
Abstract
Abstract
Background:
Single-incision pediatric endosurgery (SIPES) is defined as minimally invasive surgery performed through a unique incision in the abdomen, chest, or retroperitoneum. Several publications exist, but no previous systematic review has been made to evaluate the real benefits of this approach in terms of feasibility and clinical outcomes.
Materials and Methods:
We performed an electronic search in PubMed up to March 2012 with the terms “single AND incision OR site OR port OR trocar AND children” including related articles and obtained 197 articles. After applying our inclusion criteria, 78 articles were reviewed.
Results:
We identified prospective controlled trials (n=1), case-control studies (n=12), case series (n=49), and case reports (n=16). In total, 4212 patients had been operated on by SIPES and were separated by systems: gastrointestinal (n=2888), urologic (n=390), gynecologic (n=27), other abdominal (n=874), and thoracic (n=33) procedures. The most common procedure was SIPES appendectomy, and a unique prospective controlled trial supports its safety and effectiveness. Technically demanding surgeries such as hepatojejunostomy and colonic surgeries were described. Multichannel ports and multiple ports, standard and articulated instruments, transparietal instruments, retraction sutures, and magnets were used. Operative times, length of stay, and complications similar to standard laparoscopic surgery were described. A low conversion rate (to a reduced port, standard laparoscopy and open procedures) was also mentioned. No comparable measure for pain and cosmesis assessment was used.
Conclusions:
A wide experience in SIPES and feasibility has already been described with good clinical outcomes and low rate of conversion. Appendectomy is the unique procedure in which SIPES has been demonstrated to be safe and effective. It is pending the execution of prospective controlled trials for other operations to demonstrate, with objective evidence, the real benefits of this less invasive approach.
Introduction
In the search for less invasive procedures, ever since the development of laparoscopic surgery and with the limitations and equipment dependence of Natural Orifice Translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]), this new approach through the umbilicus, a natural embrionary orifice, 1 was first reported in 1992 by Pelosi and Pelosi. 2 Quickly, the literature showed that SIES was a feasible and excellent cosmetic procedure pending the demonstration of its clinical and economic benefits with objective evidence. In 1998, the first SIES appendectomy was described in children. 3 At present, several other single-incision pediatric endosurgery (SIPES) procedures have been reported (Table 1).
Controversies in SIPES have been stated because many of the basic principles of general and laparoscopic surgery may not be fulfilled, especially in terms of triangulation.4,5 It is not well known if the safety of the procedure may be affected, creating longer operative times and more complications.
Published data about SIPES include case reports, case series, comparative retrospective studies, and one prospective randomized controlled trial for SIPES. 6 No systematic review has been previously published for SIPES, and we believe surgeons performing minimally invasive surgery might choose their operative technique based on objective evidence. The objective of this review is to show the initial published experience about SIPES to evaluate its real benefits in terms of feasibility and clinical outcomes.
Materials and Methods
We performed a systematic review of the literature to find out the current state of SIPES procedures, including age, technical aspects, and operative outcomes. An electronic search in PubMed up to March 2012 was conducted with the following terms: “single” AND “incision” OR “site” OR “port” OR “trocar” AND “children.” Related articles were also reviewed.
Articles were considered eligible if they met the following inclusion criteria: (1) Operations were performed through a single incision. (2) The target population was children under 18 years of age. (3) Operations performed exclusively by pediatric surgeons. (4) Series larger than 100 patients were included for appendectomy operations. (5) Case reports, case series, and comparative and prospective randomized trials were included in other, nonappendectomy, operations because of their low incidence. (6) Articles should include age, operative technical aspects, and operative outcomes.
As appendectomy is a very common procedure and several short case series had been reported initially, we had just selected series larger than 100 cases. Smaller appendectomy series, continuation series, review articles, abstracts only, experts opinions articles, editorial, letters to the editor, and unpublished series were excluded.
The quality of the reviewed articles was evaluated by one of the authors. Articles were classified according to types of operations, levels of evidence, and age groups:
• Types of operations were classified by systems: gastrointestinal, urologic, gynecologic, other abdominal, and thoracic. • We used the original classification of levels of evidence described by the Canadian Task Force on the Periodic Health Examination.
