
Abstract
Abstract
Objectives:
The purpose of this study was to analyze the feasibility and safety of robotic resection of benign upper neck masses through a modified facelift approach.
Patients and Methods:
Between November 2010 and February 2012, 9 patients were enrolled in this prospective study. Six patients received a robotic submandibular gland resection via a retroauricular approach. Two patients received robotic resection of the second branchial cleft cyst. One patient received robotic operation for the removal of lymphadenopathy, which occurred in the submental area.
Results:
Robotic resection of a benign upper neck mass was successfully performed through a retroauricular approach in all patients. The average robotic system docking times and robotic operation times were 8.5 minutes and 62.4 minutes, respectively. All patients were extremely satisfied with their cosmetic results after the operation. There were no cases of nerve palsy in the marginal mandibular branch of the facial nerve, the lingual nerve, the hypoglossal nerve, or the spinal accessory nerve. No patient required blood transfusion in response to significant bleeding or was converted to open surgery. Mean blood loss was minimal (6.6 mL). The average period of follow-up for the patients was 12.7 months. All patients have maintained disease-free status.
Conclusions:
Robotic resection of a benign upper neck mass via a retroauricular approach is technically feasible and results in better cosmetic outcomes than the conventional transcervical approach. This new surgical method is safe and effective for benign upper neck masses that require surgical removal.
Introduction
Accordingly, there have been several attempts to develop new approaches that minimize or hide the incision scar resulting from the resection of benign upper neck masses.1–4 In these previous studies, the investigators usually excised the submandibular gland (SMG) or the branchial cleft cyst through a retroauricular approach using endoscopy and long surgical instruments. Because the incision scar can be hidden behind the retroauricular hairline, these procedures result in better cosmetic outcomes than conventional transcervical approaches. However, endoscopic surgery with a retroauricular approach, compared with a conventional transcervical approach, introduces several difficulties. First, the operation must be performed in a narrow working space due to the distance between the retroauricular incision and the lesions. Second, because the assistant typically handles the endoscope and moves it according to the surgeon's movement, the assistant and the surgeon often collide while performing this surgery.
To overcome the limitations of endoscopic surgery, we performed robotic surgery for the resection of benign upper neck masses using a retroauricular approach. We used the daVinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA), which is used regularly in the field of head and neck surgery. In robotic surgery, the endoscopic arm is equipped with two integrated cameras. The arm is inserted through a single retroauricular incision and is located close to the operative field. This setup gives a three-dimensional, magnified view of the operative field, allowing the surgeon to perform the operation bimanually by controlling two robotic instrument arms remotely. The surgeon can thus perform the operation easily and precisely without the collision problems associated with endoscopic surgery. We collected and analyzed treatment outcomes of patients who received robotic surgery for the resection of benign upper neck masses to confirm the validity of the procedure.
Patients and Methods
Patients
We obtained approval from the Institutional Review Board of Yonsei University, Seoul, Korea, before initiating this study. Between November 2010 and February 2012, 9 patients were enrolled in this prospective study. The average age of the patients was 31.4 (range, 18–50) years; 7 patients were female, and 2 patients were male. Six patients received robotic SMG resection for the treatment of benign disease entities that occurred in the SMG. Two patients underwent robotic resection of second branchial cleft cysts. One patient underwent robotic operation for the removal of a lymphadenopathy in the submental area. Prior to the operation, computed tomography scanning was performed on all patients to evaluate the extent and location of the lesions. Fine needle aspiration biopsy was conducted to rule out malignant tumors in all patients. All patients were counseled about the advantages and disadvantages of robotic surgical techniques, and informed consent was obtained from all patients prior to surgery. Other clinical information is summarized in Table 1.
EBL, estimated blood losa; F, female; M, male; SMG, submandibular gland.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) patients who were at least 18 years old at the time of diagnosis or (2) patients with benign disease entities of the upper neck (level I–III) with indication for surgery. Exclusion criteria were as follows: patients with (1) contraindication for surgery or general anesthesia, (2) suspected malignant neoplasm, or (3) previous treatment of the neck, including surgery or radiation.
