
Abstract
Abstract
Objectives:
Laparoendoscopic single-site surgery (LESS) in pediatric patients has emerged as a viable alternative to standard laparoscopy. The aim of our investigation was to assess different surgical approaches for LESS, stratifying by weight.
Subjects and Methods:
From March 2010 to April 2012 LESS was performed in 42 children. Children weighing below 10 kg underwent LESS through an umbilical incision using two 3-mm trocars and one 5-mm trocar. Patients above 10 kg were operated on using a metal multiuse single-site single port (X-Cone™; Karl Storz Endoskope, Tuttlingen, Germany). Conventional straight laparoscopic instruments were used in all cases.
Results:
Mean age at operation was 100 months (range, 0.25–207 months), and mean weight was 27 kg (range, 3.1–82 kg). Median operating time was 74 minutes (range, 36–300 minutes). Eighteen children underwent LESS using two 3-mm trocars and one 5-mm trocar; 1 case required two 5-mm trocars and one 10-mm trocar. Twenty-three patients were operated on with the multiuse device. All operations were carried out safely in a standard laparoscopic transperitoneal technique with full achievement of the surgical target. In none of the patients was an intraoperative complication noticed. Postoperatively two complications were noted, which resolved spontaneously.
Conclusions
: LESS for pediatric patients can be done safely and efficiently with even less trauma than in conventional laparoscopy irrespective of age and weight. However, different surgical approaches have to be considered as disposable single-site ports are not available for infants and small children. To decrease operative expenses, conventional multiuse trocars and a multiuse single-site port were used with conventional laparoscopic instruments.
Introduction
The aim of our investigation was to report our preliminary experience with two different surgical approaches for LESS in pediatric patients, stratified by age and weight. We used primarily straight conventional laparoscopic instruments and either standard trocars or a multiuse single-site port, avoiding the use of nondisposable instruments and devices.
Subjects and Methods
Between March 2010 and January 2012 42 children (17 girls and 25 boys) underwent LESS. Only three surgeons, all with advanced laparoscopic experience, operated on these patients. Institutional review board approval was obtained (protocol number 186/2010BO1), and all cases were prospectively entered into a database. Demographic data, type of procedure, operative time, intraoperative complications, technical problems, conversion, outcome, and cosmetic results were documented. Therefore surgeons were asked to fill out a detailed datasheet immediately following the procedure.
Patients were stratified according to their weight into two different groups. Children weighing below 10 kg underwent LESS through a periumbilical incision using three separate trocars, using the “Manhattan-technique” (Fig. 1). The majority of these children required one 5-mm trocar and two 3-mm trocars. One child required a 10-mm trocar and two 5-mm trocars. Patients above 10 kg were operated on using a metal multiuse single-site single port (X-Cone™; Karl Storz Endoskope, Tuttlingen, Germany) with different diameters for instruments ranging from 3 to 12.5 mm (Fig. 2).

Laparoendoscopic single-site surgery with one 5-mm trocar and two 3-mm trocars.
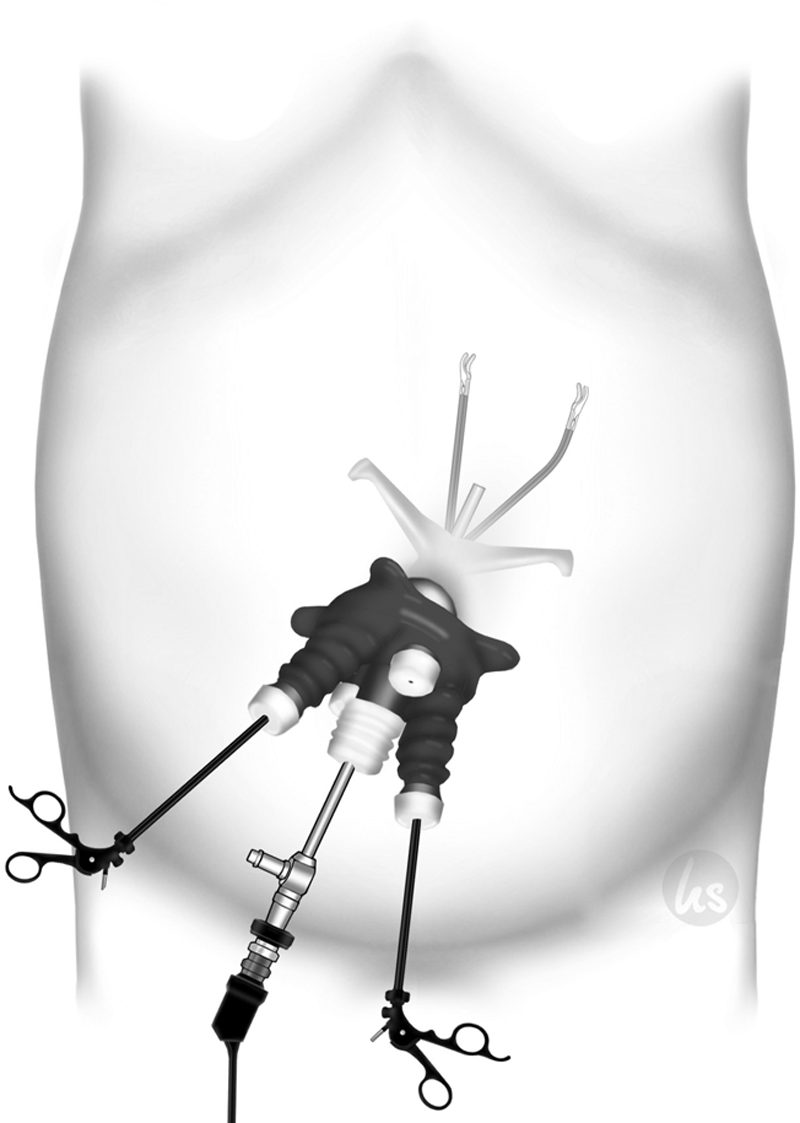
Laparoendoscopic single-site surgery with one multiuse single-site trocar (X-Cone).
The indications for surgery were appendicitis (n=11), cholecystolithiasis (n=6), ovarian processes (n=3), and cryptorchidism (n=3) as well as for nephrectomy (n=11) for nonfunctioning kidney. Three patients underwent partial nephroureterectomy (n=4) for nonfunctioning moieties in duplex systems; this was bilateral in 1 case. Other indications included varicocele (n=2), spherocytosis (n=1), and Meckel's diverticulum (n=2). In 2 patients undergoing cholecystectomy, the procedure was combined with a splenectomy.