7
• We classified into four age groups: newborns (0–28 days), infants and toddlers (1–23 months), children (2–11 years), and adolescents (12–18 years).
Data extracted from these articles were further analyzed for (1) technical aspects (port and instrumentation type) and (2) operative outcomes (operative time, conversion rate, length of stay, pain assessment, and complications).
Ports were defined as the access device chosen to perform the single-incision surgery. In pediatrics, these include multilumen devices such as the SILS™ Port (Covidien, Inc., Mansfield, MA) or the TriPort (Advanced Surgical Concepts, Bray, Ireland, United Kingdom) or the use of multiple cannulas or the combination of one-cannula and stab fascial incisions for passage of the instruments through a single skin incision.
Instrumentation included the use of standard, articulated, or curved graspers, dissectors, scissors, or any other required device.
Operative time was described as a median or medium (in minutes) and range when mentioned.
Conversion was defined as the necessity to put in one or more additional ports or stab incisions for passage of instruments away from the main skin incision or to change to an open operation.
Length of stay was described in terms of days and range when mentioned.
Pain assessment was evaluated in terms of the use of a visual analog scale (1–10) or the analgesic requirement if mentioned.
Results
After the PubMed search we identified 197 articles. After applying our eligibility criteria, we selected 78 articles6–83 to be included in this systematic review (Fig. 1).
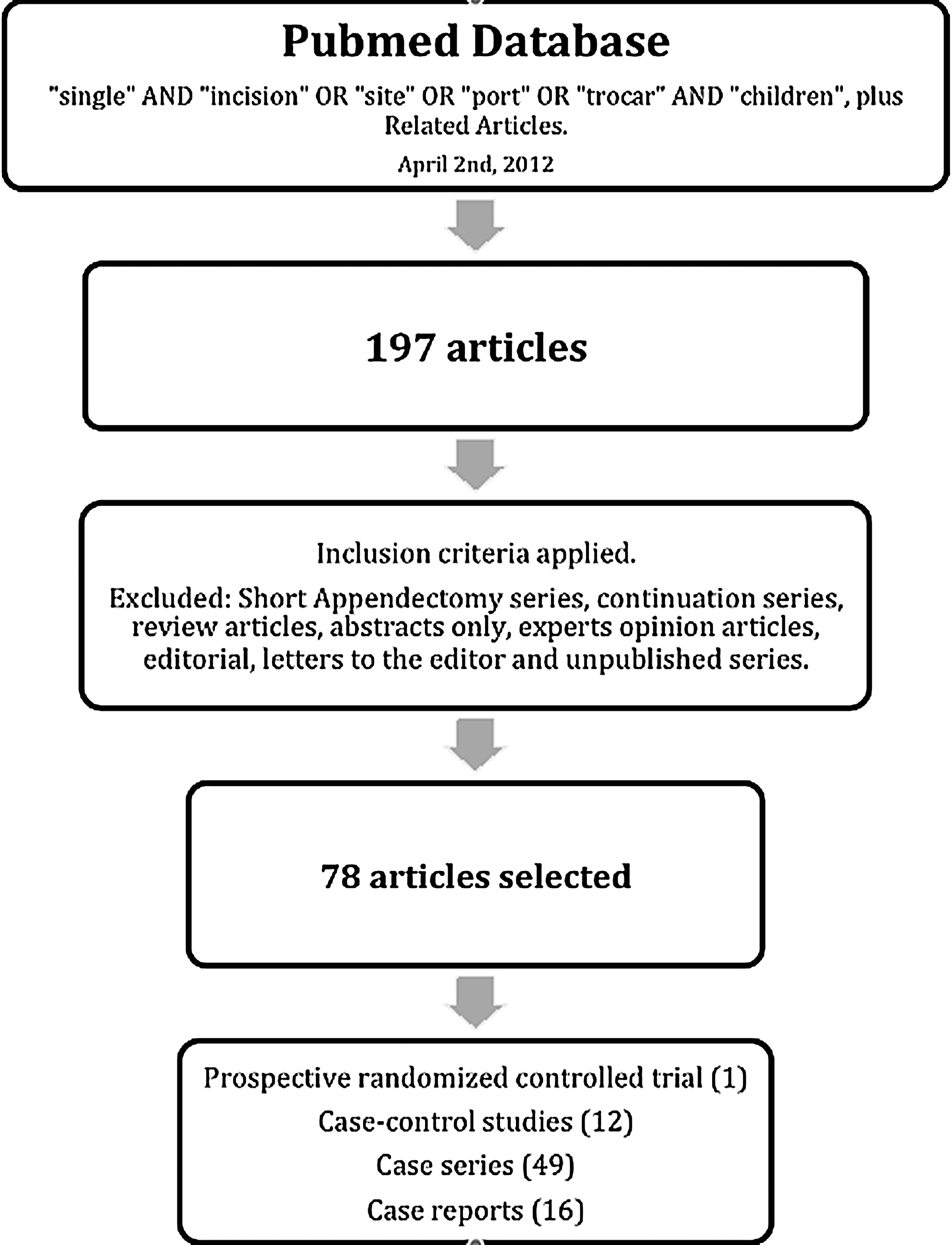
Flowchart showing the literature search strategy followed by the authors.
We identified a total of 4212 patients operated on by SIPES. We separated types of operations by systems: gastrointestinal (n=2888 patients), urological (n=390 patients), gynecological (n=27 patients), other abdominal (n=874 patients), and thoracic (n=33 patients) procedures (Table 1).
According to evidence level we had 1 prospective randomized controlled trial, 12 case-control studies, 49 case series, and 16 case reports (Table 2).
In the newborn period SIPES pyloromyotomy, endorectal pullthrough, ovarian cystectomy, and ventriculoperitoneal shunt were performed, with the youngest patients being 1 day old. The majority of operations were performed in the “children” and “adolescents” group. Distribution by age can be seen in Table 3.
Gastrointestinal SIPES
Appendectomy
