
Abstract
Abstract
Introduction:
Pediatric renal transplant patients may require native nephrectomy to avoid complications at the time of kidney transplantation. We have performed unilateral and bilateral transperitoneal pretransplant laparoscopic nephrectomies (PLNs), followed by living-related renal transplantation. The benefits of transperitoneal versus retroperitoneal dissection remain controversial.
Subjects and Methods:
A retrospective review of patients who underwent unilateral or bilateral transperitoneal PLNs between May 1, 2001 and April 30, 2009 was performed. A transperitoneal approach was used in all patients.
Results:
Eight patients underwent transperitoneal PLN. Four patients were female, and the average age was 91 months (range, 9–199 months). Five of the cases involved bilateral nephrectomy. Average operating times, including hemodialysis catheter placement and other procedures, was 4.93 hours (range, 4.25–5.97 hours) for bilateral PLN and 3.93 hours (range, 2.57–5.48 hours) for unilateral PLN. The average hospital stay was 5.9 days. All patients underwent successful renal transplantation following PLN without rejection at an average 2.3 years of follow-up.
Conclusions:
PLN appears to be an effective, safe method of removing potentially problematic, diseased kidneys prior to planned renal transplantation. A transperitoneal technique using four midline ports affords excellent access to both kidneys and, more importantly, allows for additional procedures to be completed simultaneously.
Introduction
Laparoscopic approaches to performing unilateral and bilateral nephrectomy have gained wide acceptance in the pediatric surgical and urological literature over the past decades.3,4 Pretransplant laparoscopic nephrectomies (PLNs) are performed using several approaches and methods. The most common methods include the retroperitoneal or transperitoneal approach. Several controversies still exist in the debate of performing retroperitoneal versus transperitoneal nephrectomy. Most surgeons tend to favor a particular technique. At present there is no statistical advantage in performing one approach over another, although individual studies have shown small differences.5,6
In a study by El-Ghoneimi et al., 7 13 patients safely underwent bilateral retroperitoneal pretransplant nephrectomy. Although this retroperitoneal approach is safe, it is somewhat inconvenient for bilateral nephrectomy because of the need for repositioning of the patient after the first kidney is removed. Furthermore, a bilateral nephrectomy is rarely performed without a vascular or peritoneal dialysis access procedure simultaneously or soon postoperatively. 8 Although the practice at our institution is to place an HD catheter at the time of operation, previous case studies and case series describe bilateral nephrectomy with placement of peritoneal dialysis catheters for long-term access.8,9 Some authors have argued against PLN in patients less than 1 year of age or weight less than 10 kg, yet recent studies have shown that unilateral and bilateral nephrectomies are safe in these high-risk populations.10–12
The pediatric surgeons at our institution perform the majority of unilateral or bilateral nephrectomies through the laparoscopic, four-port, transabdominal approach and remove the kidney(s) through the umbilical port site. Furthermore, we place HD catheters that allow for immediate dialysis postoperatively. The purpose of this study was to determine if our technique is a safe and efficacious modality for removing native kidneys. Additionally, it was of interest to determine if this method has yielded minimal long-term complications after renal transplant.
Subjects and Methods
Study procedures
The study design was a retrospective case series. The records of all patients who underwent unilateral or bilateral transperitoneal PLN at Helen DeVos Children's Hospital (Grand Rapids, MI) between May 2006 and April 2009 were reviewed. All patients in this study were recommended to have undergone PLN for end-stage renal disease. All patients who underwent unilateral or bilateral nephrectomy for the purpose of subsequent transplant had an HD catheter placed during the operation. Two separate pediatric surgeons at one institution performed all procedures. This study was approved by the Spectrum Health Institutional Review Board.
Data analysis
Patient demographics, disease information, operative data, and postoperative data were analyzed. Summary statistics were calculated for the data. Two cases of unilateral nephrectomy had no indication to undergo transplantation and therefore were excluded in the analysis of time to transplantation.
Results
Eight patients were identified who had a unilateral or bilateral transperitoneal PLN. Four were female, and the average age was 91 months (range, 9–199 months). Five cases identified as bilateral, and 3 cases were unilateral nephrectomy. All had indications to undergo subsequent transplantation. Indications for bilateral nephrectomy included congenital nephrotic syndrome (2 patients), high-output renal failure, vesicoureteral reflux with recurrent pyelonephritis, and cystinosis. Indications for unilateral nephrectomy included dysplastic kidney disease, nonfunctional pelvic kidney, and renal failure secondary to posterior urethral valves.
Average operating time, including HD catheter placement and other procedures, was 4.93 hours (range, 4.25–5.97 hours) for bilateral PLN and 3.93 hours (range, 2.57–5.48 hours) for unilateral nephrectomy. Of special note is that all patients who underwent bilateral or unilateral nephrectomy also had additional procedures that added to the operating room time. One patient had additional placement of a peritoneal dialysis catheter and omentectomy, while another had an HD catheter placed and bilateral inguinal hernias repaired.
The average hospital stay was 5.9 days: 7.6 days for bilateral nephrectomy and 3.0 days for unilateral nephrectomy. Average intraoperative blood loss was 53 mL. One patient required transfusion because of an HD catheter complication secondary to a blood loss of 150 mL. No other complications occurred related to PLN, HD, or transplantation. All patients underwent successful renal transplantation an average of 90 days (range, 32–18 days1) following PLN. Allograft survival was 100% with no rejection at an average of 2.3 years of follow-up.
