
Abstract
Abstract
The authors describe the theoretical basis and development of simulation systems that led to the birth of “navigation in liver surgery.” Navigation is a new technological application in the surgical field that has already been successfully used in neurosurgery and orthopedic surgery. A precondition to navigate a liver resection is the availability of a map. There are three main methods to acquire images and build a three-dimensional map. Efforts to make navigation “feasible” have been made, but some limits are still affecting the method. Lack of millimetric accuracy, deformation of the liver parenchyma during resection, and breathing movements are some of the most important criticisms of this method, which, however, is still in its infancy. Not only experimental applications but also current and future foreseeable applications of such a technology are overviewed. Goals of this technology should be to reduce the intraoperative stress on surgeons, to shorten resection time, and even indirectly to enlarge resectability of patients. Further developments of this new technology applied to liver surgery could lead in the near future to safer and more precise resections, reducing the risk of postoperative liver failure, even in the presence of large anatomical alterations or, even more frequently in this surgical field, anatomical variants.
Introduction
Methods of Image Acquisition
In order to navigate a liver resection, an essential precondition is the acquisition of images to build a map that reproduces the 3D scenario in which the surgeon will perform an image-oriented (navigated) resection under real-time control of the position of surgical instruments.
Today there are three main methods to acquire images and build a 3D map. This can be achieved through ultrasonography, CT, or magnetic resonance (MR) scan data.13,15,16 Each method has advantages and limits; the most used seems to be the 3D CT reconstruction, which can give a good map of vessels that is of vital importance in liver surgery. The automated 3D CT reconstruction seems to be, from an analysis of reports, more comfortable for surgeons, as well as precise and giving fewer problems (economical and logistic such as MR imaging [MRI]). Of course, the quality of original images is very important to achieve a reasonable realistic 3D map for navigation. Integration of some software (Hepavision®; MeVis, Bremen, Germany) and tracking systems (infrared system; Polaris®; Northern Digital Inc., Waterloo, ON, Canada) has shown robust results in a clinical study. 17 Also, “pure” ultrasound-based navigation systems have shown in the clinical experience of the Charitè Group a good applicability in surgical practice.15,18 After many experimental and some clinical applications, the method of acquisition of data to achieve a good navigation map seems no longer to be a matter of debate. CT acquisition images and 3D reconstruction are widely used in clinical practice by many groups and in experimental models of navigation.19,20 The limits of CT scans are mainly limits of biliary tract visualization/3D reconstruction; these limits can be overcome with a complex integration of CT-MRI scan data. Some attempts have also been made with integration of MRI/intraoperative ultrasound data. 21
Navigation Systems
The second step, after achieving a map to follow the position of surgical instruments in real-time (navigation), is the translation of instrument position from real anatomy to the 3D model (virtual scenario), in a real-time manner (Fig. 1). This step is very important and needs a registration phase (usually done intraoperatively with internal fiducial points with well-known modalities that do not need to be described here16,17). Actually, one of the problems is to establish a workflow with known fiducials to be standardized in order to obtain a good reproducible registration technique that gives a middle error of less than 0.5 cm. Much effort has been made by some groups to achieve this goal. As concerns tracking systems, there are three main tracking systems available: MR gradient based, electromagnetic, and optical (infrared). The type most used in experimental models, but also in some published clinical experience, seems to be the infrared optical system.15–17 However, infrared-based tracking systems have shown limits in locating surgical instruments on the map and must be perfected (Fig. 2). Because of a middle error of about 1 cm in a point-by-point correspondence between virtual maps and reality, an interesting attempt to overcome the problem was made by Banovac et al. 22 and Beller et al. 23 through an integration of infrared and electromagnetic tracking systems. Electromagnetic tracking systems have shown the important limit of interferences with metal instruments in the operating theater. 23 Therefore, despite the idea of the Charitè Group that this could be a significant advance in the research field, it is not so easily applicable. Despite all the efforts of the last 6–7 years in the direction of a standard applicability of navigation systems in liver resections, some problems remain unsolved, delaying the introduction of navigation systems into daily clinical practice. It is interesting to note that some groups tried to “manually navigate” some liver resections using intraoperative 3D planning and interactively working with this tool, but did not achieve real-time control of the surgeon's position on the map. 24 Other similar published attempts without achieving real-time control of navigation but declaring “navigation of resection” have been carried out by some groups, testifying to the great interest of surgeons to acquire this new tool.