Twelve articles fulfilled our inclusion criteria for SIPES appendectomy, including a total of 2422 patients.6,8–18 One prospective randomized trial had been published describing longer operative times, same time to oral intake and discharge, more analgesics requirements, same infectious complications, no difference in hospital charges, and no difference in time to full activity and returning to school with the SIPES approach in comparison with the three-port laparoscopic approach. 6 The majority of publications were case series, and results are compared with conventional laparoscopy.
The initial reports consisted of extracorporeal appendectomies (laparoscopic-assisted procedures). However, fully laparoscopic SIPES appendectomies without any requirement of special flexible or articulated instruments had been reported as well.11,14 Good results were described in acute, perforated, and residual appendicitis.8,11,12,16–18 The details of the operations are described in Table 4.
A, acute; C, complicated; I, interval; O, others.
EC, extracorporeal; IC, intracorporeal.
LOS, length of stay; NS, not specified.
Cholecystectomy
Eleven articles that fulfilled the inclusion criteria were considered in this review, and they included 232 patients.19–28 Technical aspects and operative outcomes are described in Table 5. These articles included three case-control studies, seven case series, and one case report (evidence level III and IV).
AR, analgesic requirement; BL, bilateral; GERD, gastroesophageal reflux disease; LPEC, laparoscopic percutaneous extraperitoneal closure; LOS, length of stay; MChP, multichannel port; NS, not specified; UL, unilateral; VPS, visual pain score.
Adolescents were the main age group in whom SIPES cholecystectomy was performed. The youngest patient was a 4-month-old infant reported by Ergün et al. 22
Multichannel ports and multiple ports had been used by the different authors. Most of them described the use of standard and articulated graspers and the passage of transparietal sutures to achieve an adequate triangulation and insure that the critical view of safety was well visualized. One report mentioned the use of magnets for retraction. 5 Some authors had been adding an additional transparietal minilaparoscopic grasper (through a stab incision). 9 Some procedures included an intraoperative cholangiography, which increased the operative time. The conversion rate was 11.2%. Wound infections were described as the unique complication (1.3%).
