
Abstract
Abstract
Background:
Laparoscopy is established as a standard of care in a variety of gynecological pathologies. Pneumoperitoneum and reverse Trendelenburg positioning during laparoscopy have been claimed to increase thrombosis risk, albeit these proposals are still controversial. The aim of this study was to assess lower extremity venous blood flow by Doppler sonography in patients undergoing laparoscopic gynecological surgeries.
Patients and Methods:
A prospective, nonrandomized, controlled study was designed to compare lower extremity venous Doppler measurements in patients undergoing diagnostic and operative gynecological laparoscopies. In the period from May 2010 to April 2011, in total, 96 patients operated on for various gynecological complaints excluding malignancy were enrolled in the study. Thirty-two of these patients underwent diagnostic laparoscopy, 34 underwent operative laparoscopy, and 30 underwent open surgery. Lower extremity venous blood flow was investigated by Doppler sonography in patients the day before surgery and 24 hours afterward. Preoperative and postoperative Doppler measurements were obtained from bilateral common and superficial femoral, bilateral great saphenous, and bilateral popliteal veins.
Results:
Lower extremity venous Doppler measurements were similar in diagnostic and operative laparoscopy groups. Femoral venous blood flow measurements were observed to be similar, but great saphenous and popliteal blood flows were found to be significantly decreased in the open surgery group compared with laparoscopic operations.
Conclusions:
The laparoscopic approach in gynecological surgery is not associated with an adverse effect on lower extremity blood flow and seems not to bring an additional risk of thrombosis.
Introduction
Pneumoperitoneum might lead to thromboembolic complications by its detrimental effect on venous flow due to increased abdominal pressure and reverse Trendelenburg positioning and by activation of the hemostatic system. 10 It was demonstrated that CO2 pneumoperitoneum might lead to increased blood viscosity and red blood cell aggregation, both of which may potentiate the risk of thrombosis. Pneumoperitoneum also might cause stasis on peripheral veins.
The present study assessed pre- and postoperative lower extremity venous blood flow by Doppler sonography in patients undergoing diagnostic and operative laparoscopic gynecological surgeries. The requirement for thromboprophylaxis has been explored in laparoscopic gynecological procedures.
Patients and Methods
In total, 96 patients operated on for various gynecological complaints or infertility between May 2010 and April 2011 were prospectively included in the present study. Patients with disorders related to the vascular system and gynecological malignancies were excluded. None of the patients included in the study was in need of postoperative anticoagulant therapy. Institutional review board approval was obtained from the University Ethics Committee. All the patients gave written informed consent for the study.
The patients underwent gynecological operations under general anesthesia. Of the patients, 32 underwent diagnostic laparoscopic surgery, 34 underwent operative laparoscopic surgery, and the remaining 30 underwent open gynecological operations. Anesthesia was in standard fashion using the same sedatives, narcotics, and muscle relaxants for all the patients. During laparoscopic surgery patients were placed supine in the Trendelenburg position at an angle of 20–30°. The pneumoperitoneum was established by insufflation of CO2 through a Veress needle and maintained at 14–16 mm Hg pressure.
Color Doppler ultrasound evaluates the diameter, blood velocity, and the amount of the blood flow in the vessels. Color Doppler examinations of the lower extemity vessels were performed the day before surgery and 24 hours afterward. All the sonographic examinations were performed by the same physician using the Aplio XG device from Toshiba Medical Systems Co. Ltd. (Tokyo, Japan) with a 12-MHz linear probe. Measurements were obtained both preoperatively and postoperatively from bilateral common and superficial femoral, bilateral great saphenous, and bilateral popliteal veins. Peak systolic velocity values were recorded. Preoperatively a coagulation profile, including activated partial thromboplastin time, prothrombin time, international normalized ratio, and complete blood count, was obtained.
The statistical analysis was performed using SPSS version 15.0 software (SPSS Inc., Chicago, IL). Descriptive statistics were used to analyze the data variables. Comparisons between pre- and postoperative Doppler measurements were performed using Student's t test. Comparisons among the three groups of patients stratified as diagnostic laparoscopy, operative laparoscopy, and open surgery were performed using one-way analysis of variance. A P value <.05 was considered statistically significant.
Results
In total, 96 patients operated on between May 2010 and April 2011 were included in the study; their mean age was 35 years (range, 19–56 years). Indications for laparoscopy and open surgery are shown in Figure 1. All the operations were performed for benign gynecological problems.