Surgical procedure
After the patient was given general anesthesia, orotracheal intubation was performed to secure the airway. After the patient was placed in a supine position on the surgical bed, the patient's head was rotated toward the contralateral side of the lesion, and a shoulder roll was inserted beneath the patient's shoulder to extend the head and neck. The protocol for making a skin incision with a retroauricular approach is as follows: the incision started from the retroauricular sulcus in the inferosuperior direction. The incision was curved posteriorly and caudally at the level of the external auditory canal. Using this protocol, the incision was located about 0.5 cm beneath the hairline so that the incision scar would be hidden postoperatively. The skin flap was elevated using monopolar cautery along the subplatysmal plane, with the sternocleidomastoid muscle (SCM) and the greater auricular nerve as landmarks. The incision was continued to the midline of the anterior neck and superiorly to the inferior border of the mandible and inferiorly to the level of inferior border of the cricoid cartilage. During the skin flap elevation, the assistant pulled the skin flap upward with an Army–Navy retractor to help the surgeon elevate the skin flap. A self-retaining retractor was then inserted through the retroauricular incision to maintain the working space, and the endoscopic arm and two instrument arms were inserted through the single retroauricular incision (Fig. 1).
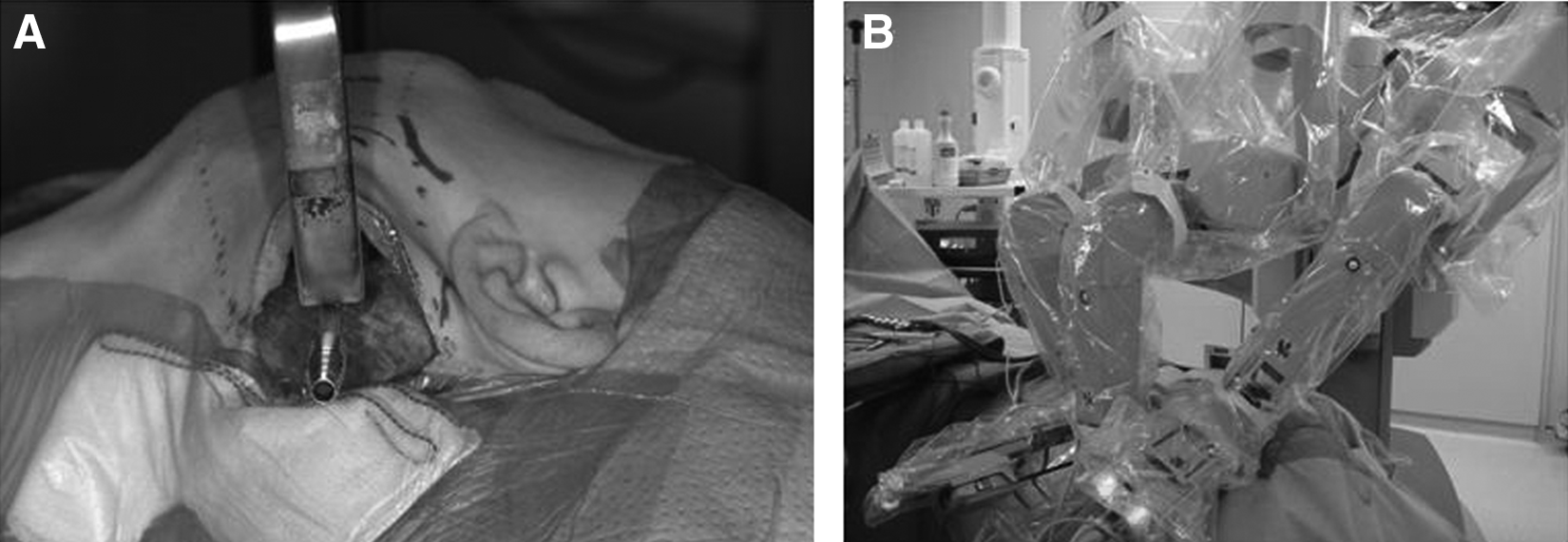
Working space for robotic resection of a benign upper neck mass via a retroauricular approach.