Splenic surgery
Seven articles of SIPES splenic procedures were included with 26 patients: pure splenectomy in 12 cases,5,21,22,27,30,31 combined splenectomy and cholecystectomy in 8 cases,5,21,27,29,30 splenic cystectomy in 5 cases,22,30 and splenopexy in 1 case. 30 These articles were six case series and one case report (evidence level IV).
The use of multichannel ports and multiple individual ports and standard, curved, and articulated graspers had been described. Incision length ranged from 2 to 2.5 cm, and this larger incision facilitated the extraction of the spleen. There were four conversions (15.4%). Other clinical outcomes are described in Table 5.
Hepaticojejunostomy
Nineteen cases of hepaticojejunostomy for choledocal cysts were included in one publication, using multiple individual ports through the umbilicus, straight standard instruments, extralong telescopes, and suture retractions, performing an intracorporeal hepatojejunostomy and an extracorporeal end-to-side enterostomy, with postoperative recovery, duration of drainage, low conversion rate (2 cases [10.5%]), and one complication (bile leak [5.3%]), similar to conventional laparoscopic hepaticojejunostomy (evidence level III). 32
Liver biopsy
Five liver biopsies were reported in one publication. 10
Pyloromyotomy
Two series fulfilled our inclusion criteria for SIPES pyloromyotomy, including a total of 64 patients.33,34 Both of the studies were comparative studies (evidence level III), signaling this approach as a reasonable alternative to standard laparoscopy with an extremely high parent satisfaction because of its improved cosmesis. Both series described the use of multiple individual ports through the umbilicus and standard minilaparoscopic instruments. Nevertheless, two mucosal perforations (3.8%) and one wound infection (1.9%) were reported in one of the series. 34 Three conversions were described (4.7%). 34
Nissen fundoplication
In total, 11 cases of SIPES Nissen fundoplication for gastroesophageal reflux disease were described in two publications (evidence level IV).5,35 Four of them had also an associated gastrostomy tube placement. Operative difficulty was described with the suturing technique. Three conversions (27.3%) and one gastroesophageal reflux disease recurrence (20%) were reported.
Heller myotomy
One SIPES Heller myotomy and Dor fundoplication was reported with complete resolution of dysphagia and regurgitation, no complications, and an excellent cosmetic result. 36
Gastrotomy tube placement
Three series and a total of 34 patients had SIPES gastrostomy tube placement.37–39 The first and longest series included 22 patients and was published in 2006. 39 All of the cases used an operative scope (optical grasper) in the site were the gastrostomy tube remained. No conversions were reported. Wound infections were reported in one series (16%).
Duodenal web resection
One duodenal web resection by SIPES was reported with the use of a multichannel port and endostapler, an operative time of 209 minutes, and no complications. 40
Jejunoileal surgery
Three series described a total of 23 SIPES jejunoileal resections and Meckel diverticulectomies (evidence level IV).10,21,41 In addition, 6 cases of SIPES adhesiolysis and 7 cases of intestinal biopsies (jejunoileal/colonic) were also described. 10 All of these procedures were completed extracorporeally with no need for conversion.
Ileocecetomy
In total, 10 SIPES ileocecetomies for Crohn's disease were described in three publications (evidence level IV).21,42,43 All of them described an extracorporeal anastomosis with no conversion.
Colonic surgery
One article reported 10 patients in whom colonic procedures for inflammatory bowel disease and polyposis syndromes were performed: three total colectomies and eight ileal-pouch anal anastomoses with and without ileostomy. 43
Multichannel ports, a “glove port,” and multiple individual ports were used in SIPES bowel surgery, and all of them used standard straight instruments and an extracorporeal anastomosis. Complications included two anastomotic leaks in patients without a protective ileostomy (20%), one small bowel obstruction (10%), and one pelvic abscess (10%).
Another article reported a total abdominal colectomy with the use of magnets and no complications. 25
An additional port was added for better maneuverability in 7 cases (63.6%).