Indication for nephroureterectomy was a nonfunctioning kidney due to vesicoureteral reflux in 8 cases, giant multicystic dysplasia with displacement of the abdominal contents to the contralateral side in 2 patients, and a rudimentary kidney without function in 1 case. For patients with a duplex kidney, the indication for undergoing partial nephrectomy was a nonfunctioning moiety. In all these patients kidney dysfunction was proved either by technetium-99m mercaptoacetyltriglycine renal scan or by dimercaptosuccinic acid renal scintigraphy. In children with duplex systems, diagnostic as well as functional evaluation was achieved with the use of dynamic magnetic resonance urography at 1.5 T using a navigator-triggered turbo fast low-angle shot sequence in order to provide split renal function and contrast medium excretion (Table 1).
According to the modified Dindo–Clavien classification of surgical complications. 1
F, female; M, male.
Surgical technique
With the patient positioned in the supine position, a small subumbilical incision was made along the lower half of the umbilical ring ranging between the 2 o'clock and the 10 o'clock position. In patients weighing below 10 kg, a 5-mm reusable trocar was placed under direct vision into the abdominal cavity, and pneumoperitoneum was established. A 5-mm 30° scope was inserted, and two 3-mm standard working ports were placed between the 2 and 10 o'clock positions, respectively, through separate fascial stab wounds. The trocars were placed at varying depths, using the “Manhattan-technique,” in order to minimize crowding of the trocars. Conventional 3-mm straight instruments were used. Two of the patients undergoing nephroureterectomy for giant multicystic dysplasia required cyst puncture and evacuation to provide the requisite working space for the remainder of the case. Other indications for children weighing below 10 kg included cryptorchidism, ovarian processes, and duplex kidney with a nonfunctioning moiety. In those patients the surgical technique was analogous as described above, also using straight instruments and hook electrocautery for tissue dissection (Fig. 1). In patients weighing more than 10 kg the incision was made along the lower half of the umbilical ring from the 3 o'clock to the 9 o'clock position. A metal multiuse single-site single port (X-Cone) was placed under direct vision in the abdominal cavity, the double half-cones of X-Cone were put together, and a silicon-rubber seal was placed on top of the external opening. Then pneumoperitoneum was achieved. The silicon-rubber seal offers five working channels, allowing the use of instruments with different diameters ranging from 3 to 12.5 mm. To avoid instrument clashing a Hopkins (Karl Storz Endoskope) forward-oblique telescope (30°; diameter, 5.5 mm; length, 50 cm) was used. One straight 5-mm instrument and one curved 5-mm grasper were inserted. Tissue dissection was performed using a Harmonic® (Ethicon, Blue Ash, OH) scalpel, sealing devices (Ligasure™; Covidien, Mansfield, MA), or hook or bipolar electrocautery. In resecting procedures, the specimens were retrieved through the X-Cone without further incision of the fascia. In splenectomies, all different techniques for dissection were uses as described above, in addition for one patient the splenic pedicle was dissected with an Endo GIA™ (Ethicon) stapling device, using one additional 12-mm disposable trocar (Ethicon) for insertion. In case of a Meckel's diverticulum, resection and consecutive end-to-end anastomosis of the bowel were performed ante situ through either the X-Cone or the umbilical incision (Fig. 2).
