
Abstract
Abstract
Introduction:
Various techniques and energy-based devices have been used to minimize the blood loss during transection of the liver parenchyma laparoscopically. The laparoscopic Habib™ 4X sealer (Rita Medical Systems, Inc., Fremont, CA) is a promising device using bipolar radiofrequency energy. The purpose of the study was to test the safety and the efficiency of the device in laparoscopic left lateral sectionectomy.
Patients and Methods:
Five patients underwent laparoscopic left lateral sectionectomy using the laparoscopic Habib 4X in a period of 12 months. Indications for liver resection were hepatocellular carcinoma in 2 cirrhotic patients and colorectal cancer liver metastasis in 3 patients. Technical aspects were analyzed.
Results:
All the patients underwent formal laparoscopic left lateral sectionectomy. The Pringle maneuver was not applied in any of the patients. Mean operative time was 75 minutes (range, 60–90 minutes). Bleeding control along the transection line was satisfactory. No conversion to laparotomy was required. Operative blood loss was minimal. No blood transfusion was recorded. The postoperative period was uneventful. Median hospital stay was 3 days (range, 2–5 days). Histopathology revealed that the margins were disease free.
Conclusions:
Laparoscopic left lateral segmentectomy with the use of Habib 4X proved safe and efficient. This technique may be an initial step for surgeons shifting to laparoscopic liver surgery provided they have previous experience in laparoscopic and liver surgery. Well-designed controlled randomized studies are needed in order to evaluate further the role of the device used in the present study in minimally invasive liver surgery.
Introduction
The use of bipolar radiofrequency (RF) energy has overcomed the limitations of monopolar energy, namely, the elimination of collateral damage to adjacent structures and avoidance of the heat-sink phenomenon. Especially for laparoscopic use, bipolar RF energy has been already successfully applied in liver resections, partial nephrectomies, and distal pancreatectomies. 3 On these lines, the Habib™ 4X sealer (Rita Medical Systems, Inc., Fremont, CA) is a well-established device in open surgery using bipolar RF energy. Recently, it has been successfully tested in laparoscopic resections, proving to be feasible and safe with minimal blood loss liver resection. 4
The purpose of the study was to standardize the application of the device in our initial experience. Technical aspects using the laparoscopic Habib 4X in laparoscopic liver resection are also analyzed.
Patients and Methods
Five laparoscopic left lateral liver resections in 3 male and 2 female patients with a mean age of 65 years (range, 55–75 years) were carried out in a period of 12 months. Indications for liver resection were primary hepatocellular cancer of Child Class A with hepatitis B virus–positive cirrhosis in 2 patients, whereas colorectal cancer metachronous metastasis was the diagnosis for the other 3 patients. All patients were preoperatively staged with abdominal contrast-enhanced computed tomography, which delineated the lesions in liver segments II and III. Extrahepatic disease was excluded. The mean lesion diameter was 3 cm (range, 2–4 cm). Based solely on imaging criteria, a left lateral liver resection was decided on in the preoperative setting. Patients were informed of the innovative nature of the procedure, and consent was obtained prior to surgery.
All the operations were performed by two certified hepatopancreatobiliary surgeons (D.Z. and L.R.J.). The laparoscopic Habib 4X (model LH4X) was used in all cases. The laparoscopic Habib 4X consists of a 2×2 array of needles arranged in a rectangle and uses bipolar RF energy. It measures 45 cm in length with a protected insulated area to allow 5 cm in length for RF. The device can be introduced via a 10–12-mm laparoscopic port (Fig. 1). It is connected to a generator (Rita Medical Systems, Inc.) that produces up to 250 W of RF power, and it can be run in manual or automatic mode. Parameters such as generator output, tissue impedance, temperature, and time can be constantly monitored. The RF power setting defaults to 125 W, and this can be modified according to user experience and the thermal requirements of the individual tissue types. Specifically, for the left lateral segnentectomy, the power used was between 70 and 125 W. We must emphasize that lower power may be more effective in coagulating major vascular structures.
The laparoscopic Habib 4X (model LH4X) sealer.
Under general anesthesia, the patient was positioned in the supine position. A maximum central venous pressure value of 3 or 5 mm of H2O was maintained. Pneumoperitoneum was established with the introduction of a Veress needle. Insufflation pressure was maintained at the level of 10–12 mm Hg. Three trocars of 12 mm and one of 5 mm were placed along the subcostal margin. The two 12-mm ports were inserted to one side, and the rest were inserted from the other side. The Pringle maneuver was not applied. Perihepatic and peritoneal adhesions related to the previous laparotomy were divided to determine the entire peritoneal cavity for either local recurrence at the site of previous colorectal resection or for peritoneal deposits.