Endorectal pullthrough
One report of 6 cases of SIPES endorectal pullthrough for Hirschsprung's disease was included with the use of standard instruments and no conversions or complications. 44
Urologic SIPES
In total, 390 SIPES procedures, both laparoscopic and retroperitoneoscopic, have been reported: 212 varicocelectomies,10,22,50,62 109 pyeloplasties,10,57–59 52 nephrectomies,45–56 6 gonadectomies,22,50,66 5 orchiopexies,63–65 4 renal biopsies, 1 renal cyst decortication, and 1 urinoma drainage. 10 Four comparative studies were included: three for SIPES nephrectomies and one for pyeloplasties (evidence level III). Other articles were case series (evidence level IV).
Gynecologic SIPES
A total of four articles fulfilled our inclusion criteria for SIPES gynecologic procedures (evidence level IV) including 27 patients: 19 ovarian cystectomies,5,22,67–69 6 oophorectomies, and 2 ovarian teratoma excisions.22,67 The use of multichannel ports and operative scopes with standard and articulated graspers and good operative outcomes were described.
Other abdominal procedures
One retroperitoneal lymphangioma resection was reported with the aid of magnets. 5 A Morgagni diaphragmatic hernia repair had been reported without complications. 70
Nine articles fulfilled our inclusion criteria for SIPES inguinal hernia repair including 835 patients, in whom a percutaneous needle completed the procedures at the internal ring level.71–79 Complications reports included recurrences (2.7%), hydroceles (1.3%), and suture granulomas (1.2%).
Two SIPES series related to ventriculoperitoneal shunts for hydrocephalia included 10 patients.80,81 Two SIPES series related to insertion or revision of a peritoneal dialysis catheter included 27 patients.10,82
All of these articles were case series and have an evidence level of IV.
Thoracic SIPES
Two articles fulfilled our inclusion criteria for SIPES thoracoscopic procedures, including 20 empyema drainage procedures,10,83 10 lung resections, 1 mediastinal biopsy, 1 chest wall biopsy, and 1 neuroblastoma resection. 83 One of the articles was a comparative study with conventional video-assisted thoracoscopic surgery (VATS) having an evidence level of III and supporting SIPES to be as safe and efficient as VATS and that should be performed by pediatric surgeons with expertise in VATS. 83 No differences were found in the chest drain removal or hospital length of stay. A clear esthetic advantage was described because the incision is where the chest drain was left. No conversions were reported.
Discussion
SIES is defined as minimally invasive surgery performed through a unique incision in the abdomen, chest, or retroperitoneum, as has been reviewed. Several terminologies have been used to describe this approach; however, our preference in children is to use SIPES, described by Muensterer and co-workers9,34,35,40,42,44,72,84 as a broad term that includes laparoscopy, thoracoscopy, retroperitoneoscopy, or other, performed through one single incision in children. The potential advantages of SIPES are less trauma, fewer port site-related complications, reduced pain, shorter length of hospital stay, and improved cosmesis (one scar in a natural location).
Having reviewed the technical aspects of SIPES procedures and the clinical outcomes by systems, we are able to state some features about this approach.
In terms of instrumentation, special devices have been designed to allow the passage of different instruments through a single incision and include multichannel port devices, flexible-tip scopes, and articulated or curved graspers, dissectors, and scissors. 4 It has been shown in the literature that these “specialized” devices are not necessary to perform most SIPES operations in children. Multiple individual ports through a single incision provide acceptable exposure and excellent cosmetic results and mean no additional cost. Furthermore, the use of extra-long telescopes and low-profile cannulas through a single incision provides superior hand maneuverability, avoiding clashing of instruments. The use of stab incisions and transparietal sutures for retracting structures allows adequate exposure as well, and these are easily placed in children because of their thin abdominal wall. Magnets have recently been described to provide adequate exposure as well. 5
Most of the reports show operating times, lengths of stay, and rate of infectious complications comparable to those with traditional laparoscopy, with a low rate of conversion.
There is no consensus about the definition of “conversion” among authors in the literature. We had defined it as the need to use one or more additional ports to complete the procedure or to change to an open procedure. However, the conversion from a single-port to a reduced-port procedure may be considered a “modified” or “hybrid” SIPES procedure for some authors.