Robotic resection of branchial cleft cysts was performed via a retroauricular approach as follows (Fig. 2). After the anterior border of the SCM was identified, the deep cervical fascia encasing the SCM was opened along the anterior border. Dissection then proceeded toward the medial side of the SCM. The assistant then pulled laterally on the SCM with an Army–Navy retractor to open sufficient working space. The lesion then becomes observable between the carotid space and the medial side of the SCM, and dissection carefully continued along the lesion. The surgical plane was kept as close to the lesion as possible during the operation. Significant neurovascular structures could be easily preserved without iatrogenic injury if resection was done using Harmonic® (Ethicon Endo-Surgery, Blue Ash, OH) curved shears or monopolar cautery after the important structures under the surgical plane were identified by lifting and spreading the surrounding tissues with a Maryland dissector. Finally, the specimen was removed through the retroauricular incision, a single closed drainage was inserted behind the incision line, and the operation was completed.
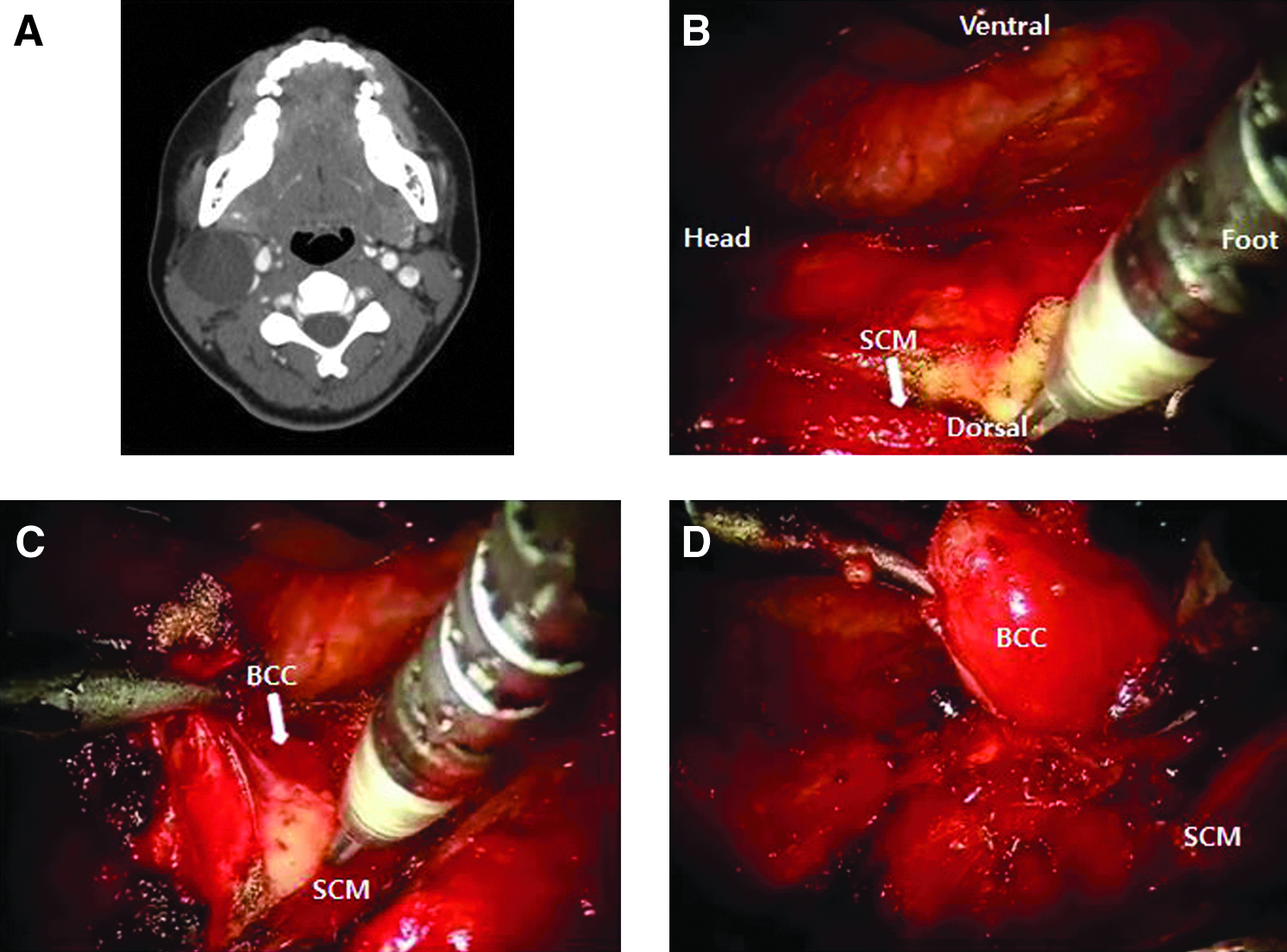
Robotic resection of a branchial cleft cyst (BCC) via a retroauricular approach.