Results
Mean age at operation was 100 months (range, 0.25–207 months). Mean weight at operation was 27 kg (range, 3.1–82 kg). Median operating time was 74 minutes (range, 36–300 minutes). Eighteen children underwent LESS using two 3-mm trocars and one 5-mm trocar; 1 case required two 5-mm trocars and one 10-mm trocar. Twenty-three patients were operated on with the X-Cone. All operations were carried out in a standard laparoscopic transperitoneal technique. All procedures could be carried out safely with full achievement of the surgical target.
LESS could be completed in all children undergoing surgery without the need of conversion to conventional laparoscopy or open surgery. However, additional 5-mm trocars in standard laparoscopic positions had to be used in 2 cases of appendectomy and 1 case of a cholecystectomy. In 1 case of a combined cholecystectomy and splenectomy one single additional 12-mm disposable trocar for insertion of an Endo GIA stapling device was placed in order to provide proper vessel ligation of the splenic pedicle in a patient weighing 82 kg; the spleen specimen weighed 1,575 g. In another case of a varicocelectomy a conversion from the X-Cone to LESS with one 5-mm and two 3-mm trocars was necessary because of gas leakage and rigidity of the X-Cone, thus preventing proper ligation of the spermatic vessels. The procedure then could be continued without any further problems.
There were no intraoperative complications, and no children required blood transfusions. In one child who had undergone partial nephroureterectomy, renal artery spasm was noted in postoperative ultrasound leading to further diagnostic work-up, including computed tomography scan and angiography, which ruled out intimal dissection, thus being a Grade III complication according to the modified Dindo–Clavien classification of surgical complications. 1 The further course of the child was uneventful with full recovery of normal renal perfusion. In another child, a postoperative urinoma resolved spontaneously by postoperative Day 5, thus representing a Grade 1 complication according to the modified Dindo-Clavien classification of surgical complications. 1 Recovery was otherwise uneventful in the remaining children. The postoperative cosmesis was excellent in all cases.
Discussion
The advantages of laparoscopic surgery in pediatric patients have gained sufficient evidence in terms of efficacy and superior cosmesis combined with a decreased length of hospital stay in comparison with conventional open surgery.2–5 The aim to further reduce invasiveness of surgical approaches has led to the evolution of a variety of techniques such as single-incision laparoscopic surgery, single-incision pediatric endosurgery, LESS, or natural orifice translumenal endoscopic surgery (NOTES™; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society for American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) in trying to achieve the common goal of scarless surgery. The development of these surgical techniques would not have been possible without the synchronous advancements in the development of less invasive instrumentation for all aspects of endoscopic surgery. However, for different reasons, the adoption of LESS in pediatric patients has been slower and, like the application of laparoscopy and thoracoscopy in children in general, has historically lagged behind those in adult patients. 6 More recently, pediatric surgeons have been increasingly performing minimally invasive procedures through a single incision.7–14 Therefore specially designed ports and instruments have been designed to compensate for the disadvantages of working through a single incision and losing the advantage of triangulation of working instruments. However, these newly developed devices have been mainly used with the focus on adult patients. The result is that these devices are often too large, too long, or too thick for pediatric surgical purposes. In addition, a wide range of specialized instrumentation was also designed. Unfortunately, these instruments are also disposable, resulting in further increased costs for single-incision procedures easily exceeding $500 for one procedure. Finally, the surgeon has had to adapt to these new techniques using a variety of new devices, such as single-site ports, curved instruments, or bendable instruments.
With the aim for cost control for LESS in children, we decided to prospectively investigate the practicability and the limitations of the use of standard laparoscopic 3- and 5-mm trocars and instruments, respectively, and the use of a multiuse, single-site port to perform LESS for a variety of pediatric surgical and urological indications. In patients weighing below 10 kg we used conventional 3- and 5-mm instruments and trocars. For those newborn children or infants, 3-mm instruments seemed to be most appropriate as reticulating and curved instruments were only available in 5-mm diameter at that time. This enabled us to use the same instruments as in conventional laparoscopy. Similar cost considerations are supported by other authors 10 in small case series.