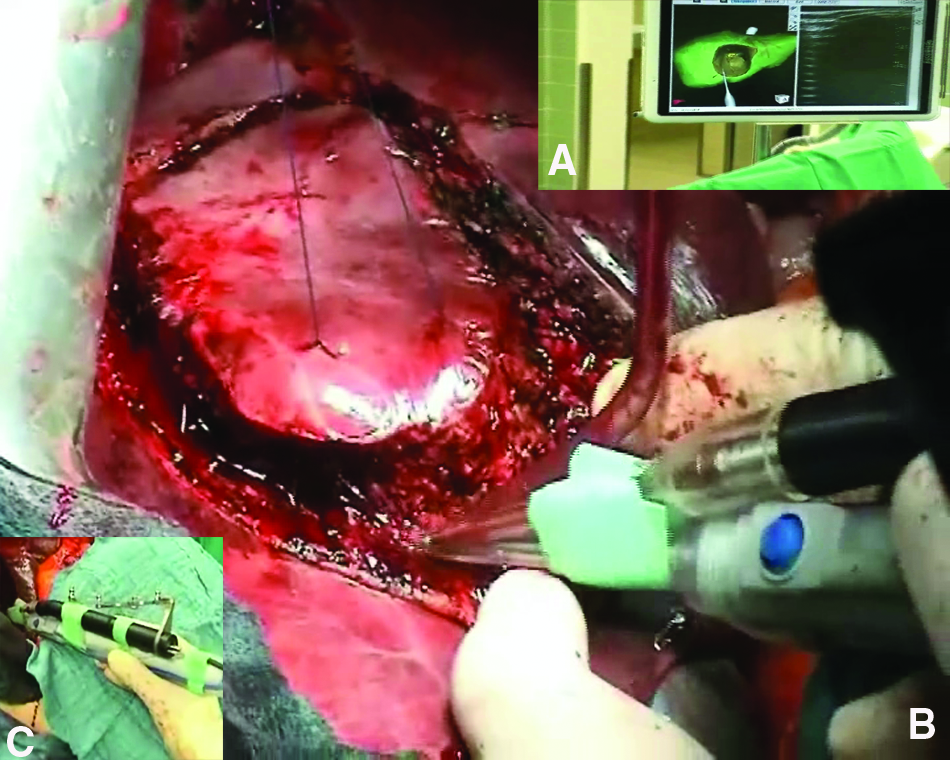

Surgeons interactively working with a three-dimensional model during a “navigated” liver resection.
Unsolved Problems
The main problems of navigation of liver resections are related to the nature of this organ; in fact, in soft tissue surgery the deformation of the organ (due to intraoperative manipulation) is a major problem because the real-time codification of such a deformation with the contemporary representation in the 3D model is very important: manipulation changes the anatomical distance between important structures (i.e., tumor, vessels) and of course the preoperative codified resection line. Thus, without the concomitant real-time deformation of the model, every element of millimetric precision is lost. Some experimental attempts were made by Markert et al. 25 in a pig model using surface fiducials communicating through the same infrared technology. Some groups are carrying out research in this direction, but knowledge and data are still at an experimental level. Another unsolved problem is related to brief movements of the liver during surgical resection: these movements produce a shift estimated in about 1 cm that additionally increases the error of localization on the map. This problem is also related to the change of anatomical elements due to liver mobilization. This problem can be overcome by recalibrating the liver model to real anatomy or by choosing fiducial points in a rigid structure (such as the hepatic vein-cava junction). Above all, the major problem of navigation methods in liver resection remains the millimetric correspondence between reconstructed anatomy and real anatomy. The middle error between the planned resection line and resection plane conducted on real liver anatomy is about 1 cm. 16 This distance is still unacceptable even under the best surgical conditions.
Indications and Perspectives
However, even with all these problems, some clinical applications of navigation in liver surgery have been published, and other fields seem to be promising for an extensive use of this technology in the future. Navigation systems in their current state can allow the resection of unidentifiable liver metastases that have disappeared after chemotherapy. 17 Local resection of lesions in the V segments without the need of liver mobilization or extensive manipulation can be navigated. Generally, central lesions with central resection lines can be navigated (extended liver resections are foreseeable as one of the future applications of such a method) as well as central resections in the presence of complex venous drainage or anatomical variants that need a “map” to be followed as a “safe” route for resection. Moreover, the emerging indication to resect recurrent metastases means that surgeons are seeing “anatomically changed livers” due to a previous operation. This anatomical alteration can sometimes lead even experienced surgeons to accidental lesions of important hilar structures (such as vessels). The distance from these “noble” structures in the near future could be safely “navigated,” reducing the intraoperative stress on surgeons, shortening resection time, and even indirectly enlarging operability/resectability of such patients. To date, after demonstrations of navigation feasibility (see the FUSION project 26 ), research is oriented toward improving overall system accuracy. Especially during the last part of resection (deep position of instruments), the accuracy of the system disappears because of major deformation, fiducial orientation, and distance. Another reported problem is the intraoperative stress on surgeons who must continuously look at the navigation video to check position and simultaneously look at the operating field. 17 Some attempts to reduce the video-dependence of surgeons and improve precision of navigation during resection have been done with optional audio feedback 27 ; therefore, in our opinion, this is one of the future research fields of navigation systems.
Conclusions
In conclusion, navigation systems for liver surgery are designed to achieve more accuracy during resection, to reduce the risk of accidental iatrogenic injuries of important anatomical structures, to guarantee a safe margin around the tumor (R0) avoiding only theoretical calculation of resting liver volume, to achieve correspondence between simulated resting liver volume and real resting liver anatomy and consequently to reduce the risk of postoperative liver failure, and finally to reduce intraoperative stress on surgeons by giving important information about anatomical orientation during resections. Some of these goals have been reached during the last 10 years, thanks to many published experimental and clinical data from research groups all over the world.
More effort must be made over the next few years to achieve more precision and resolve all the intraoperative problems in order to find the best indications and to establish navigation systems in routine clinical practice for liver resections. Considering the high costs of navigation systems, the ethical limits to clinical experimentation, and the high interdisciplinary competence required to set up and make these systems function correctly together with the potential for improved surgery, it can be easily understood why navigation systems seem to be one of the most challenging fields of surgical research.
Footnotes
Disclosure Statement
No competing financial interests exist.