Robotic resection of the SMG via a retroauricular approach was performed as follows (Fig. 3). During the skin flap elevation, the submandibular lodge could be easily observed under the mandible. The deep cervical fascia encasing the SMG was opened at the inferior border of the SMG and was stripped upward to avoid injury of the marginal mandibular branch of the facial nerve. Dissection was then performed in the postero-inferior portion of the SMG to identify the posterior border of the digastric muscle. At that point, the proximal portion of the facial artery was identifiable between the SMG and the posterior belly of the digastric muscle, and it was ligated with Harmonic curved shears or a hemoclip. Next, the SMG was dissected from the inferior border of the mandible. After the mylohyoid muscle was identified, it was lifted upward with Maryland forceps to reveal Wharton's duct, the hypoglossal nerve, and the lingual nerve. Wharton's duct was then ligated with a hemoclip, and the SMG specimen was removed through the retroauricular incision. The operation was completed after a single closed drainage was inserted behind the incision line.
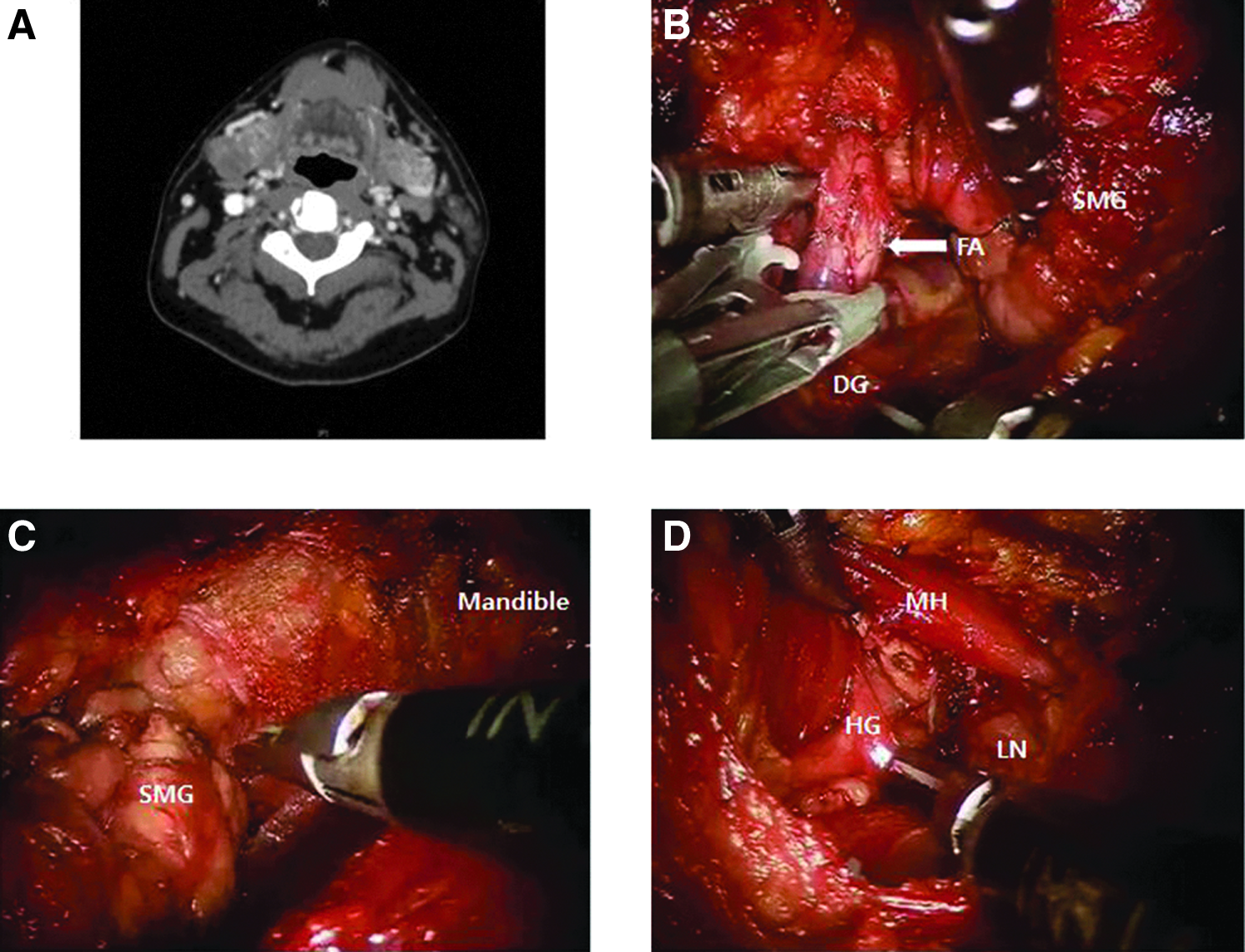
Robotic resection of the submandibular gland (SMG) via a retroauricular approach.
Results
Patients
Robotic resection of benign upper neck masses was successfully performed through a retroauricular approach in the 9 patients enrolled in this study. Six patients received robotic SMG resection via a retroauricular approach for the treatment of benign disease entities that occurred in the SMG. On pathologic examination, 3 patients were diagnosed with pleomorphic adenoma, and 3 patients were diagnosed