In terms of pain, it is believed that a larger umbilical incision may translate into more postoperative pain. However, others have speculated that limiting the number of incisions means decreasing trauma to the tissue and translates into reduced pain. Unfortunately, we did not find a uniform pain assessment among authors, and others did not even mention it.
Finally, the esthetic assessment has not objectively been described and remains just as a “improved cosmesis” subjective appraisal by the surgeon.
Gastrointestinal SIPES
Appendectomy
Appendectomy is the most common SIPES procedure. Pelosi and Pelosi 2 reported the first SIES appendectomy in adults in 1992. A French report by Begin 85 described the first SIPES appendectomy in children published in a French journal in 1993, and Esposito 3 reported the first SIPES cases found in PubMed in 1998.
This technique was originally described using an operative laparoscope to exteriorize the appendix through the umbilicus and perform an extracorporeal appendectomy. Others used conventional cannulas to exteriorize the appendix. This may be unique to children because the thin abdominal wall and the shorter distance from the cecum to the umbilicus allow for the appendix to be easily exteriorized. 86 Lee et al. 11 and Agkür et al. 14 reported the intracorporeal technique, as well as other short series.87,88
We understand that there is a preference among SIPES surgeons to operate on acute noncomplicated appendicitis; however, with the increasing experience, some complicated cases are performed without the necessity of an additional port or to convert to a conventional laparoscopy or to an open approach.8,11,12,16–18
The mean operative time was longer with the SIPES approach in the prospective trial of St Peter et al., 6 where a 10% conversion rate was described, a value similar to our 10.7% conversion rate found in this review (Table 5).
In terms of pain, Chandler and Danielson 89 reported an overall decrease in intravenous narcotics after SIPES appendectomy compared with conventional laparoscopic appendectomy in a large study on 110 children. A prospective study of 39 patients by Mayer et al. 90 demonstrated that SIPES appendectomies did not translate into increased postoperative pain and reduced the amount of postoperative analgesics. However, St Peter et al. 6 found that more doses of analgesia were given in the SIPES patients during their hospital stay but not during convalescence. In our review we did not identify a comparable pain assessment method. Three of the publications evaluated pain in terms of analgesic requirement and showed minimal dose requirements, and the other eight publications do not mention anything about it.
Initial reports showed great concern about the increasing risk of wound infections in SIPES appendectomy. However, the wound infection rate decreased with time as soon as greater experience had been achieved, and nowadays it has been demonstrated that the wound infection rate (2.3% in our findings) is not different from that of conventional laparoscopic appendectomies. Additionally, there was no difference in infectious complications found in the prospective trial of St Peter et al. 6
One last concern is that the larger umbilical incision could theoretically increase the risk of postoperative hernias; however, this has not been detected in the follow-up of the prospective trial mentioned and also is not described in any of the publications reviewed.
Thus, in summary, for SIPES appendectomies there exists evidence of feasibility for acute and complicated cases, longer operative times in some cases, equal global analgesic requirement, and equal rate of infectious complications compared with conventional laparoscopic appendectomies. Therefore, as appendicitis is a relatively frequent pathology, we encourage experienced laparoscopic surgeons to perform this almost scarless surgery in children.
Cholecystectomy
Cholecystectomy is the second most common SIPES gastrointestinal procedure performed in children. In 1997Navarra 91 performed the first SIES cholecystectomy. 92 The first published data about SIPES cholecystectomy belong to Dutta 27 and Ponsky et al. 28 in 2009.
A significant number of cases needed an additional instrument or port to visualize the critical view of safety with a conversion rate of 11.2%. Good outcomes with low rates of infectious complications (1.3% in our findings) are reported using this technique; however, the lack of prospective controlled trials suggests that these procedures are feasible and safe but with no objective evidence of it yet.
Splenic surgery
In 2009, Dutta et al. 27 reported their experience with SIPES splenectomy in 6 cases, 2 of them with associated cholecystectomy. Six reports of SIPES splenectomy exist in the literature. Additionally, there are five reports of simultaneous cholecystectomy and splenectomy.