Initially, the left lobe of the liver and the whole peritoneal cavity were thoroughly inspected. Laparoscopic intraoperative ultrasound was applied in all cases in order to rule out possible undetected metastasis and also extension of the lesions beyond the resection line as the inspection alone could not define the actual extend of the liver tumor. The falciform ligament was divided by a Harmonic® scalpel (Ethicon Endo-Surgery, Blue Ash, OH). The intended transection line was marked on the liver surface using diathermy. Afterward, the left triangular ligament was divided.
The Habib 4X was then used to cause coagulative necrosis along the transection line. The coagulated parenchyma was then progressively transected after each RF application with laparoscopic scissors. The left portal vein branch of segment III was skeletonized and then divided (Fig. 2). Subsequently, the branch of segment II was identified and divided with an Endo GIA™ stapler (Covidien, Norwalk, CT) (Fig. 3). Finally, the specimen (Fig. 4) was extracted in an endobag via an enlarged 12-mm trocar site. A silicon drain was routinely placed along the resection margin (Fig. 5).
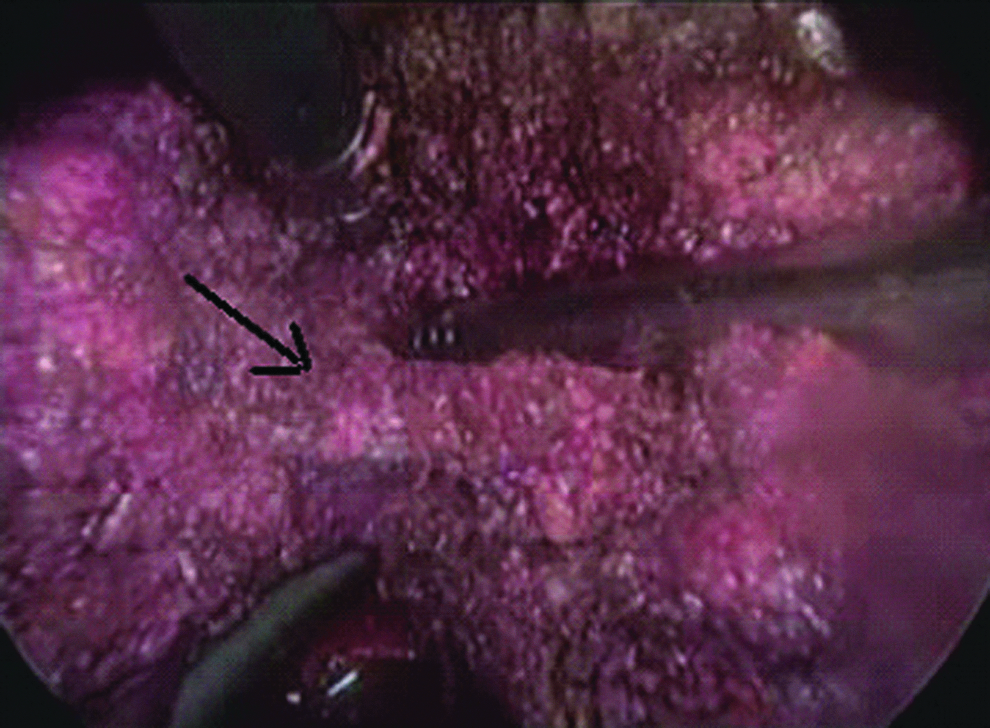
Intraoperative image. The black arrow indicates the left portal vein branch of segment III.

The branch of segment II (black arrow) was identified and divided with an Endo GIA stapler.