with chronic sialadenitis. Two other patients received robotic excision via a retroauricular approach for the surgical treatment of level II cystic masses of the neck and were diagnosed as having branchial cleft cysts. One patient underwent robotic excision via a retroauricular approach for the treatment of a level Ia solid mass of the neck and was diagnosed with chronic lymphadenopathy.
Treatment outcome
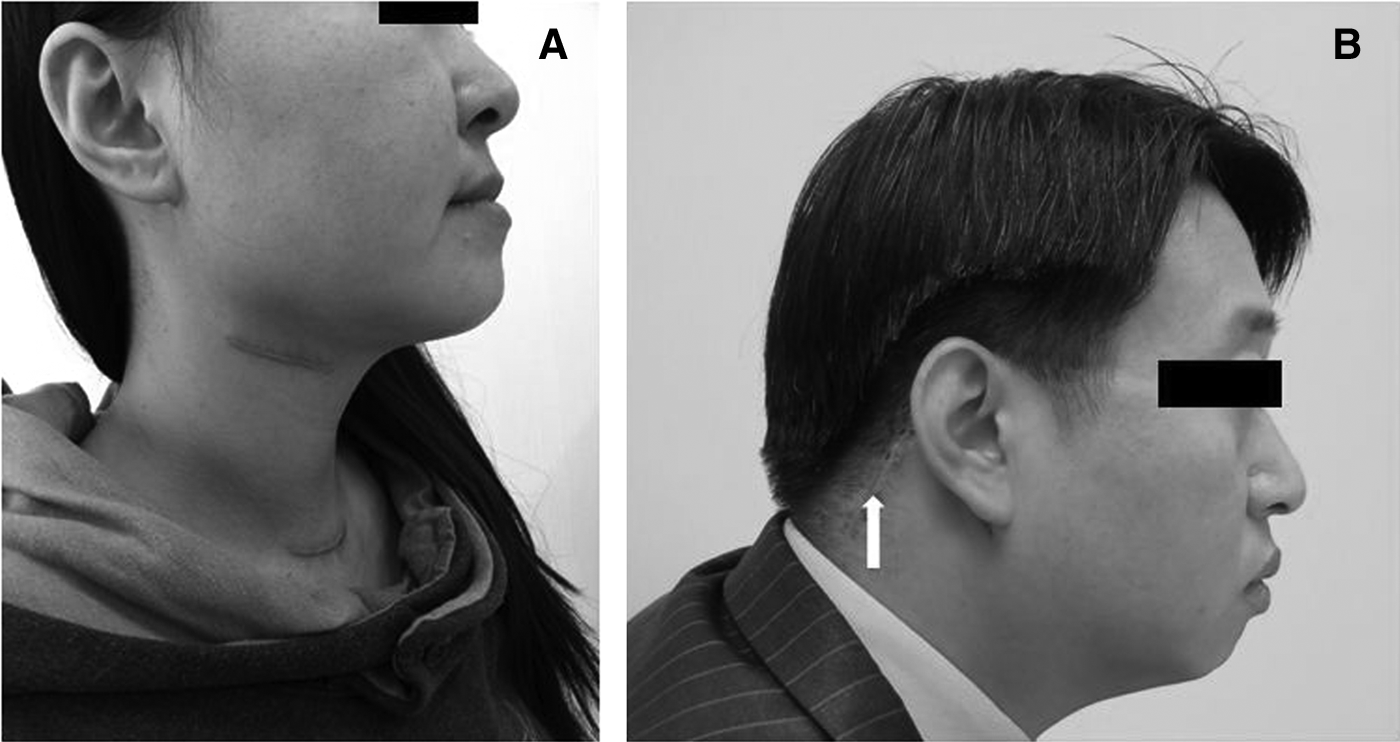
The average robotic system docking times and robotic operation times were 8.5 (range, 5–15) minutes and 62.4 (range, 45–85) minutes, respectively. The mean time of skin flap elevation was 30.1 (range, 25–32) minutes. The average amount of postoperative drainage was 22.3 mL, and the drainage duration was 2.2 days on average. The average hospital stay was 2.6 days. Patient satisfaction with the cosmetic results was measured on a graded scale of I (extremely satisfied), II (satisfied), III (average), IV (dissatisfied), and V (extremely dissatisfied). Eight patients were extremely satisfied with their cosmetic results after their operation, and 1 patient was satisfied with his cosmetic results (Fig. 4 and Table 2).
Complications
In this study, there were no cases of nerve palsy occurring in the marginal mandibular branch of the facial nerve, the lingual nerve, the hypoglossal nerve, or the spinal accessory nerve. The mean blood loss was minimal (6.6 mL), and no patients required a blood transfusion in response to significant bleeding or were converted to open surgery. No postoperative complications, such as hematoma, skin flap necrosis, or wound infection, occurred.
Follow-up