Cosmetic advantages of SIPES splenectomy are self-evident, resulting in the absence of any visible scar. The benefits in other clinical outcomes, such as pain and hospitalization, are still nebulous because this technique is still evolving, and few reports exist even in the adult population.94,95 However, operative times, blood loss, conversion rate, and length of stay seem to be similar to those of traditional laparoscopic splenectomy.
Pyloromyotomy
Muensterer et al. 84 reported the first series of SIPES pyloromyotomy without the necessity of special ports or instruments. A posterior series included a comparison study of 52 babies in whom SIPES was performed with two different techniques by the same research group. 34 Gastric mucosal perforations occurred in 3.2% of the cases, and 4.7% of the cases were converted to a three-port laparoscopy or open surgery. These studies suggest that SIPES pyloromyotomy is feasible, but the demonstration of its safeness is still pending because of the high perforation rate reported.
Hepaticojejunostomy
A single comparative study reported that SIPES hepaticojejunostomy for choledocal cyst is feasible in experienced hands. 32 This is considered a technically demanding surgery and shows that complex surgeries can also be performed through a single incision in children.
Bowel surgeries
SIPES jejunoileal resection, Meckel diverticulectomy, and ileocecectomy have been described with the use of longer incisions, which allow for exteriorization, resection, and anastomosis of the bowel segment with short operative times, excellent cosmesis, no conversions, and no complications.10,21,41
Padilla et al. 5 and Potter et al. 43 described SIPES colectomies and ileal-pouch anal anastomosis with and without ileostomy in two reports (11 patients), with operative times, length of hospital stay, and functional outcomes similar to those of open, laparoscopic-assisted, and laparoscopic colonic surgery in children. An additional port was added for better maneuverability in 63.6% of the cases. However, a 50% rate of complications is described in one of the reports, 43 including anastomotic leaks (20%), bowel obstruction (10%), pelvic abscess (10%), and portal vein thrombosis (10%).
A single report described SIPES endorectal pullthrough. Although the procedure is technically challenging, infants with Hirschsprung's disease can be operated on by SIPES safely with good postoperative results, excellent cosmesis, and no conversion or complications. 44
We just have little and weak evidence about advantages of SIPES in bowel surgeries because these entities are not very frequent in pediatrics, and it might be difficult to perform a prospective trial to evaluate their real outcomes. However, it is suggested that significant rates of conversion and postoperative complications exist with colectomies, thus discouraging surgeons from performing SIPES in colonic diseases.
Urologic SIPES
In the last decade, indications for urologic endosurgery in children have been expanded, and SIPES partial and total nephrectomies, nephroureterectomies, pyeloplasties, varicocelectomies, orchiopexies, and gonadectomies have been reported.
Varicocelectomy
Varicocelectomies are the most common urologic procedure performed by SIPES. Kaouk and Palmer 62 reported the first SIPES varicocelectomies. Three other series have been described with good results.10,20,49 Multichannel ports and operative scopes, with standard and articulated graspers, are used by authors in the literature. Comparable operating times, length of stay, and complications to those of traditional laparoscopy and a conversion rate of 9.9% are described.
Pyeloplasty
Pyeloplasty is the second most common urologic SIPES procedure. In general, standard and SIPES laparoscopic, transperitoneal and retroperitoneal, and robotic pyeloplasties have been reported.
In 2007, Lima et al. 60 described a “one trocar assisted pyeloplasty,” consisting of a retroperitoneoscopic technique in which the ureteropelvic junction was dissected and exteriorized and a manual extracorporeal anastomosis was performed. Later on, several authors reported their experience as a safe and effective technique, specially in very small children, including a comparative study with open pyeloplasty.10,57,58
The use of a multichannel port with articulated graspers for a fully laparoscopic procedure or the use of operative scopes with standard instruments for an extracorporeal anastomosis is described with a conversion rate of 7.3% and similar complications to those with the traditional laparoscopic approach.
Nephrectomy
Rane and Rao 96 described the first SIES nephrectomy in 2008 in adults. Park et al. 97 and Johnson et al. 56 in 2009 and Wong et al. 98 in 2010 reported the first cases of SIPES nephrectomies. Kim et al. 45 reported the largest series with 11 cases in a comparative study.