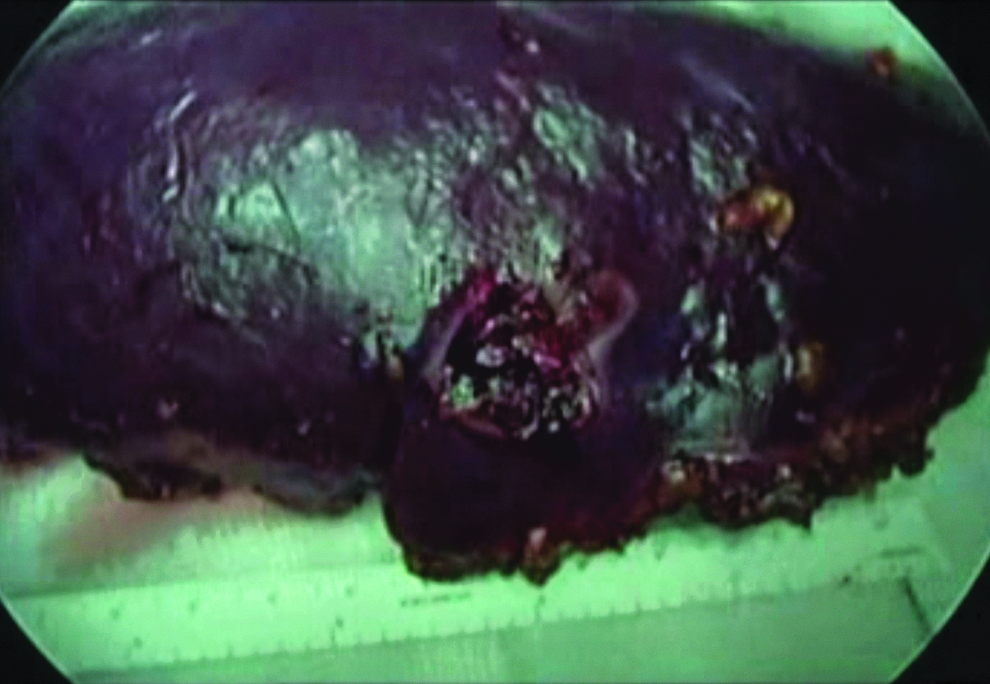
The resected specimen includes segments II and III.
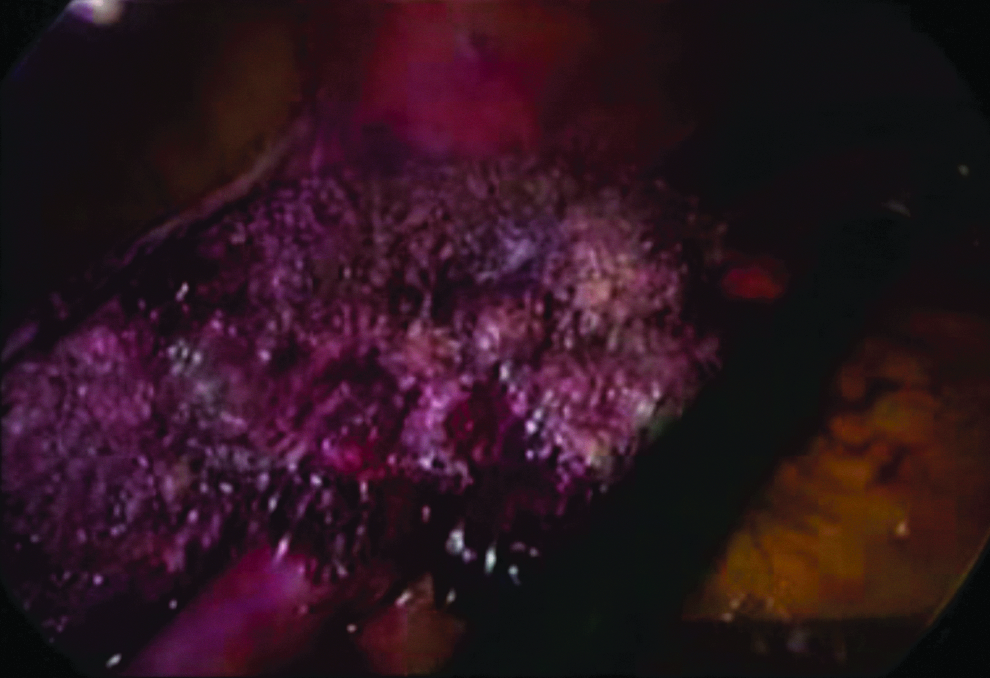
The cut surface after the resection using the laparoscopic Habib 4X (model LH4X) sealer.
Results
A formal laparoscopic left lateral sectionectomy was performed in all patients. Mean duration of the procedure was 75 minutes (range, 60–90 minutes). No conversion to laparotomy was required, as bleeding control along the transection line was totally satisfactory with the equipment used. Operative blood loss was minimal. Intraoperative transfusion of packed red blood cells was not required. All patients had good recovery. No postoperative complications occurred. No mortality was recorded. Median hospital stay was 3 days (range, 2–5 days). Histopathology revealed that the margins were disease free.