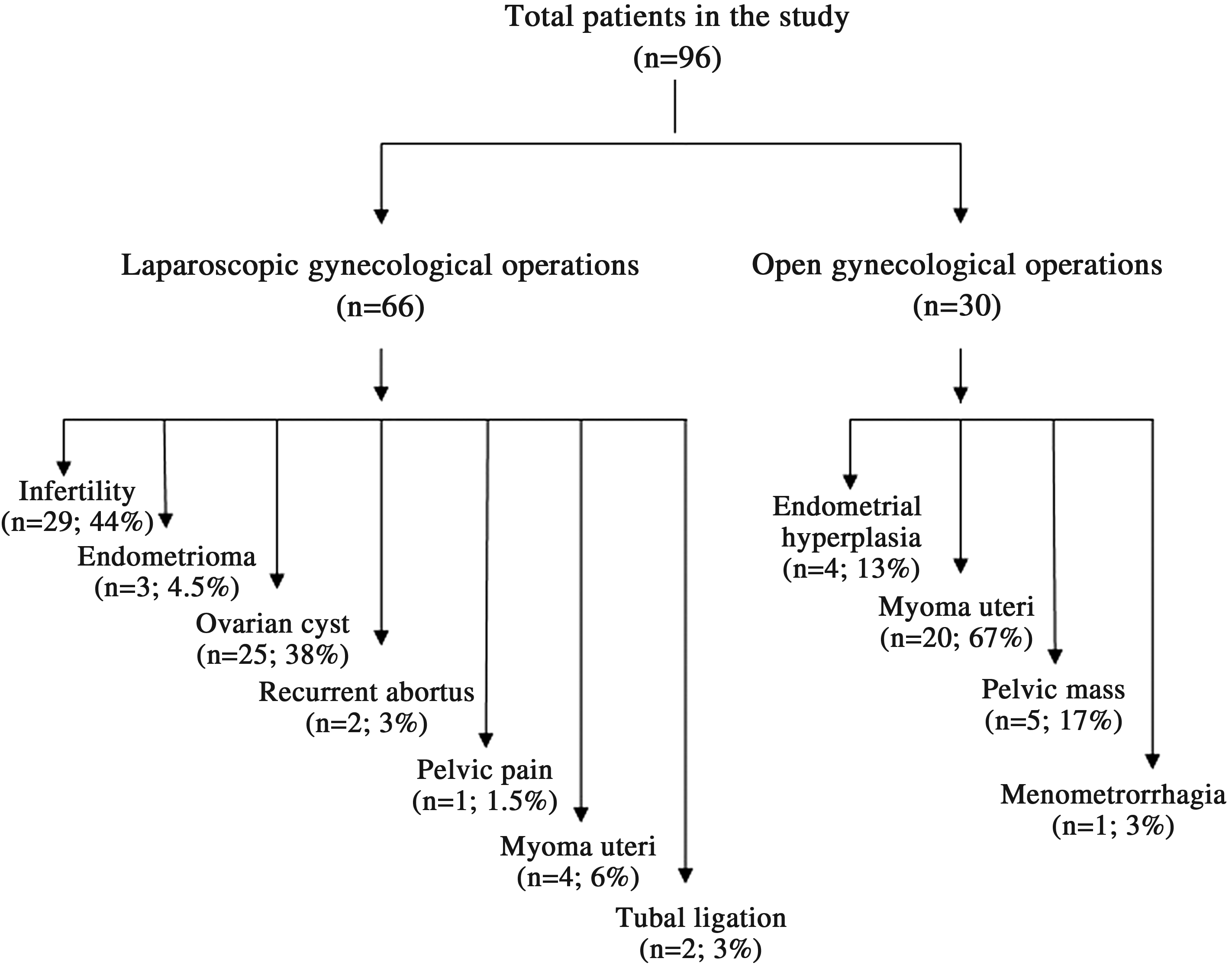
Indications for laparoscopic and open gynecological surgery.