The use of multichannel ports, “glove ports,” and multiple individual ports, with standard and articulated graspers, is described with a low conversion rate of 2.9% and a unique complication of retroperitoneal fluid collection (1.9%), showing that this is a safe and feasible procedure for children.
Gynecologic SIPES
Ovarian cystectomy is the most common SIPES procedure reported and has been performed in patients between 1 day of life and 17 years old. Prospective studies are required to demonstrate SIPES benefits in pediatric gynecology.
Other abdominal SIPES procedures
A retroperitoneal lymphangioma resection, a Morgagni diaphragmatic hernia repair, inguinal hernia repairs, ventriculoperitoneal shunt placement or revision, and peritoneal dialysis catheter insertion or revision have been reported by SIPES. This indicates the variety of surgeries that can be performed by SIPES, showing good functional and cosmetic outcomes.
Several techniques have been described for laparoscopic inguinal hernia repair. Advantages include the possibility of evaluation of the contralateral side and avoidance of trauma to the vas deferens and spermatic vessels. A hybrid technique with the “laparoscopic percutaneous extraperitoneal closure” was introduced by Takehara et al. 99 for inguinal hernia in children, as a simpler method with a low recurrence rate. Several series reported their cases even before the development of the concept of “single-incision laparoscopic surgery.” One or two individual ports in the umbilicus with the aid of a laparoscopic percutaneous extraperitoneal closure or large round needle are reported to close the inguinal internal ring. A recurrence rate of 2.7% is found between the reports. We believe that a prospective trial about SIPES inguinal hernia repair can be accomplished, because of the high incidence, to evaluate the security and benefits of this procedure.
Thoracic SIPES
SIPES thoracoscopy has also been described with comparable results to those of VATS in terms of equal operative time, length of stay, and better cosmesis.10,83 The most frequent procedure reported is empyema drainage. SIPES might be a safe and effective option for experienced VATS surgeons to treat certain thoracic diseases. There are no prospective studies to confirm these findings.
Conclusions
In summary, we have made a systematic search of all the SIPES procedures reported in the literature, under our inclusion criteria, finding no objective evidence in clinical outcomes, except for appendectomies.
Further analysis could not be performed because of the weak nature of the evidence in the majority of publications and some methodological defects of the literature reviewed. The low incidence of some pediatric surgical diseases (favoring case series with low level of evidence) and the lack of uniformity in evaluating some measures among surgeons, like pain assessment or cosmesis, for example, are the main contributors to this limitation.
Finally, it is suggested that performing pediatric endosurgery through multiple incisions for small cannulas and/or stab incisions (initially described by Ostlie and Holcomb, 100 noted by Rothenberg et al. 101 ), so-called “minilaparoscopy,” 102 “reduced port” surgery, or “hydrid surgery” in adults, 103 provides a safe and feasible surgery in children, resulting in minimal trauma and scars.
From this systematic review we conclude:
• A wide experience in SIPES and its feasibility have already been described with good clinical outcomes and low rate of conversion. • The majority of the SIPES procedures were performed in the “children” and “adolescents” groups. • Appendectomy is the unique procedure in which SIPES has demonstrated to be safe and effective. • Some SIPES procedures can be performed with the same standard instruments of a conventional three-port laparoscopy in children, meaning no additional cost. • Cosmesis seems to be a self-evident benefit of SIPES, although there is no objective assessment of it among authors in the literature, and it must be carefully weighed against the possibility of affecting the safety of the procedure. • Experienced endoscopic surgeons might consider SIPES as another surgical approach to treat certain pathologies; however, the execution of prospective controlled trials is pending to demonstrate, with objective evidence, the real benefits of this less invasive approach. • Pediatric patients have particular characteristics that allow minimally invasive surgery to be performed safely with the use of hybrid assistance, like reduced ports, stab incisions, and percutaneous retraction sutures. Until the effectiveness of SIPES procedures is proven, we strongly recommend to keep on performing “minilaparoscopy” in our pediatric patients.
Footnotes
Disclosure Statement
No competing financial interests exist.