Discussion
Pretransplant nephrectomies via retroperitoneal and transperitoneal approaches are described in the literature.1,3–7 Based on our case series, the latter approach is shown to be efficacious compared with data available in the literature.4–6 In our cohort we found several advantages to performing a transperitoneal nephrectomy.
At our institution, all patients received additional procedures at the time of nephrectomy. The use of a supine position made procedures such as peritoneal dialysis catheter placement, omentectomy, and inguinal hernia repairs more feasible in our small cohort. All patients who undergo bilateral nephrectomies require dialysis catheter placement during nephrectomy or in the perioperative period. By performing simultaneous placement of a HD catheter, our patients were spared an additional procedure in the pre- or postoperative period. Urrutia et al. 8 first described the placement of a peritoneal dialysis catheter during pretransplant bilateral nephrectomy. They also encouraged supine positioning and a transperitoneal approach as it offered ease of catheter placement compared with a retroperitoneal approach.
In our study, all patients, in addition to having undergone a unilateral or bilateral nephrectomy, also had an HD catheter placed, while two patients had concurrent procdures (e.g., hernia repair and omentectomy). It is possible that other necessary procedures could be consolidated when a patient undergoes PLN with a transperitoneal dissection. Additional procedures such as those that we performed would not be possible through a retroperitoneal approach. Theoretically, there is risk of complication from longer operating room times when additional procedures are performed, but overall we feel the risk is justified when a patient may need to undergo subsequent operations to perform additional procedures.
The transperitoneal and retroperitoneal approaches require markedly different positioning of the patient during the procedure. For a retroperitoneal dissection, the patient is placed in a lateral decubitus position and must be repositioned mid-procedure when bilateral nephrectomies are performed. With a transperitoneal approach the patient remains supine throughout the dissection. The only significant transition during the procedure is the surgeon moving to the other side of the operating room table between nephrectomies (Fig. 1). No significant changes with regard to patient repositioning or draping is required with a transperitoneal approach.
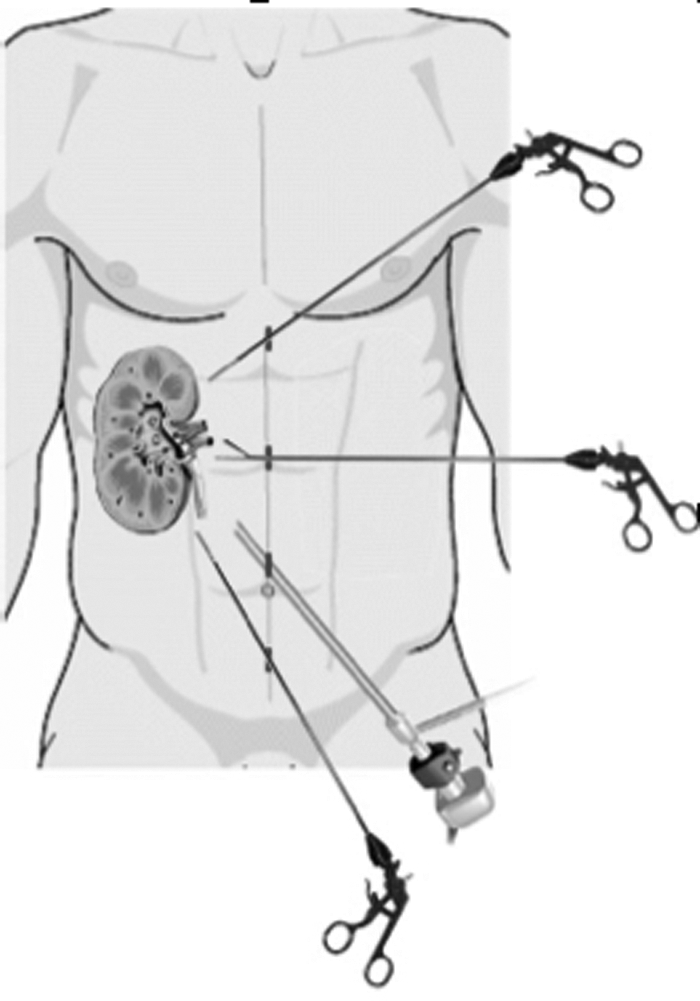
Four-port laparoscopic approach demonstrating positioning of ports during nephrectomy.
For both laparoscopic approaches, the benefits of pain control and length of stay have been demonstrated in previous studies. 13 However, only four incisions are required for the transperitoneal procedure. Although we did not specifically analyze analgesia in our group of patients, we suspect that four incisions in the midline abdomen offer improved comfort, compared with patients who have undergone a bilateral retroperitoneal approach. These patients need three bilateral laparoscopic incisions that are muscle splitting, whereas the transperitoneal approach offers the benefit of midline trocar placement where, theoretically, no muscle fibers are traversed.
In conclusion, based upon our small sample set, we believe that the bilateral transperitoneal approach offers a distinct advantage over a retroperitoneal approach in pediatric pretransplant bilateral nephrectomies, with regard to reduced positioning of the patient during the procedure as well as fewer incisions.
Footnotes
Acknowledgments
We would like to thank Alan Davis, PhD, and the Grand Rapids Medical Education Partners Research Department for their help reviewing and preparing this manuscript.
Disclosure Statement
T.B. has received honoraria/speaking fees from Gambro Healthcare. B.J.G., D.R., and J.D. have no competing financial interests.