Discussion
Laparoscopic left lateral sectionectomy has been established in favor of laparoscopic liver surgery. The advantages over open surgery are the earlier improvement in serum transaminase levels, the reduced postoperative analgesic requirement, the shorter delay in oral intake, and the shorter hospital stay. 5 On the other hand, disadvantages remain: the technically challenging liver mobilization and retraction, the lack of tactile sensation, and the difficult tumor margin determination. In order to overcome these obstacles, laparoscopic surgery uses the advances of technological progress. 6
The resection was planned according to segmental vascular anatomy. The left portal vein has two portions: the transverse part, which is a short segment coursing through the porta hepatis, and the umbilical part. The latter descends into the umbilical fossa. At its end, the umbilical part is subdivided into a left branch (the oblique inferior branch), which supplies segment III, and the right branch (known as the oblique-upper branch), which supplies segment II.7,8 We could divide small vascular pedicles to the immediate left of the falciform ligament. In our patients, we could provide precise identification of these structures before division. Caution should be paid not to ligate the angle of the main branch of the left portal vein.
The actual challenge regarding laparoscopic liver resections is the ability to control an inadvertent bleeding. The ideal equipment for a safe laparoscopic liver resection would fulfill the prerequisites for minimal intraoperative bleeding along the transection line and decreased operative time with good results regarding mid-term complications such as bile leak. The Habib 4X is designed to be hemostatic without the need for inflow occlusion. Furthermore, coagulative necrosis caused by the Habib 4X before the actual transection of the parenchyma allowed meticulous and precise transection of the liver tissue along the plane desired and appeared effective in obliterating any vessels encountered. The minimal observed intraoperative blood loss and the virtual absence of postoperative complications in our patients demonstrate the favorable effects of the equipment used on the safety of laparoscopic liver resection. The successful completion of all liver resections laparoscopically, albeit promising, cannot stand as a definite conclusion about the usefulness of the device. Sufficient experience in both open and laparoscopic surgery is prerequisite for successful results in minimally invasive liver surgery.
As long as we had the facility in our departments to perform intraoperative ultrasound, which ensured intraoperative evaluation and definition of resectability and provided the previous experience in advanced laparoscopic and hepatic surgery, we could suggest that laparoscopic left lateral sectionectomy is the gold-standard technique, especially for solitary lesions. With the goal of increasing our experience, the next cases will be highly selected patients with solitary lesions located in anterior segments in order to define the resection criteria, especially for the RF technique.
Regarding technical issues, we avoided any unnecessary liver mobilization maneuvers. This certainly cannot be generalized as left lateral sectionectomy is by definition a procedure that does not usually require technically demanding division of liver attachments. However, our impression based on the observed effectiveness of the device is that performing laparoscopic liver resections with use of the Habib 4X can decrease the traditional time-consuming extensive mobilizations required for liver resections. According to our data, all procedures were completed successfully laparoscopically. The angles obtained for the introduction of the instrument inside the liver parenchyma from the certain port sites were adequate in all cases. However, in the 2 cases where the exact tumor margins were determined with intraoperative ultrasound, caution should be paid in the initial probe direction. After the RF application, data extracted from the ultrasonographic assessment would be inaccurate. When minor intraoperative bleeding was encountered, the use of simple cautery alone achieved adequate hemostasis.
However, a few things should be kept in mind before interpreting the results of the present study and seeking definite correspondence in clinical practice. Laparoscopic cancer surgery and especially liver resections require careful patient selection. 9 In the present study, highly selected patients as candidates for the main indication of laparoscopic liver resection (i.e., left lateral sectionectomy) participated. However, we consider such selectivity necessary taking into account the actual pilot nature of a newly introduced laparoscopic resection technique within the learning curve of two certified hepatopancreatobiliary surgeons. Additionally, all reports mention the incidence of postoperative complications without a distinctive approach due to the limited numbers of patients included in the study. Determining the incidence of complications was not the actual challenge in this study. Technical issues related with the real-time application of the technique were the primary end point.
In conclusion, laparoscopic liver resection with the use of the laparoscopic Habib 4X proved safe and efficient in the given patient sample. This technique may be an initial step for surgeons shifting to laparoscopic liver surgery provided previous experience in laparoscopic and liver surgery. Well-designed controlled randomized studies are needed in order to evaluate further the role of the device used in the present report in minimally invasive liver surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.