently exposing the patients to a high-risk environment for acquisition of Barrett's metaplasia. 30 However, our outcomes revealed no postoperative symptoms of reflux, probably due to sacrificing as little normal gastric wall of the EGJ as possible, which composed the antireflux mechanism, by performing ESD.
There is little consensus evaluating the appropriateness of endoscopic management in patients with GIMTs, although some pioneers have made an attempt. With respect to oncologic outcomes, the threshold for surgical intervention and conversion to laparotomy should be low. Ganai et al. 31 reported that size greater than 8 cm was an independent predictor of conversion to open surgery during the laparoscopic performance for gastric SMTs. Therefore, we recommend both biological and technical issues should be considered in selection of optimal intervention for GIMTs adjacent to the EGJ. Although ESD can be an alternative to laparoscopic or open approaches in well-selected patients, full surgical resection should be adopted if the results of preoperative workup are deemed suspicious of a more aggressive entity (e.g., GISTs with high mitotic index, presence of ulceration) and technical complexity (e.g., irregular shape, larger size, exophytic growth pattern). A multidisciplinary team may help in decision-making and perioperative emergency.
Our study still has some limitations. First, it is a retrospective review with selection bias due to the inclusion criteria. This could explain the relatively small mean size of the enrolled sample. However, it is not arbitrary to restrict the tumor size amenable for ESD within 5 cm, taking account of the ambiguous biological nature and potential malignancy of all GISTs. 32 Second, because the majority of our cases have occurred in the past 4 years, we cannot comment on long-term oncologic outcomes, so that further investigation is needed. Third, our cohort is small; therefore accumulation of data from multicenter studies including larger numbers may confirm our findings and more accurately predict incomplete resection. Finally, we do not compare ESD with other surgical, laparoscopic, or endoscopic resection manners. In fact, the endoscopic submucosal tunnel technique has also been adopted at our institution for treating patients with achalasia, and seven SMTs, including two at the cardia, were attempted for en bloc removal by the tunnel technique since August 2011. 20 However, our preliminary experience is limited, so that the indications of this advanced modality should be well established with further assessment. Also, the technique we used here is easily adaptable to an endoscopist already comfortable performing standard ESD. From our practical perspective, it is suggested that an endoscopist start with relatively small GIMTs (e.g., <20 mm) with regular shape that are located in the lower portion of the stomach, which are easier to access and to manipulate.
In conclusion, ESD is feasible and safe for well-selected patients with GIMTs adjacent to the EGJ, and irregular tumor shape should be considered as a technical difficulty while performing ESD. Oncologic outcomes need to be assessed with longer follow-up.
Footnotes
Acknowledgments
This study is partly supported by the National Nature Science Foundation of China (grant 81000157 to Q.X.Y.). We thank all the doctors, nurses, and pathologists who participated in this study over the years.
Disclosure Statement
No competing financial interests exist.