Well-established problems for the surgeon in LESS surgery are trocar crowding, instrument clashing, intra-abdominal exposure, and triangulation. Several case series of laparoscopic single-site procedures7,15,16 have demonstrated this. In our group of patients weighing below 10 kg, trocar crowding and instrument clashing occurred significantly less often compared with those patients operated on with the X-Cone. With the use of the X-Cone in patients weighing above 10 kg, we minimized instrument clashing by using a long telescope 50 cm in length in order to move the camera head out of range of the instrument handles and thus out of the range of the surgeon's hands. The use of transabdominal traction sutures to expose or to stabilize the surgical site also compensated for the limited number of working ports. A major problem while using the X-Cone was gas leakage due to insufficient sealing of the silicon-rubber seal placed on top of the external opening. With tearing at the cap secondary to instrument movement, gas leakage worsened throughout the course of an operation. The application of a sterile lubricant decreased the friction and reduced the resistance of the instrument's movement through the rubber cap, resulting in less tearing of the seal. With the X-Cone we were able to use standard laparoscopic instruments for dissection and preparation, for ligation with clips, a vessel-sealing device, or the Harmonic scalpel. A curved or bent instrument in selected cases aided exposure and triangulation. In a recently published report on using the X-Cone in a porcine model 17 similar experiences could be documented. With the use of one straight instrument and one curved grasper, the best mean score for subjective parameters such as triangulation, different dissection directions, and retraction could be obtained. This supports our experience in pediatric patients. It is interesting that the authors also reported the problem of significant gas leakage in 58% of their cases. 17
The operating time in our series was a median of 74 minutes (range, 36–300 minutes) and therefore competitive compared with other studies applying LESS to pediatric patients.15,18–20 However, operating times exceeded up to 300 minutes in 1 case of nephrectomy, which is considered to be significantly longer than in conventional laparoscopy as recently published in a own series of 23 cases. 4 Other authors documented rather longer operating times with a mean of 192.2 minutes for LESS, 219.3 minutes for conventional laparoscopy, and even 127.4 minutes for open nephrectomy in children 21 and a mean of 139 minutes in another study. 20 That might also reflect the learning curve for LESS in children even for rather experienced surgeons who are familiar with laparoscopic procedures; however, for adults another study 22 could not prove any difference in terms of operating time between the two approaches.
In centers with major experience for LESS in children and for standard procedures such as appendectomy, very competitive operating times with a median of 40 minutes have already been published.16,23 For cholecystectomy other authors recently published their preliminary experiences7,24–26 and noted it was safe and feasible. However, similar to our patients, additional trocars were infrequently necessary to accomplish the procedure. This clearly reflects the surgeons' needs for exposure and triangulation during LESS procedures, which may be difficult in individual cases 27 irrespective of the trocar technique used for LESS. The one major task for applying LESS is cosmesis and “scarless surgery,” when the surgical scar can be concealed in our natural scar, the umbilicus. This does not necessarily mean the use of just one single-site trocar system as the access using multiple working ports through a single umbilical incision also offers superior cosmetic results compared with multiple scars due to stab incisions for conventional laparoscopy. However, because of the commitment to evidence-based medicine it will be important to scientifically evaluate, whether those demands for a “scarless surgery” justify longer operating times, technical difficulties, and increased costs but, on the other hand, offer significant benefit for the patient. 28
In conclusion, LESS can be performed safely and efficiently in a pediatric patient population irrespective of age and weight. The cosmesis is superior to conventional laparoscopy with the surgical scar concealed in the umbilicus. However, different surgical approaches have to be considered when patients are stratified for age and weight because single-site ports are not available for small children and infants. We preferred to use conventional multiuse trocars or a multiuse single-site single port, mainly for economic reasons. Those techniques offered the advantage of LESS combined with the use of a familiar instrumentation, thus allowing the surgeon to rather quickly overcome the drawbacks of LESS, such as fewer degrees of freedom, in-line view of the endoscope, and clashing of instruments. However, both trocars and instrumentation will benefit from future technical development of instruments and trocars more suitable for small children. The learning curve for LESS offers an increase in the surgeon's technical skills, which is appreciated and potentially of value for a variety of endoscopic procedures, whether single incision or standard. Our article also seeks to urge the challenge of future education and training in LESS but also the need for further prospective evaluation of single-site laparoscopic surgery.
Footnotes
Acknowledgments
Illustrations were provided by Hannes Schramm, Photography and Graphics, University of Tuebingen.
Disclosure Statement
No competing financial interests exist.