The average period of follow-up for the patients was 12.7 (range, 8–22) months. All patients have maintained disease-free status.
Discussion
Although a transcervical approach is commonly used for surgical treatment of neck diseases, this approach inevitably leaves a visible scar on the neck. It is important that this scarring can induce severe disfigurement in patients and leave them vulnerable to hypertrophic scars or keloids (Fig. 4A). These disfigurements may be a great burden to patients and can have negative psychological or social influences on their lives. 5 Accordingly, several studies have attempted to hide or minimize the incision line in order to obtain a better cosmetic outcome. In these studies, the operation to hide the incision scar was usually performed after the parotid surgery. Appiani 6 first reported the use of a rhytidectomy incision as a cosmetic approach for parotid surgery in 1967. Terris et al. 7 operated on parotid tumors through a modified facelift incision and reported better cosmetic satisfaction without additional postoperative complications. Facelift incisions leave a postoperative scar behind the retroauricular hairline, and patients were satisfied with these hidden scars. Since then, other researchers have used the facelift incision approach for the surgical treatment of other diseases of the neck. In particular, Kim et al. 1 reported an endoscopic-assisted submandibular sialadenectomy via the facelift approach. Roh 8 reported on the removal of upper neck masses via a retroauricular approach. In cases in which a facelift or retroauricular approach was used to resect the lesions, complications related to the operation did not occur, and patients were satisfied with their cosmetic outcomes.