We categorized operations into three groups as diagnostic laparoscopy, operative laparoscopy, and open surgery groups. In the first group (Group 1) 32 patients underwent diagnostic laparoscopy at a pressure of 14–16 mm Hg, in the second group (Group 2) 34 patients underwent operative laparoscopy at a pressure of 14–16 mm Hg, and in the third group (Group 3) 30 patients underwent open gynecological surgery. There was no statistically significant difference between Groups 1 and 2 in terms of age, body mass index, operation duration, and blood parameters of activated partial thromboplastin time, prothrombin time, hemoglobin, hematocrit, and platelets (Table 1). The mean duration of the operation was 62 minutes (range, 30–90 minutes) in the diagnostic laparoscopy group and 70 minutes (range, 60–120 minutes) in the operative laparoscopy group. Operation duration was significantly longer in Group 3 compared with Groups 1 and 2, as expected (Table 1).
Rows with the same superscript letters are significantly different: aP<.001, bP<.001, cP=.024, dP=.007, eP=.004, fP=.05, gP=.003, hP=.005.
aPTT, activated partial thromboplastin time; BMI, body mass index; INR, international normalized ratio; NS, not significant; PT, prothrombin time.
In each group, preoperative and postoperative Doppler measurements from both common and superficial femoral veins, great saphenous, and popliteal veins were almost identical except for left great saphenous vein blood flow in Group 1, which increased postoperatively (Table 2). When Doppler measurements in Groups 1 and 2 were compared, no significant difference was observed in the preoperative measurements (Table 3). Postoperatively, left great saphenous vein blood flow was found to be significantly lower in the operative laparoscopy group compared with the diagnostic laparoscopy group (Table 4).
LCFV, left common femoral vein; LGSV, left great saphenous vein; LPOPV, left popliteal vein; LSFV, left superficial femoral vein; NS, not significant; Post, postoperative; Pre, preoperative; PSV, peak systolic velocity; RCFV, right common femoral vein; RGSV, right great saphenous vein; RPOPV, right popliteal vein; RSFV, right superficial femoral vein.
Rows with the same superscript letters are significantly different: aP=.035, bP=.01, cP=.005, dP=.007, eP=.006.
LCFV, left common femoral vein; LGSV, left great saphenous vein; LPOPV, left popliteal vein; LSFV, left superficial femoral vein; NS, not significant; PSV, peak systolic velocity; RCFV, right common femoral vein; RGSV, right great saphenous vein; RPOPV, right popliteal vein; RSFV, right superficial femoral vein.
Rows with the same superscript letters are significantly different: aP=.045, bP=.009, cP=.001, dP=< .001, eP=.024, fP=.0005, gP=0.006, hP=.001.
LCFV, left common femoral vein; LGSV, left great saphenous vein; LPOPV, left popliteal vein; LSFV, left superficial femoral vein; NS, not significant; PSV, peak systolic velocity; RCFV, right common femoral vein; RGSV, right great saphenous vein; RPOPV, right popliteal vein; RSFV, right superficial femoral vein.
To compare laparoscopic surgery with open surgery, postoperative blood flow in the great saphenous and popliteal veins in the open surgery group (Group 3) was found to be significantly decreased compared with both Groups 1 and 2 (Table 4). Although preoperative popliteal venous blood flow was already significantly lower in Group 3 compared with both Groups 1 and 2, the postoperative decrease in popliteal venous blood flow was even more significant (Tables 3 and 4).
Discussion
The present study demonstrated that both the diagnostic and the operative gynecological laparoscopy procedures caused no detrimental effect on the lower extremity venous blood flow. In other words, no additional venous stasis in the lower limbs occurs in laparoscopic gynecological surgery, and it might even be safer for patients with benign gynecological problems. However, operation duration is probably the key player.
Pharmacological thromboprophylaxis for laparoscopy was recommended to be the same as for conventional surgery (i.e., individualized according to additional thrombosis risk factors and continued for a minimum of 7–10 days). 7 Many authors advised using low insufflation pressure during surgery and postoperative use of low-molecular-weight heparin and also anti-embolic stockings as routine measures during laparoscopy to prevent DVT. 9 Other recommended measures are keeping the reverse Trendelenburg position at a minimum and intermittent release of the pneumoperitoneum in long operations. General anesthesia, muscle relaxants, and pneumoperitoneum together have been suggested to cause venous stasis in the lower extremity.11,12 Stasis is one of the Virchow triad for thrombosis, and anesthesia alone is a reason for venous stasis at lower extremities. Pneumoperitoneum was suggested to predispose to DVT, and a long operation duration in the reverse Trendelenburg position was noted as a further potentiating factor. 7 On the other hand, some authors reported that the risk of thromboembolic disease due to pneumoperitoneum was theoretical. 13 Similarly, Bais et al. 6 did not confirm the presence of venous stasis during laparoscopic surgery. It was demonstrated that venous stasis in the lower limbs significantly increased when pneumoperitoneum exceeded 12 mm Hg, which was shown as a markedly decreased peak blood velocity and significant dilation of the femoral vein intraoperatively. 11 However, on postoperative scans reversal to normal was noted, and no postoperative DVT occurred in a group of 65 patients. 11 The authors underlined the potential for thrombotic complications when intraabdominal pressure exceeded 12 mm Hg, although abdominal insufflation up to 20 mm Hg has been demonstrated to be well tolerated in most patients. 14 In the present study, both diagnostic and operative laparoscopies were performed at 14–16 mm Hg pressure, and no postoperative thromboembolic complication occurred in 66 patients.
In a recent study by Nick et al., 15 the incidence of DVT or pulmonary embolism in 849 patients undergoing laparoscopic gynecological operations was investigated, and the thromboembolism risk was found to be 0.7%. The authors categorized operations as low-intermediate complexity and high complexity, including gynecological malignancies, and recommended postoperative anticoagulation only in high-complexity operations. In another study including 266 patients, in order to assess the incidence of venous thromboembolism in laparoscopic gynecological procedures, sonographic evaluation was performed 7 and 14 days postoperatively, and telephone contact was scheduled 30 and 90 days afterward. 16 In that study, patients with previous venous thromboembolism and malignancy were also excluded. The authors reported no venous thromboembolism either sonographically or clinically, and gynecological laparoscopy in nonmalignant cases was claimed to be a low-risk procedure for postoperative venous thromboembolism. In the present study, we categorized operations as diagnostic and operative laparoscopic gynecological operations and distinctly excluded gynecological malignancies from the study. No significant difference was found between the two laparoscopy groups as regards Doppler measurements 24 hours postoperatively.
Duration of laparoscopic surgery was suggested to have a significant effect on activation of coagulation, and increased duration of pneumoperitoneum might lead to an increased risk for the development of postoperative DVT. 17 Operative laparoscopies are usually longer in duration and therefore might be associated with a higher probability of thromboembolic complications. In a case report by Hsieh et al., 18 a massive pulmonary embolism causing sudden cardiac arrest in the immediate postoperative period in an otherwise healthy woman who had a laparoscopic hysterectomy was presented. Pneumoperitoneum was claimed as the factor interfering with venous flow in the lower extremities predisposing to DVT or pulmonary embolism. In the present study, diagnostic and operative laparoscopic operations were compared, and similar color Doppler examination results were obtained in both groups. However, operation duration was similar in the diagnostic and operative laparoscopy groups; therefore those statistically similar Doppler measurements might be due to similar operation durations in the two groups. Further studies with significantly different operation durations might reveal dissimilar results.
When the patient is in the head-down tilt position, the femoral vein diameter decreased, and the velocity and the amount of blood flow increased. However, in the feet-down tilt position, the femoral vein diameter increased, and the velocity and the amount of blood flow decreased. Moreover, with the increase of pneumoperitoneum pressure, the femoral vein diameter increased, and the velocity and the amount of blood flow decreased. 12 As a result, the head-down tilt position should decrease the risk of DVT after the laparoscopy; however, the feet-down tilt position and CO2 pneumoperitoneum might increase the risk. Laparoscopic cholecystectomy, in contrast to gynecological laparoscopy, is performed in the reverse Trendelenburg position, which potentiates any venous stasis due to anesthesia and pneumoperitoneum. To summarize, the head-down tilt position in gynecological laparoscopy facilitates blood circulation and therefore diminishes the risk of DVT after laparoscopy; however, the feet-down tilt position in laparoscopic cholecystectomy together with CO2 pneumoperitoneum can interfere with the recirculation of blood and increase the risk of DVT following laparoscopy.
In conclusion, laparoscopic surgery in patients with benign gynecological problems might be considered as a safe approach with regard to thrombosis risk. Scientific evidence in relation to thromboprophylaxis for gynecological laparoscopic surgery is limited; therefore patients should be evaluated individually based on risk factors. Future investigation including different risk groups and various laparoscopic gynecological procedures is warranted.
Footnotes
Acknowledgments
We thank to the doctors, nurses, and staff who have treated and taken care of the patients included in the study.
Disclosure Statement
No competing financial interests exist.