However, facelift or retroauricular approaches have several disadvantages. It takes more time to elevate the skin flap because of the long distance between the incision and the lesion, causing the assistant to need to continuously retract the skin flap during the elevation process. This can cause the long and thin skin flap to become necrotized because of poor vascular supply and continuous retraction during the operation. Additionally, unlike the conventional transcervical approach, the surgeon may not be used to the superior-to-inferior anatomic orientation that is required with a retroauricular approach, which results in a narrow working space and difficulty obtaining a sufficient view of the anterior lesion. In endoscopic surgery, although the endoscope gives the surgeon a magnified view of the operative field within a narrow space, it also necessitates that the assistant hold the endoscope during the entire operation and move the scope in response to the surgeon's movement. This can lead to collisions between the surgeon and the assistant that can hamper their ability to perform the operation precisely and completely. In addition, because of the “level effect” when using a long instrument, it is difficult to perform endoscopic surgery precisely.
Transoral robotic surgeries and robotic thyroidectomies using the daVinci Surgical System have been actively researched in the field of head and neck medicine.9–14 The endoscopic arm is equipped with two integrated cameras. This gives the surgeon a three-dimensional magnified view of the operative field and allows the operator to perform the removal of the upper aerodigestive tract tumor transorally and to perform robotic thyroidectomy within a narrow space by using the two articulated instrument arms. Recently, Singer et al. 15 and Terris et al. 16 performed a robotic facelift thyroidectomy using the daVinci Surgical System and reported the feasibility and safety of these procedures. They noted several advantages of this procedure, including lessening of the extent of dissection, more rapid wound healing, outpatient management without the use of closed drainage in the postoperative period, and better cosmetic outcomes. The concept for our study originated from this previous research. We performed robotic resection of benign upper neck masses via a retroauricular approach. In all our patients, the operations were successfully completed without any additional complication such as skin flap necrosis or hematoma. The average blood loss was minimal (6.6 mL). The drainage tube was removed, on average, 2.2 days postoperatively, and the average hospital stay was 3.2 days. During the follow-up period of 12.7 months, there were no cases of disease recurrence. All patients were satisfied with their cosmetic outcomes (Fig. 4B).
The neck is a complex anatomical structure in which main vessels and various cranial nerves are located. Accordingly, there are risks associated with surgery in this region, such as significant bleeding from main vessels or neural injury to the cranial nerves. In robotic surgery using the daVinci Surgical System, an endoscopic arm equipped with two integrated cameras can be located close to the operative field through a single retroauricular incision. Therefore, the surgeon can observe even tiny vessels that would be difficult to observe easily through a narrow working space inlet with the naked eye. In addition, these operations can be performed precisely and bimanually in a limited narrow working space by using two instrument arms, which are able to move freely within a narrow space. In endoscopic surgery, the surgeon typically uses long instruments to perform the operation through a long and narrow working space. Because of the long axis of the instruments, the lever effect cannot be avoided, making it difficult to perform the operation precisely. In addition, collisions between the surgeon and the assistant occur throughout the operation. Surgeons must gain a great deal of experience performing endoscopic surgery before they can overcome these problems. Alternatively, with robotic surgery, the surgeon can control the two robotic arms remotely from the console, avoiding the collisions associated with endoscopic surgery.
Conclusions
Although surgeons can perform a precise operation with the superiority of the robotic daVinci Surgical System, an appropriate training program was required for the operator to adapt to robotic surgery. Before the initiation of this study, the senior author (S.H.K.) had already received training and performed the robotic surgery on more than 100 cases. With these requirements, robotic resection of benign upper neck masses via a retroauricular approach is technically feasible and results in better cosmetic outcomes than the conventional transcervical approach. This new surgical method is safe and effective for benign upper neck masses that require surgical removal.
Footnotes
Disclosure Statement
No competing financial interests exist.